Ctg
Reading File
Finding Sources
Searching the Web
cardiotocography CTG interpretation fetal heart rate monitoring
Finding Sources
Asking for Preferences
How to read ctg explain with images
Reading File
Finding Sources
Searching the Web
how to read CTG cardiotocography interpretation guide images
Reading File
Reading Web Page
how to read CTG interpretation features decelerations variability
Reading File
Loading Image
Reading File
Loading Image
Reading File
Searching the Web
CTG trace decelerations accelerations variability diagram labeled
Loading Image
Loading Image
Finding Sources
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
I now have comprehensive content from the textbook and supporting images. Let me compile the full answer.
How to Read a CTG (Cardiotocography)
A CTG trace has two channels:
- Upper channel - Fetal Heart Rate (FHR) in beats per minute (bpm)
- Lower channel - Uterine contractions (tocogram)
The CTG Strip - What You're Looking At
Here is a normal CTG: baseline ~130 bpm, good variability, no decelerations, regular contractions below.
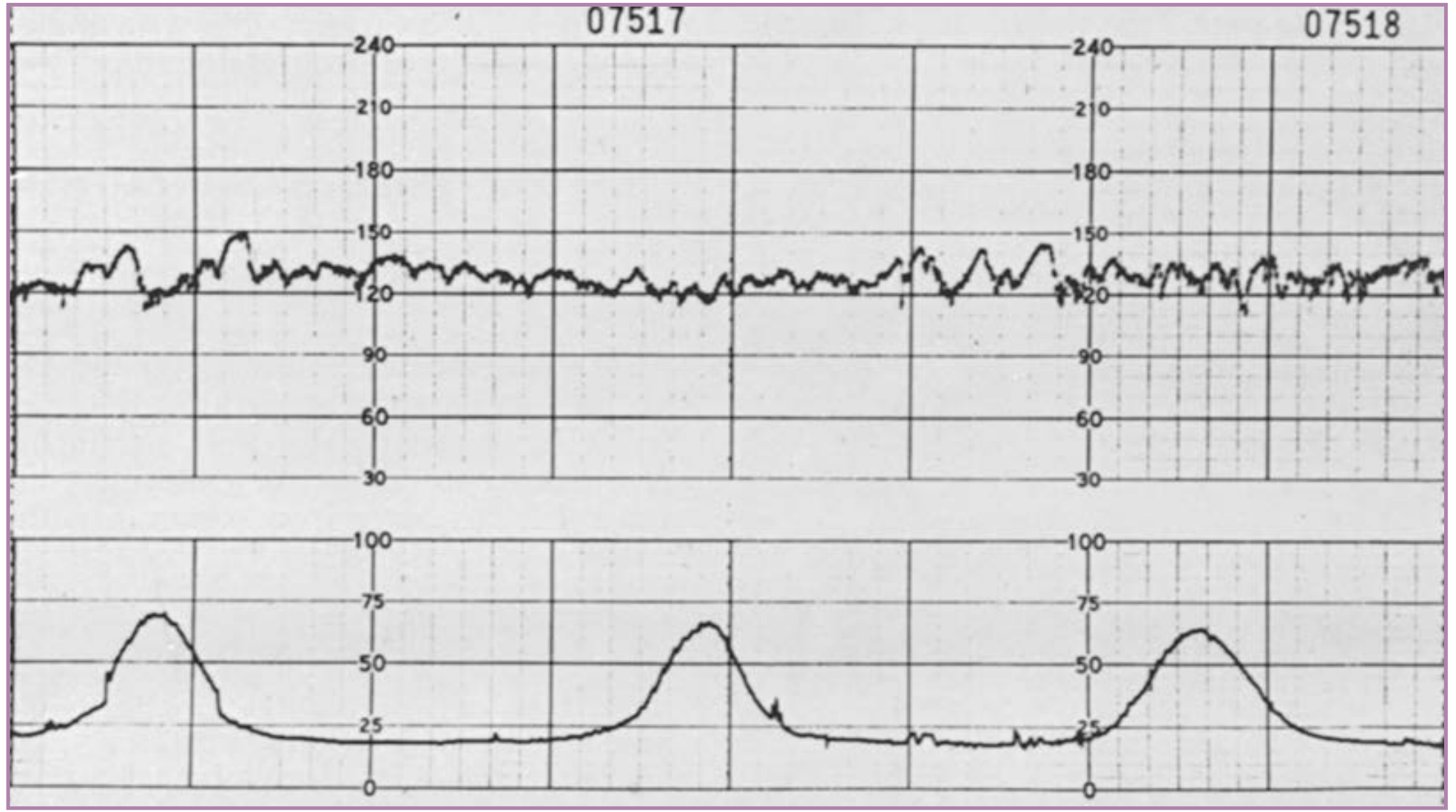
Normal FHR pattern: ~130 bpm, normal variability (~15 bpm amplitude), no periodic changes. Uterine contractions 2-3 min apart, ~60-70 mmHg intensity. - Creasy & Resnik's Maternal-Fetal Medicine
Step 1 - Baseline Fetal Heart Rate
The baseline rate is the mean FHR over a 10-minute window, excluding accelerations and decelerations.
