

provide the answer as second mbbs microbiology
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have all the information needed to answer all five questions comprehensively. Let me compile the complete answer.
Case-Based Answer: UTI Microbiology (2nd MBBS)
Case Summary: A 32-year-old female presents with dysuria and increased frequency of micturition for 2 days. Urine culture shows lactose-fermenting, non-mucoid colonies on MacConkey agar with significant bacteriuria.
Q-1: What Type of UTI Does the Patient Have?
This patient has acute uncomplicated lower UTI (Cystitis).
Classification basis:
| Feature | This Patient |
|---|---|
| Site | Lower urinary tract (bladder) |
| Symptoms | Dysuria + frequency — hallmarks of cystitis |
| Duration | 2 days (acute) |
| Host | Young adult female, community-acquired |
| Structural abnormality | None mentioned |
Types of UTI by anatomical site:
- Lower UTI → Cystitis (bladder), urethritis
- Upper UTI → Pyelonephritis (kidney/renal pelvis)
This patient has no fever, no flank pain, no costovertebral tenderness — symptoms characteristic of pyelonephritis. She has classic lower tract symptoms only, making this acute uncomplicated cystitis.
Symptoms of cystitis: frequency, urgency, dysuria, suprapubic pain, occasionally gross hematuria. Fever is uncommon in simple cystitis. — Tintinalli's Emergency Medicine
Q-2: What is Significant Bacteriuria?
Significant bacteriuria is defined as the presence of ≥10⁵ CFU/mL (colony forming units per milliliter) of a single organism in a properly collected midstream clean-catch urine sample — indicating true infection rather than contamination.
Key thresholds (Kass criteria):
| Colony Count | Interpretation |
|---|---|
| ≥ 10⁵ CFU/mL | Significant bacteriuria (symptomatic or asymptomatic) |
| ≥ 10³ CFU/mL | Significant in symptomatic young women with Gram-negative rods |
| ≥ 10³ CFU/mL | Significant in catheter-associated UTI (CAUTI) |
| < 10³ CFU/mL | Likely contamination |
"It is generally accepted that 10⁵ or more CFU/mL of urine is significant bacteriuria, though the patients may be symptomatic or asymptomatic. Some young women have dysuria and other symptoms of cystitis with less than 10⁵ CFU/mL of urine; in these women, as few as 10³ CFU/mL of a Gram-negative rod may be significant bacteriuria." — Jawetz, Melnick & Adelberg's Medical Microbiology, 28th Ed.
Why it matters: Counts below threshold usually represent urethral/perineal contamination during collection. The threshold was first proposed by Kass (1956) to differentiate bladder bacteriuria from contamination.
Q-3: Which Organism is Probably Responsible?
The most likely organism is Escherichia coli (E. coli).
Evidence from the case:
- Lactose fermenting colonies → pink/red colonies on MacConkey agar (E. coli ferments lactose, producing acid that turns the pH indicator red/pink)
- Non-mucoid colonies → distinguishes from Klebsiella pneumoniae (which produces mucoid/viscous colonies due to a thick polysaccharide capsule)
- Young adult female with community-acquired acute cystitis → classic E. coli setting
"E. coli causes 80–90% of acute uncomplicated bacterial lower tract infections (cystitis) in young women." — Jawetz, Melnick & Adelberg's Medical Microbiology
Common uropathogens in uncomplicated UTI:
| Organism | Frequency | MacConkey appearance |
|---|---|---|
| E. coli | 75–85% | Pink, non-mucoid colonies |
| Staphylococcus saprophyticus | 5–15% | Does not grow on MacConkey |
| Klebsiella pneumoniae | ~5% | Pink, mucoid colonies |
| Enterococcus faecalis | ~5% | Small pink colonies |
Virulence factors of uropathogenic E. coli:
- Type 1 fimbriae — bind to uroepithelial cells
- P fimbriae (Pap pili) — bind to P blood group antigen on uroepithelium; associated with pyelonephritis
- Haemolysin — lyses RBCs
- Aerobactin — iron acquisition
- K antigen (capsule) — antiphagocytic
Q-4: What is Complicated UTI?
Complicated UTI is defined as a urinary tract infection occurring in a patient with a functional or anatomically abnormal urinary tract, or in the presence of comorbidities that place the patient at risk for more serious adverse outcomes.
