Fate of Haemoglobin
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
I now have comprehensive, well-sourced information from multiple authoritative textbooks. Let me compose the full answer.
Fate of Haemoglobin
Haemoglobin (Hb) released from senescent red blood cells undergoes an orderly series of degradative steps that ultimately yield bilirubin, iron for recycling, and amino acids from globin. The pathway can be divided into five stages.
1. Source and Trigger
About 80-85% of the ~4 mg/kg/day of bilirubin produced in a healthy adult comes from the breakdown of haemoglobin in senescent red blood cells (lifespan ~120 days). The remaining 15-20% derives from:
- Premature destruction of erythroid precursors in the bone marrow ("ineffective erythropoiesis")
- Turnover of other haemoproteins: myoglobin, cytochromes, peroxidases, catalase
When RBCs age, they become less deformable and are recognised and phagocytosed by macrophages of the reticuloendothelial system (RES) - primarily in the spleen, and also in the liver and bone marrow.
(Harrison's Principles of Internal Medicine 22E; Henry's Clinical Diagnosis and Management by Laboratory Methods)
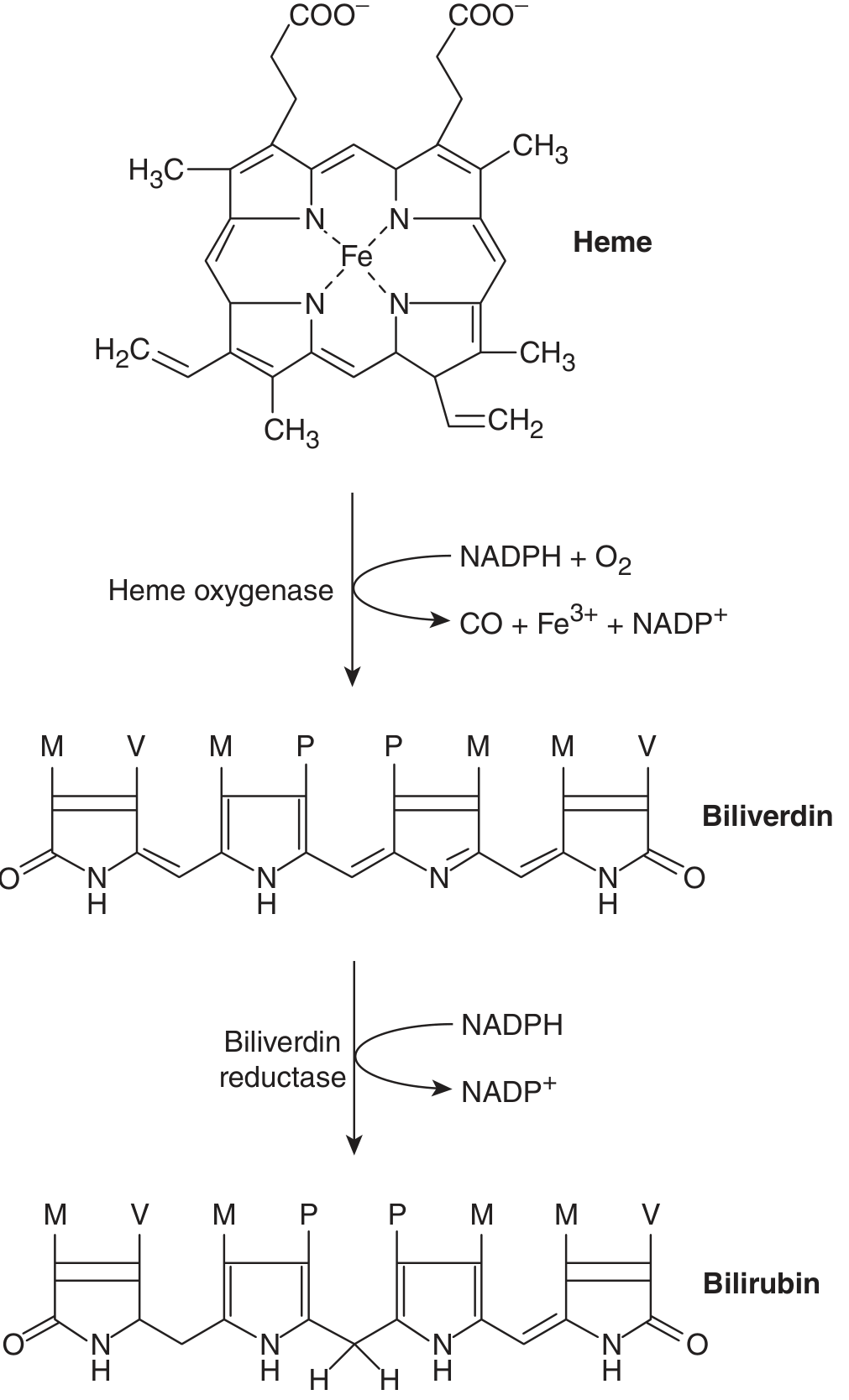
2. Breakdown of Haemoglobin to Biliverdin
Inside RES macrophages, the haemoglobin molecule is split into:
- Globin chains - returned to the amino acid pool and reutilised for protein synthesis