| Finding | Rate | Significance |
|---|---|---|
| Normal | 110-160 bpm | Reassuring |
| Bradycardia | <110 bpm | Non-reassuring / Abnormal |
| Tachycardia | >160 bpm | Non-reassuring (161-180) / Abnormal (>180) |
The average FHR is around 140 bpm at term. Vagal tone maturation causes the rate to decrease progressively through gestation (155 bpm at 20 weeks → 140 bpm at term).
Step 2 - Variability
Variability refers to the normal beat-to-beat fluctuations in FHR. It reflects an intact neurological pathway from the fetal brain → vagus nerve → sinoatrial node. This is one of the most important features on the trace.
| Type | Amplitude | Meaning |
|---|---|---|
| Moderate (normal) | 6-25 bpm | Reassuring - healthy CNS |
| Minimal | 1-5 bpm | Non-reassuring (may be sleep cycle, drugs, or early hypoxia) |
| Absent | <1 bpm | Abnormal - possible acidosis |
| Marked (saltatory) | >25 bpm | Abnormal if sustained >25 min |
| Sinusoidal | Smooth sine wave, 3-6 cycles/min | Abnormal - indicates severe fetal anemia |
Causes of reduced variability: Fetal sleep (most common, up to 40 min), fetal acidosis/hypoxia, opiates/benzodiazepines, prematurity (<28 weeks), congenital heart block.
Step 3 - Accelerations
Accelerations = abrupt FHR rise >15 bpm for >15 seconds above baseline.
- Reassuring sign - indicates healthy fetal CNS activity
- Typically occur with fetal movements
- In fetuses <32 weeks, the threshold is >10 bpm for >10 seconds
- Absence of accelerations on an otherwise normal trace is of uncertain significance alone
Step 4 - Decelerations
Decelerations = drop in FHR >15 bpm for >15 seconds. They are classified by their timing relative to uterine contractions.