"Complicated UTI is infection involving a functional or anatomically abnormal urinary tract or infection in the presence of comorbidities that place the patient at risk for more serious adverse outcomes." — Tintinalli's Emergency Medicine
Risk Factors for Complicated UTI:
| Risk Factor | Example |
|---|---|
| Male sex | Any UTI in males is considered complicated |
| Structural/anatomic abnormality | Nephrolithiasis, polycystic kidneys, neurogenic bladder |
| Foreign body in urinary tract | Indwelling catheter, ureteral stent |
| Pregnancy | Physiological changes predispose to ascending infection |
| Diabetes mellitus | Impaired immunity |
| Immunosuppression | AIDS, chemotherapy, steroids |
| Advanced age (men) | Prostatic hypertrophy, recent instrumentation |
| Spinal cord injury | Neurogenic bladder, chronic catheterization |
| Resistant organisms | E.g., ESBL-producers, fluoroquinolone-resistant strains |
| Nursing home residency | With/without catheter |
Microbiology of complicated UTI (broader spectrum than uncomplicated):
- E. coli (still most common)
- Enterococcus spp.
- Klebsiella pneumoniae
- Pseudomonas aeruginosa
- Proteus mirabilis
- Candida spp.
- Staphylococcus aureus
- Often polymicrobial and with antimicrobial resistance
Uncomplicated vs. Complicated UTI:
| Feature | Uncomplicated | Complicated |
|---|---|---|
| Host | Healthy, premenopausal, non-pregnant female | Male, pregnancy, structural abnormality, comorbidity |
| Pathogen | Mostly E. coli | Broader, more resistant |
| Treatment | Short course oral antibiotics | Longer course, culture-guided, often parenteral |
| Risk of treatment failure | Low | Higher |
Q-5: Treatment of Community-Acquired UTI
A. Uncomplicated Cystitis (as in this patient)
First-line agents (preferred for their efficacy, short-course effectiveness, and minimal impact on normal flora):
| Drug | Dose & Duration |
|---|---|
| Nitrofurantoin (macrocrystal) | 100 mg TDS × 5 days |
| Trimethoprim-sulfamethoxazole (TMP-SMX) | 800/160 mg BD × 3 days (only if local resistance <20%) |
| Fosfomycin | 3 g single oral dose |
| Pivmecillinam | 400 mg BD × 3–7 days |
"Nitrofurantoin (100 mg three times daily for 5 days) is associated with the fewest adverse effects and results in a significantly higher likelihood of clinical and microbiological resolution." — Goldman-Cecil Medicine
Symptomatic relief: Phenazopyridine 100 mg TDS for up to 2 days (urinary analgesic — turns urine orange; use with antibiotics only).
Drugs to avoid as first-line:
- Fluoroquinolones (ciprofloxacin) — not recommended first-line due to toxicity concerns and resistance promotion; reserved for pyelonephritis/complicated UTI
- Amoxicillin alone — high resistance rates
B. Acute Uncomplicated Pyelonephritis
| Severity | Drug | Duration |
|---|---|---|
| Mild–moderate (oral) | Ciprofloxacin 500 mg BD | 5–7 days |
| TMP-SMX 960 mg BD | 14 days | |
| Cefixime 400 mg OD | 14 days | |
| Severe (IV → oral stepdown) | Gentamicin IV → oral | 10–14 days |
| Ceftriaxone IV → oral | 7–14 days |
Note: Nitrofurantoin and fosfomycin are NOT suitable for pyelonephritis (do not achieve adequate renal tissue concentrations).
C. Complicated UTI
- Culture-guided therapy is essential
- Empiric IV options for severe cases: piperacillin-tazobactam, meropenem, plazomicin
- Duration: 7–14 days depending on clinical response
- Address underlying anatomical/structural abnormality
D. Special Situations
Pregnancy: Nitrofurantoin or oral cephalosporins (cephalexin) are preferred. TMP-SMX: avoid in 1st trimester (teratogenic) and 3rd trimester (neonatal kernicterus). Screen all pregnant women at 12–16 weeks for asymptomatic bacteriuria.
Summary for the Case Patient:
| Answer | |
|---|---|
| Type of UTI | Acute uncomplicated lower UTI (cystitis) |
| Significant bacteriuria | ≥10⁵ CFU/mL on culture |
| Causative organism | Escherichia coli (lactose fermenter, non-mucoid) |
| Complicated UTI | UTI with structural/functional abnormality or comorbidity |
| Treatment | Nitrofurantoin 100 mg TDS × 5 days (first-line) |
Sources: Jawetz, Melnick & Adelberg's Medical Microbiology 28th Ed.; Tintinalli's Emergency Medicine; Goldman-Cecil Medicine; Campbell-Walsh Urology

microbiology second mbbs
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
I now have all the information needed. Let me compile the complete answer.
