Pleural cavity explanation all imp for uc exams
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a thorough exam-focused answer. Let me compile it all:
Pleural Cavity - Complete Exam Notes
Sources: Gray's Anatomy for Students, Guyton & Hall Medical Physiology, Robbins Pathology, Color Atlas of Human Anatomy
1. Definition & Basic Structure
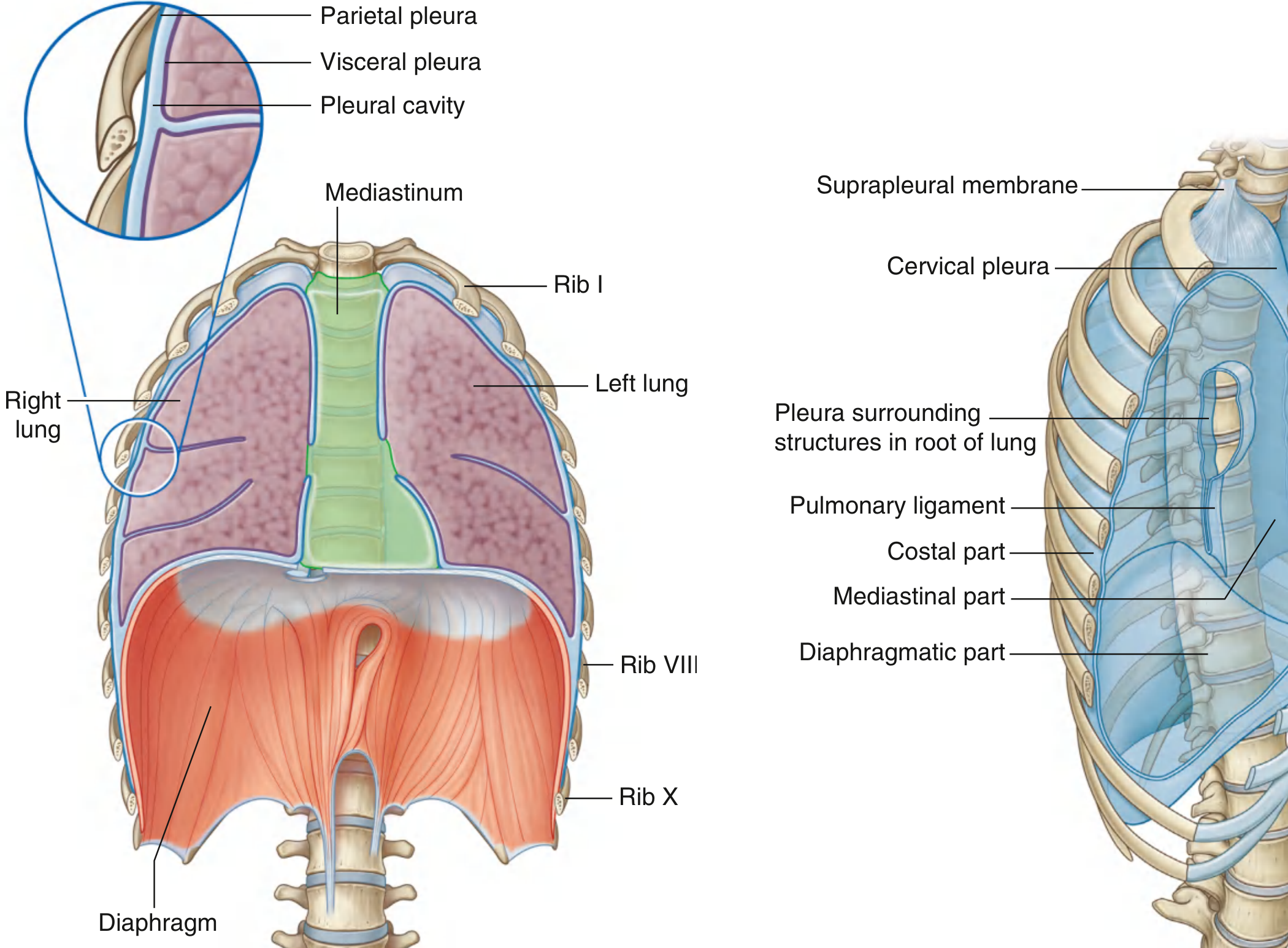
The pleural cavity is a potential space between two serous membranes - the parietal pleura and the visceral (pulmonary) pleura. It is lined by a single layer of flat cells called mesothelium plus supporting connective tissue. Normally it contains only a few milliliters (~15 mL max) of clear serous fluid that acts as a lubricant, allowing the lung to slide freely during respiration.