- Haem (ferroprotoporphyrin IX) - undergoes enzymatic degradation
The haem ring is cleaved by the microsomal enzyme heme oxygenase (requires NADPH and O₂), which oxidatively opens the alpha-methene bridge of the porphyrin ring. The products are:
| Product | Fate |
|---|---|
| Biliverdin (green, linear tetrapyrrole) | Reduced to bilirubin |
| Iron (Fe³⁺) | Released, bound to transferrin, recycled for new Hb synthesis |
| Carbon monoxide (CO) | Transported as carboxyhaeomoglobin; exhaled via lungs |
Biliverdin reductase (a cytosolic, NADPH-dependent enzyme) then reduces the central methylene bridge of biliverdin to produce unconjugated bilirubin (UCB).
(Ganong's Review of Medical Physiology 26th Ed.; Harrison's 22E)
Here is the chemical pathway:
3. Transport to the Liver
Unconjugated bilirubin (UCB) is highly insoluble in water due to tight intramolecular hydrogen bonding - the propionic acid carboxyl groups of one dipyrrolic half form bonds with the imino/lactam groups of the opposite half, burying the hydrophilic residues and exposing the hydrophobic exterior.
To be carried in aqueous plasma, UCB binds tightly and reversibly to albumin in a ~1:1 molar ratio. This albumin-bilirubin complex is transported to the liver sinusoids. The albumin itself does not enter the hepatocyte.
(Harrison's 22E; Ganong's 26th Ed.)