This diagram shows all three types compared:

Early Decelerations
- Begin with the contraction and recover when the contraction ends (mirror image)
- Caused by increased fetal intracranial pressure → vagal stimulation
- Physiological - not concerning
Variable Decelerations
- Abrupt onset and recovery (onset to nadir <30 seconds)
- Variable in shape, duration, and depth
- Not consistently related to contractions
- Caused by umbilical cord compression
- Presence of "shoulders" (small accelerations before and after) = fetus is compensating, not yet hypoxic
- Loss of shoulders = fetus becoming hypoxic - more worrying
Late Decelerations
- Begin at the peak of contraction, recover after the contraction ends
- Smooth, uniform shape
- Caused by uteroplacental insufficiency → fetal hypoxia
- Always pathological
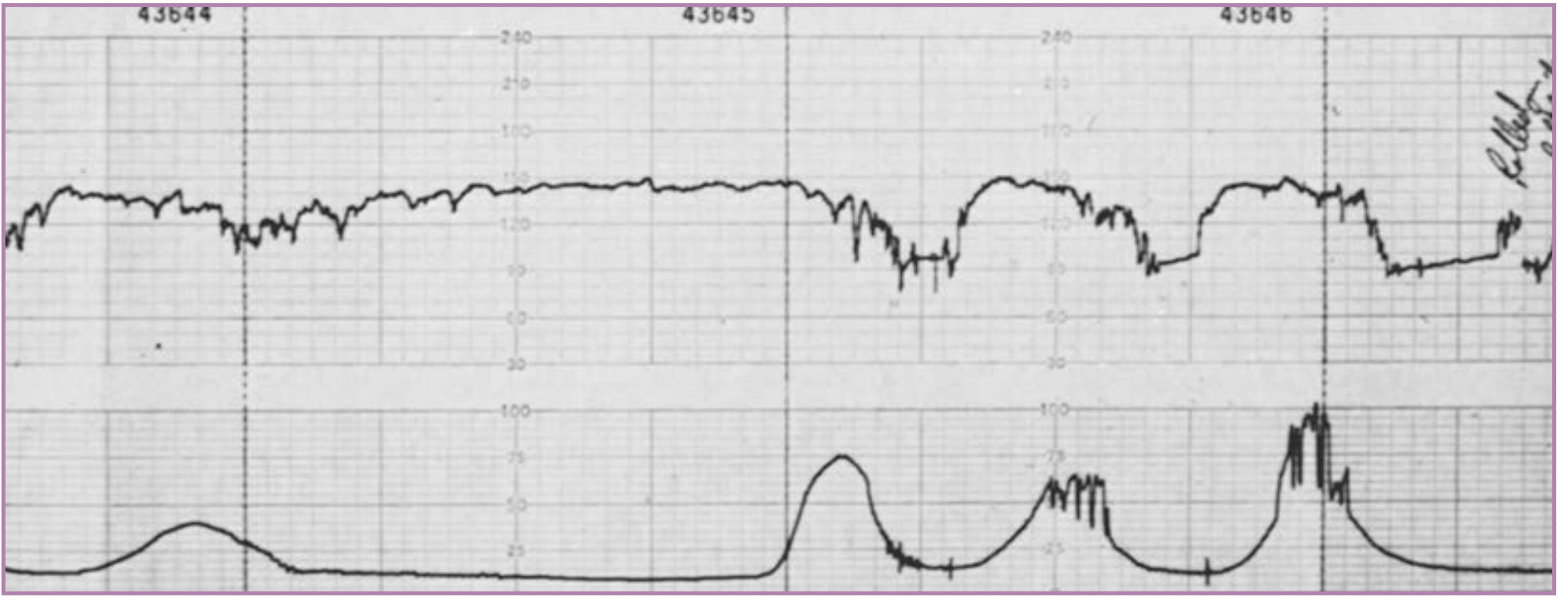
This shows reflex late decelerations on a real CTG (note FHR dips after each contraction peak):
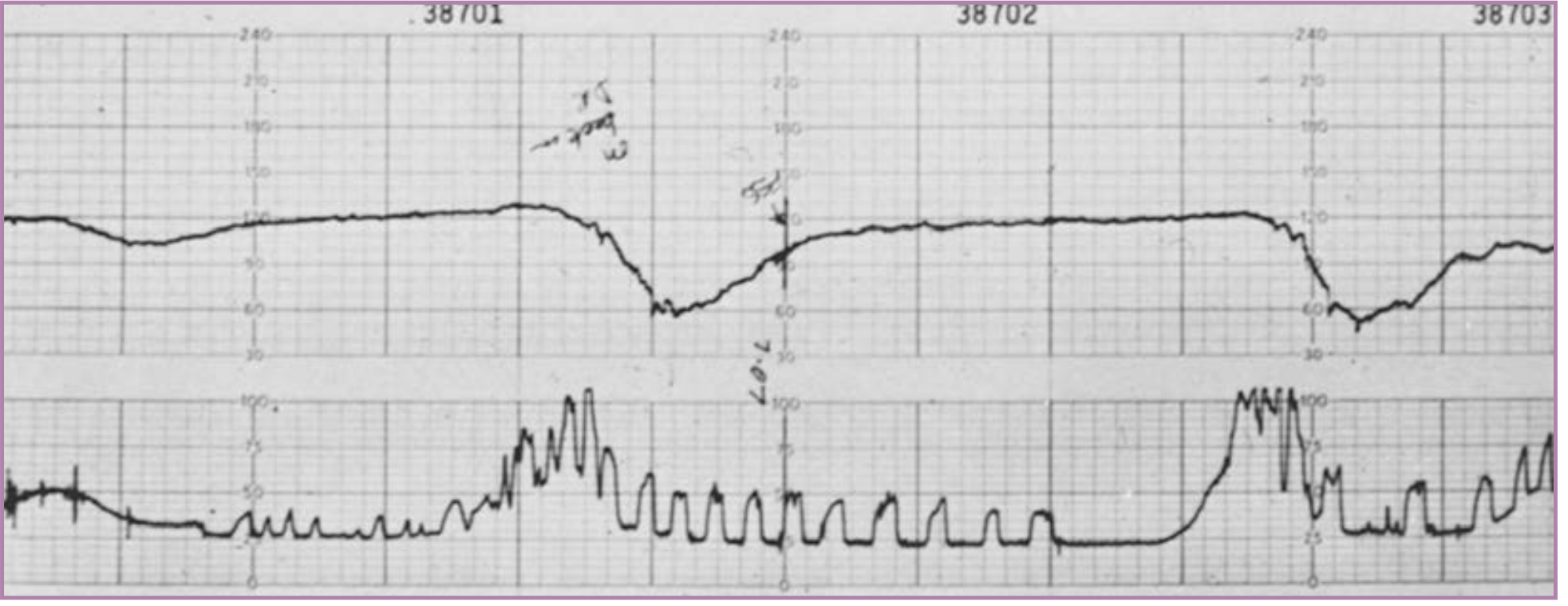
And here is non-reflex late decelerations with absent variability - the most ominous pattern (fetal scalp pH was 7.07 in this case):
Prolonged Deceleration
- FHR drop ≥15 bpm lasting ≥2 minutes but <10 minutes
- 2-3 minutes = non-reassuring
-
3 minutes = immediately abnormal (same as acute bradycardia)
Step 5 - Contractions
Assess using the tocogram (lower channel):
- Normal labour: contractions every 2-3 min, lasting ~60 seconds
- Max 5 contractions in 10 minutes
-
5 contractions in 10 min = tachysystole (oxytocin effect, reduces fetal recovery time)