"Each pleural cavity is the potential space enclosed between the visceral and parietal pleurae." - Gray's Anatomy for Students
2. Types of Pleura
Visceral (Pulmonary) Pleura
- Covers the entire lung surface and dips into the interlobar fissures
- Cannot be stripped from the lung surface
- Does NOT cover the hilum or the area around the pulmonary ligament
- Innervated by visceral afferent nerves (via bronchial vessels) - NOT sensitive to pain
- Continuous with parietal pleura at the hilum
Parietal Pleura
Named by region (exam favorite!):
| Part | Location |
|---|---|
| Costal part | Lines ribs and intercostal spaces |
| Diaphragmatic part | Covers superior surface of diaphragm |
| Mediastinal part | Covers the mediastinum |
| Cervical pleura (pleural cupola) | Dome-shaped extension above first rib into the neck |
- Covered superiorly by the suprapleural membrane (attached to medial margin of rib I and transverse process of CVII) - keeps the dome taut
- Innervated by somatic afferent fibers - IS sensitive to pain
3. Nerve Supply (HIGH YIELD for exams!)
| Region | Nerve | Pain Referral |
|---|---|---|
| Costal pleura | Intercostal nerves | Thoracic wall (local) |
| Diaphragmatic pleura | Phrenic nerve (C3, C4, C5) | Lateral neck + supraclavicular shoulder region |
| Mediastinal pleura | Phrenic nerve (C3, C4, C5) | Lateral neck + supraclavicular shoulder region |
| Visceral pleura | Visceral afferents | No pain |
Mnemonic: "C3, C4, C5 keeps the diaphragm alive" - same roots innervate the diaphragmatic/mediastinal pleura.
4. Pulmonary Ligament
Below the root of the lung, the mediastinal pleura forms a double fold called the pulmonary ligament, which hangs downward from the hilum like an apron. It allows movement of structures within the lung root during breathing.
5. Pleural Recesses (Clinically Important!)
Recesses form where two layers of parietal pleura become opposed - the lung does NOT fill these spaces during quiet breathing.
Costodiaphragmatic Recess
- Between costal and diaphragmatic pleura
- Largest and most clinically important recess
- Deepest after forced expiration; shallowest after forced inspiration
- This is where pleural fluid collects first - aspiration (thoracentesis) is done here
Costomediastinal Recess
- Anteriorly between costal and mediastinal pleura
- Largest on the left side (at cardiac notch region)
6. Surface (Peripheral) Reflections of the Pleura - EXAM NUMBERS
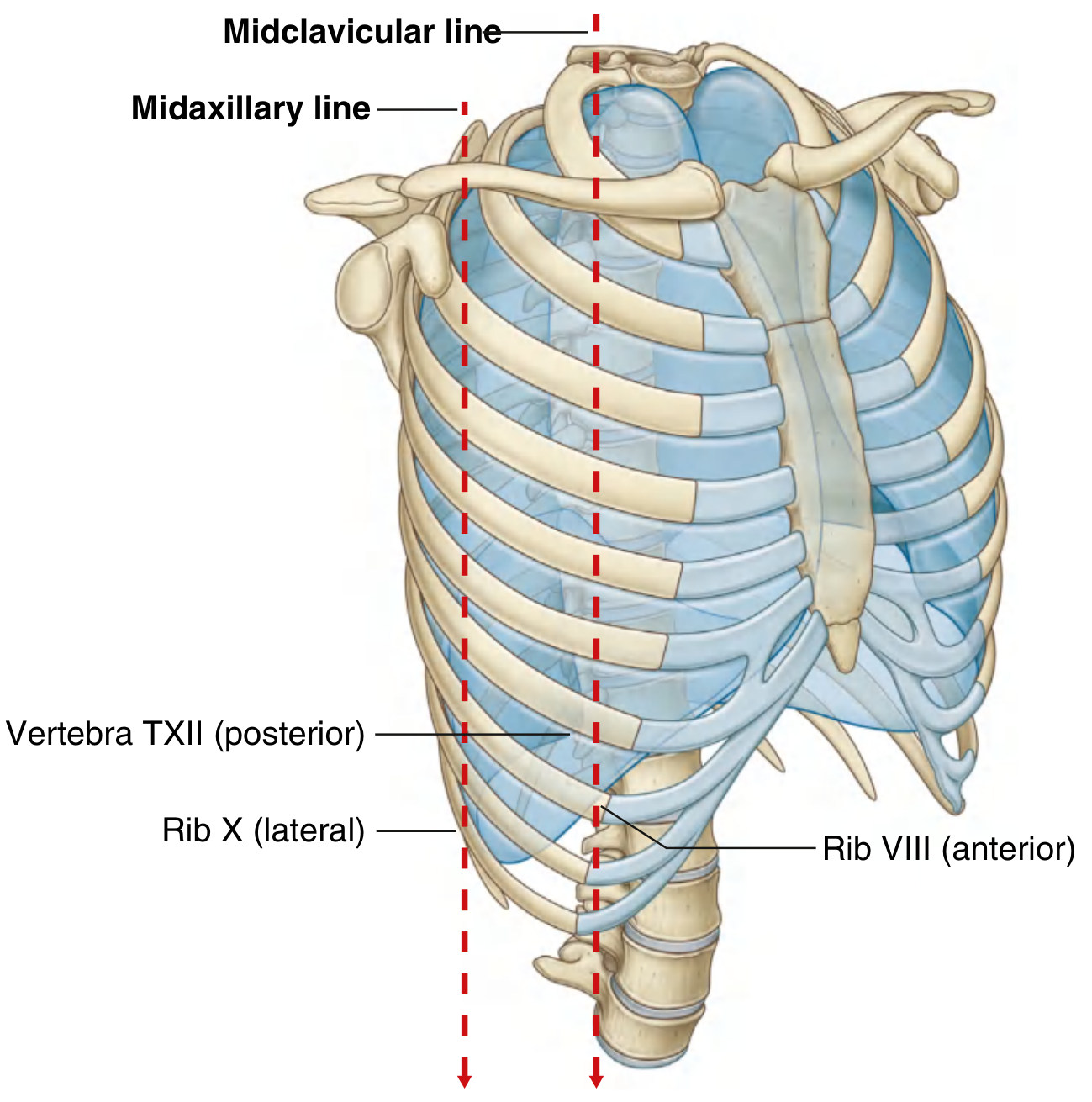
Inferior boundary of the pleural cavity:
| Reference line | Rib level |
|---|---|
| Midclavicular line | Rib VIII |
| Midaxillary line | Rib X |
| Posterior (vertebral column) | T XII |
Inferior boundary of the LUNG (during quiet respiration):
| Reference line | Rib level |
|---|---|
| Midclavicular line | Rib VI |
| Midaxillary line | Rib VIII |
| Posterior | T X |
Key rule: Lung border is always ~2 ribs higher than the pleural border. The gap between them = the costodiaphragmatic recess.
Superior extent: Pleural cavity projects 3-4 cm above the first costal cartilage into the root of the neck (but not above the neck of rib I). This is why stab wounds to the root of the neck can cause pneumothorax.