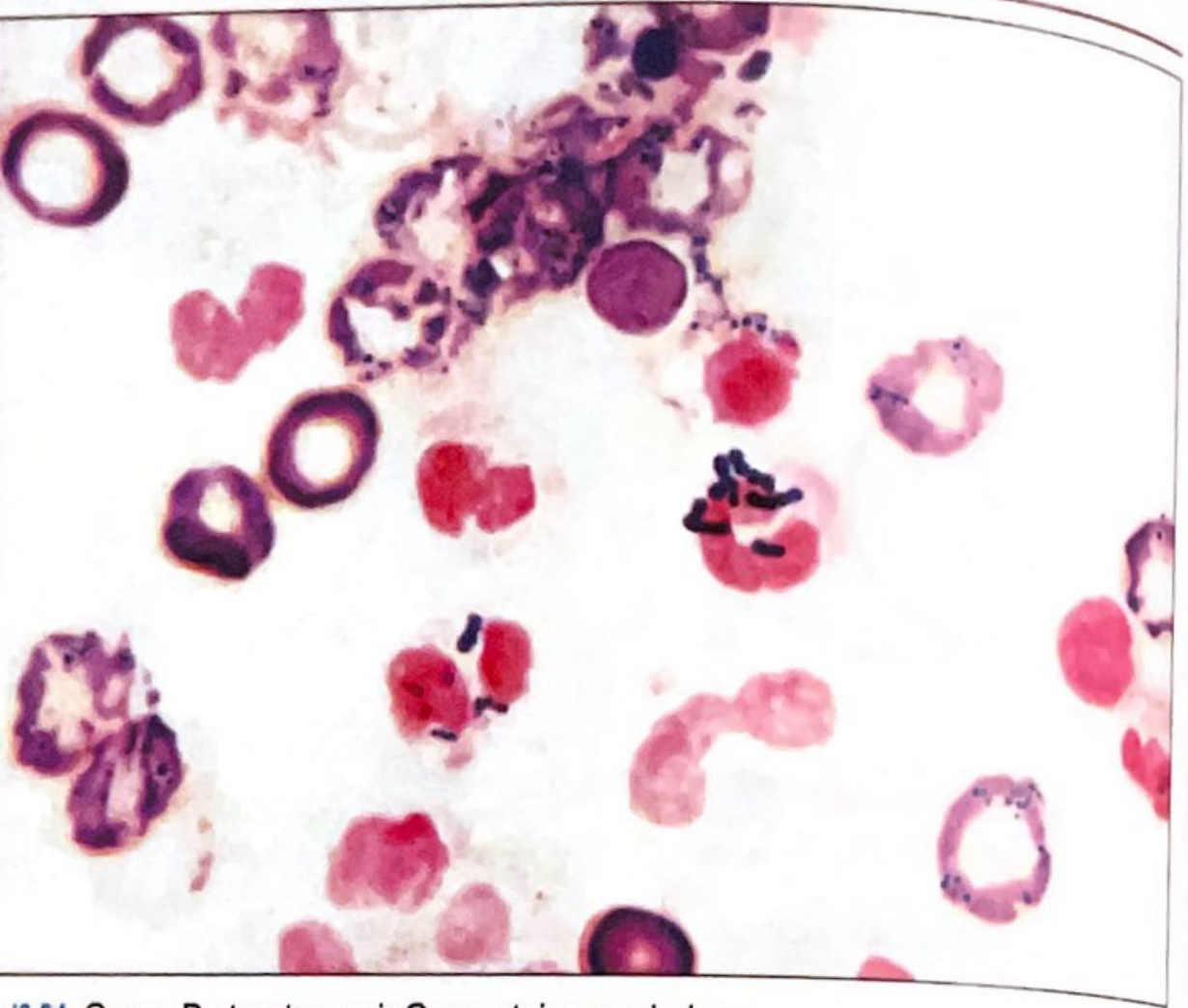
Q1: Gram Stained Smear from CSF of Newborn with Meningitis
(a) Description of the Gram Stained Smear
Looking at the image provided:
The smear shows:
- Gram-positive cocci (staining dark blue/violet) arranged in short chains and pairs
- Background shows pink-staining RBCs and leucocytes (inflammatory cells)
- Organisms are small, round cocci in characteristic chain arrangements
Microbiological Description:
| Feature | Findings |
|---|---|
| Gram reaction | Gram-positive (blue/violet) |
| Shape | Cocci (spherical) |
| Arrangement | Pairs (diplococci) and short chains |
| Size | Medium-sized |
| Background cells | Neutrophils/leucocytes (inflammatory cells) — consistent with bacterial meningitis |
| Capsule | Not visible on Gram stain (requires India ink or capsular staining) |
Identification: This is Streptococcus agalactiae (Group B Streptococcus / GBS) — the most common cause of neonatal meningitis.