Overall CTG Classification (NICHD / NICE)
Category I (Normal) - all features reassuring
- Baseline 110-160 bpm
- Moderate variability (6-25 bpm)
- No late or variable decelerations
- Accelerations present or absent
- Early decelerations present or absent
Category II (Suspicious/Indeterminate) - one non-reassuring feature
Examples: tachycardia, minimal variability, recurrent variable decelerations with moderate variability, prolonged deceleration 2-10 min, late decelerations with moderate variability.
Category III (Pathological/Abnormal) - requires immediate action
- Absent variability plus any of: recurrent late decelerations, recurrent variable decelerations, bradycardia
- Or: Sinusoidal pattern
Quick Memory Aid - "DR C BRAVADO"
| Letter | Feature |
|---|---|
| DR | Define Risk |
| C | Contractions |
| B | Baseline rate |
| R | Rhythm |
| A | Accelerations |
| V | Variability |
| A | Accelerations (confirm) |
| D | Decelerations |
| O | Overall impression |
Management by Category
| Category | Action |
|---|---|
| Normal (Cat I) | Continue monitoring |
| Suspicious (Cat II) | Correct reversible causes (position change, IV fluids, stop oxytocin, O2), fetal scalp stimulation, consider FBS |
| Pathological (Cat III) | Immediate delivery (aim within 30 minutes) |
Sources: Creasy & Resnik's Maternal-Fetal Medicine, NICE NG229 Fetal Monitoring in Labour, Creasy & Resnik's Maternal-Fetal Medicine 8e pp. 732-750.
This is a shared conversation. Sign in to Orris to start your own chat.