7. Pleural Fluid Physiology (Guyton & Hall)
- Normal volume: only a few milliliters per side
- Fluid continuously transudes from pleural membrane capillaries into the space
- Excess is drained by lymphatics opening into: (1) mediastinum, (2) superior surface of diaphragm, (3) lateral surfaces of parietal pleura
- Intrapleural pressure is negative (-7 mmHg) - caused by lymphatic pumping
- This negative pressure keeps the lung expanded against the chest wall
- The collapse tendency of the lungs is about -4 mmHg, so pleural pressure must be at least -4 mmHg to keep lungs open
8. Clinical Conditions (Pathology - Robbins)
Pleural Effusion
Accumulation of excess fluid in the pleural space. Causes:
| Mechanism | Example |
|---|---|
| ↑ Hydrostatic pressure | Congestive heart failure (transudate) |
| ↑ Vascular permeability | Pneumonia (exudate) |
| ↓ Osmotic pressure | Nephrotic syndrome, liver failure (transudate) |
| ↑ Intrapleural negative pressure | Atelectasis |
| ↓ Lymphatic drainage | Mediastinal carcinomatosis |
| Blockage of lymphatics | Obstruction |
Inflammatory Pleural Effusions (Pleuritis)
- Serous/serofibrinous pleuritis: TB, pneumonia, pulmonary infarction, rheumatoid arthritis, SLE, uremia, radiotherapy
- Empyema (purulent): Bacterial/fungal seeding - usually by spread from intrapulmonary infection. Yellow-green pus, masses of neutrophils. Can organize into dense fibrous adhesions obliterating the pleural space.
- Hemorrhagic pleuritis: Associated with bleeding disorders or malignancy
Pneumothorax
Air in the pleural cavity - collapses the lung. Can be spontaneous, traumatic, or tension (medical emergency).
Mesothelioma
Primary malignant tumor of the pleura - strongly associated with asbestos exposure. Most important primary pleural neoplasm.
9. Quick Summary Table for Exam
| Feature | Visceral Pleura | Parietal Pleura |
|---|---|---|
| Location | On lung surface | Lines thoracic wall |
| Pain sensitive | No | Yes |
| Nerve supply | Visceral afferents | Somatic (intercostal + phrenic) |
| Can be stripped | No | Yes |
| Blood supply | Bronchial arteries | Intercostal + internal thoracic + musculophrenic arteries |
10. High-Yield Exam Points Summary
- Pleural cavity is a potential space - normally contains only a thin film of fluid
- Costodiaphragmatic recess is the largest and most clinically important recess (site of fluid collection and thoracentesis)
- Pleural border is 2 ribs below the lung border at equivalent positions
- Phrenic nerve (C3,4,5) innervates diaphragmatic and mediastinal pleura - pain refers to shoulder/neck
- Costal pleura - pain via intercostal nerves, felt locally
- Intrapleural pressure is -7 mmHg (negative) - keeps lungs expanded
- Suprapleural membrane covers the cervical pleura dome
- Causes of effusion: heart failure (transudate), infection (exudate), malignancy, nephrotic syndrome
- Empyema = pus in pleural cavity (from bacterial spread)
- Mesothelioma = primary pleural malignancy, linked to asbestos
This is a shared conversation. Sign in to Orris to start your own chat.