4. Hepatic Processing (Four Steps)
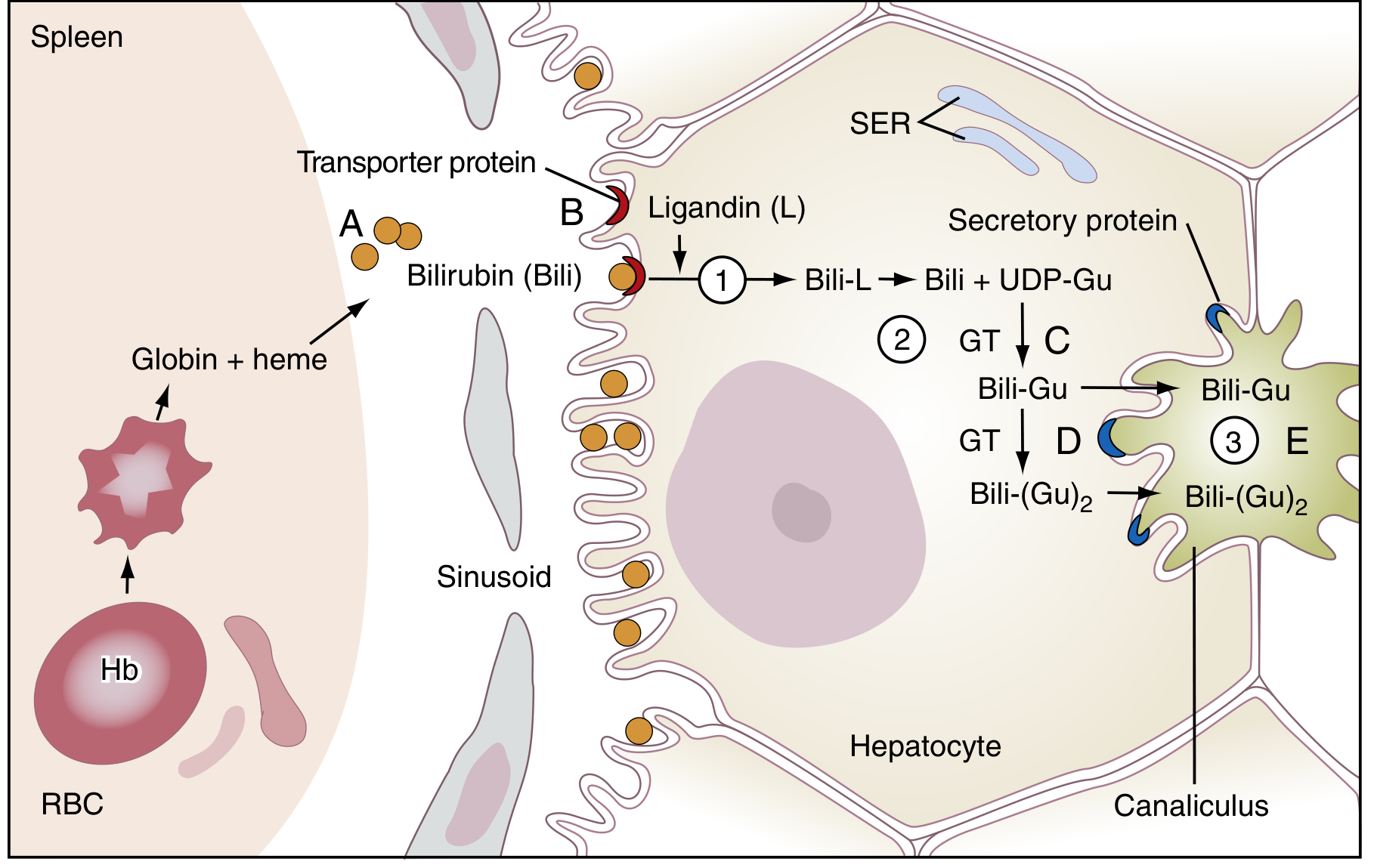
Step 1 - Hepatocellular Uptake
Albumin-bound bilirubin passes through the fenestrated sinusoidal endothelium to reach the hepatocyte. Bilirubin dissociates from albumin and enters hepatocytes via organic anion transporting polypeptides (OATPs) - carrier-mediated membrane transport (though the precise transporter remains incompletely defined). The albumin stays in the sinusoid.
Step 2 - Intracellular Binding
Inside the hepatocyte, UCB is bound by cytoplasmic proteins - the "Y" and "Z" proteins (collectively called ligandin, members of the glutathione-S-transferase superfamily). This prevents back-diffusion of bilirubin into plasma and shuttles it toward the smooth endoplasmic reticulum (SER).
Step 3 - Conjugation
In the SER, the enzyme bilirubin UDP-glucuronosyltransferase (UGT1A1) catalyses the esterification of bilirubin's propionic acid side chains with glucuronic acid (donated by UDP-glucuronic acid). This produces:
- Bilirubin monoglucuronide (BMG) - one glucuronic acid
- Bilirubin diglucuronide (BDG) - two glucuronic acids (predominant form in bile, ratio BMG:BDG in bile ~1:4)
Conjugation disrupts the internal hydrogen bonds, making bilirubin water-soluble (direct bilirubin).