"Streptococcus agalactiae — Gram-positive cocci singly, in pairs and short chains. Neonatal sepsis, pneumonia, and meningitis due to colonization of the maternal genital tract." — Quick Compendium of Clinical Pathology, 5th Ed.
Other key features on culture (not seen in Gram stain but important for ID):
- β-hemolysis (narrow zone — may need to lift colony to see it)
- CAMP test positive — GBS CAMP factor enhances the hemolytic zone of S. aureus
- Hippurate hydrolysis positive
- Bacitracin resistant (unlike Group A Strep)
(b) Route of Infection
GBS causes two distinct forms of neonatal infection depending on the timing and route:
1. Early-Onset Disease (≤6 days of birth; most common ≤24 hrs)
Route: Vertical / Intrapartum transmission
| Step | Mechanism |
|---|---|
| Source | Maternal vaginal/rectal colonization with GBS (15–40% of women) |
| Transmission | Ascending infection from colonized birth canal during labor |
| Portal of entry | Aspiration of infected amniotic fluid or vaginal secretions during passage through birth canal |
| Pathogenesis | Bacteremia → hematogenous spread → Blood-brain barrier penetration → meningitis |
Clinical features: Respiratory distress, sepsis, meningitis — presents within hours to 6 days of birth.
Risk factors for early-onset:
- Prolonged rupture of membranes (>18 hours)
- Premature labor (<37 weeks)
- Maternal fever during labor (≥38°C)
- Previous infant with GBS infection
- GBS bacteriuria in current pregnancy
2. Late-Onset Disease (>7 days to 3 months)
Route: Horizontal / Nosocomial or community transmission
| Step | Mechanism |
|---|---|
| Source | Colonized mother (breast milk, skin contact), hospital environment, or community contact |
| Transmission | Post-natal horizontal transmission |
| Dominant presentation | Bacteremia with meningitis (meningitis more prominent in late-onset than early-onset) |
"Early-onset neonatal disease: within 7 days of birth, infected newborns develop signs and symptoms of pneumonia, meningitis, and sepsis. Late-onset neonatal disease: more than 1 week after birth, neonates develop signs and symptoms of bacteremia with meningitis." — Medical Microbiology, 9th Ed.
Summary Diagram of Route
Maternal GBS colonization (vagina/rectum/GI tract)
↓ [Intrapartum / ascending]
Birth canal → Amniotic fluid contamination
↓ [Neonatal aspiration/aspiration]
Neonatal lung / nasopharynx / GI tract
↓ [Bacteremia]
Bloodstream
↓ [Blood-brain barrier penetration]
MENINGITIS (CSF — Gram-positive cocci in chains)
Prevention
- Screen all pregnant women at 35–37 weeks with vaginal + rectal swabs for GBS
- If positive → Intrapartum IV Penicillin G (5 million units loading, then 3 million units every 4 hours) during labor
- Alternative: IV Ampicillin (penicillin-allergic patients: clindamycin or vancomycin)
Treatment of Established Neonatal GBS Meningitis
- IV Penicillin G (400,000 units/kg/day) — drug of choice, for 10–14 days
- + Gentamicin (synergistic) — especially for meningitis and severe infections
- Alternative: Ceftriaxone or Vancomycin (if penicillin-allergic)
Sources: Goldman-Cecil Medicine; Medical Microbiology 9th Ed. (Murray); Quick Compendium of Clinical Pathology 5th Ed.; Jawetz, Melnick & Adelberg's Medical Microbiology 28th Ed.; Miller's Anesthesia

microbiology 2nd mbbs
Finding Sources
Finding Sources
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.