Step 4 - Canalicular Secretion
Conjugated bilirubin (mostly BDG) is actively transported across the canalicular membrane into bile by the ATP-dependent transporter MRP2 (multidrug resistance-associated protein 2, also called cMOAT/ABCC2). A smaller fraction is exported back into portal sinusoids by MRP3 and can be reuptaken by adjacent hepatocytes via OATP1B1/OATP1B3 (enterohepatic circulation of conjugates).
(Harrison's 22E; Henry's; Ganong's 26th Ed.)
5. Intestinal Fate and Urobilinogen Cycle
Conjugated bilirubin passes through the bile ducts into the duodenum. The intestinal mucosa is relatively impermeable to conjugated bilirubin, so it passes unchanged through the proximal small bowel.
In the distal ileum and colon, bacterial beta-glucuronidases hydrolyse the conjugate back to UCB, and intestinal bacteria further reduce it to a group of colourless compounds called urobilinogens (d-urobilinogen, i-urobilinogen, l-urobilinogen).
From urobilinogens:
- ~10-20% are reabsorbed from the gut into the portal circulation
- Most are re-excreted by the liver (enterohepatic circulation)
- A small amount (< 4 mg/day) escapes into the systemic circulation and is excreted in urine as urobilinogen
- ~80-90% are oxidised in the colon to stercobilin (urobilin), which gives faeces their characteristic brown colour. Absence of stercobilin causes clay/pale-coloured stools (e.g., in complete bile duct obstruction).
(Harrison's 22E; Ganong's 26th Ed.; Henry's Clinical Diagnosis)
Summary Flowchart
Senescent RBC
↓ (macrophages of RES - spleen, liver, marrow)
Haemoglobin
↓
Globin → amino acids (recycled)
Haem
↓ Heme oxygenase (NADPH, O₂)
Biliverdin + CO (exhaled) + Fe²⁺ (→ transferrin → recycled)
↓ Biliverdin reductase (NADPH)
Unconjugated bilirubin (UCB)
↓ bound to albumin → transported to liver
Hepatocyte uptake (OATP)
↓
Bound to ligandin (GST) in cytosol
↓
Conjugation (UGT1A1 in SER) → Bilirubin glucuronides (BDG/BMG)
↓ MRP2
Secreted into bile canaliculi
↓
Intestine → bacterial reduction
↓
Urobilinogen
├── ~80-90%: oxidised → Stercobilin (excreted in faeces, brown colour)
└── ~10-20%: reabsorbed
├── most: liver → re-excreted in bile (enterohepatic circulation)
└── small amount → kidney → urine as urobilinogen
Clinically Relevant Points
| Defect | Consequence |
|---|---|
| Excess Hb breakdown (haemolysis) | Raised unconjugated bilirubin; urobilinogen in urine; pigment gallstones |
| UGT1A1 absent (Crigler-Najjar type I) | Severe unconjugated hyperbilirubinaemia; kernicterus |
| UGT1A1 reduced (Gilbert's syndrome) | Mild unconjugated hyperbilirubinaemia; benign |
| MRP2 deficient (Dubin-Johnson syndrome) | Conjugated bilirubin accumulates; conjugated hyperbilirubinaemia |
| Bile duct obstruction | No bilirubin in intestine → pale stools; conjugated bilirubin in urine (bilirubinuria); absent urinary urobilinogen |
| Delta-bilirubin | Conjugated bilirubin covalently bound to albumin (half-life 17 days); explains prolonged jaundice after hepatic injury even after resolution |
(Harrison's Principles of Internal Medicine 22E; Henry's Clinical Diagnosis and Management by Laboratory Methods; Ganong's Review of Medical Physiology 26th Ed.)
This is a shared conversation. Sign in to Orris to start your own chat.