Tell me treatment for hypocalcemia
Reading File
Finding Sources
Searching PubMed
hypocalcemia treatment management
Reading File
Reading File
Reading File
Finding Sources
I have comprehensive information from three authoritative textbooks. Here is the full treatment guide for hypocalcemia:
Treatment of Hypocalcemia
Classification by Severity
Before treating, hypocalcemia is broadly classified as:
- Acute / symptomatic - medical emergency (tetany, seizures, laryngospasm, QT prolongation, cardiac arrhythmia)
- Chronic / asymptomatic - managed with oral supplementation
1. Acute Symptomatic Hypocalcemia (Emergency Treatment)
Symptomatic hypocalcemia is a medical emergency requiring IV calcium immediately.
IV Calcium Options
| Preparation | Volume | Elemental Ca²⁺ |
|---|---|---|
| Calcium gluconate 10% | 10-20 mL | ~93 mg per 10 mL |
| Calcium chloride 10% | 3-5 mL | ~272 mg per 10 mL |
Calcium gluconate is preferred for peripheral IV access - it is less irritating to veins.
Calcium chloride contains ~3x more elemental calcium per mL but is reserved for cardiac arrest / CPR due to pain and risk of vein sclerosis with peripheral infusion.
Dosing Protocol
- Initial bolus: Calcium gluconate 10-20 mL (10%) IV over 10 minutes with continuous ECG monitoring (watch QT interval).
- In children: calcium gluconate 1-2 mL/kg at <1 mL/min
- If symptoms persist (tetany, seizures): repeat the bolus as needed.
- Maintenance infusion: Elemental calcium 1-2 mg/kg/hour (continuous IV infusion) until serum calcium normalizes.
Key Precautions
- Do not give IV calcium with bicarbonate- or phosphate-containing solutions (risk of precipitation).
- Do not give IV calcium in severe hyperphosphatemia (risk of ectopic calcium-phosphate deposition).
- Monitor serial ionized calcium levels throughout treatment.
- Watch for extravasation - calcium-containing fluids cause tissue necrosis.
- Avoid alkalosis - it further reduces ionized calcium.
2. Chronic / Asymptomatic Hypocalcemia
Oral supplementation is the standard approach - IV is not indicated unless the patient is symptomatic.
Oral Calcium
- Calcium carbonate is the most common oral supplement (1250 mg calcium carbonate = 500 mg elemental calcium).
- Start with 1-2 g of elemental calcium three times daily, given away from meals to maximize absorption.
Vitamin D / Calcitriol
- Calcitriol (active vitamin D) significantly improves calcium absorption from the gut.
- Start at 0.25 mcg twice daily and titrate up.
- For vitamin D deficiency (e.g., rickets), oral vitamin D 1000-2000 IU daily for 4 weeks with elemental calcium 40 mg/kg/day.
Diuretic Adjustment
- If the patient is on loop diuretics, consider switching to thiazide diuretics - thiazides reduce urinary calcium excretion, helping retain calcium.
3. Treat Underlying Causes
Hypocalcemia often has a correctable underlying cause:
| Cause | Specific Treatment |
|---|---|
| Hypomagnesemia | Treat first with magnesium sulfate IV (0.1-0.2 mL/kg of 50% solution) - hypocalcemia will not correct until Mg²⁺ is normalized |
| Hypoparathyroidism | Calcitriol + calcium supplementation long-term |
| Vitamin D deficiency | Cholecalciferol or ergocalciferol + calcium |
| Pseudohypoparathyroidism | Calcitriol + calcium (PTH resistance) |
| Post-thyroidectomy / parathyroid surgery | IV calcium initially, then oral calcitriol + calcium carbonate |
| Hyperphosphatemia | Low-phosphate diet, phosphate binders; volume expansion if acute |
| Rapid blood transfusion | IV calcium (citrate in blood products chelates Ca²⁺) |
Important: Check serum magnesium in all cases of hypocalcemia. Hypomagnesemia impairs PTH secretion and causes PTH resistance - calcium will not rise until magnesium is corrected.
4. Monitoring During Treatment
- Fasting total and ionized serum calcium - check regularly
- Serum phosphate - monitor for reciprocal changes
- 24-hour urine calcium - keep below 4 mg/kg/day to prevent hypercalciuria and nephrocalcinosis
- Spot urine calcium-to-creatinine ratio - useful for outpatient monitoring
- PTH level - if hypocalcemia is not due to PTH deficiency
- Serum magnesium - at least annually in chronic cases
5. Anesthetic Considerations
- Correct significant hypocalcemia before elective surgery.
- Monitor ionized calcium intraoperatively in patients with known hypocalcemia.
- Avoid alkalosis intraoperatively (decreases ionized Ca²⁺).
- IV calcium may be needed after rapid transfusion of citrated blood products or large albumin volumes.
- Expect potentiation of negative inotropic effects of anesthetic agents.
- Responses to neuromuscular blocking agents are inconsistent - use nerve stimulator monitoring.
Sources:
- Brenner and Rector's The Kidney, 2-Volume Set
- National Kidney Foundation Primer on Kidney Diseases, 8e
- Morgan and Mikhail's Clinical Anesthesiology, 7e
Tell me for orally med
Based on what was already retrieved from the textbooks, here is a focused summary of oral medications for hypocalcemia:
Oral Treatment of Hypocalcemia
Oral therapy is used for chronic or asymptomatic hypocalcemia. Symptomatic patients always need IV calcium first.
1. Oral Calcium Supplements
Calcium Carbonate (most common)
- Dose: 1-2 g of elemental calcium, 3 times daily
- Note: 1250 mg calcium carbonate = 500 mg elemental calcium
- Take away from meals to maximize absorption
- Preferred as first-line oral supplement
Calcium Chloride
- Generally not used orally - reserved for IV use only (causes vein sclerosis and pain even via IV peripheral routes)
2. Vitamin D Preparations (co-administered with calcium)
Calcitriol (1,25-dihydroxyvitamin D - active form)
- Dose: Start at 0.25 mcg twice daily, titrate up as needed
- Significantly increases gut calcium absorption
- Preferred in hypoparathyroidism and renal disease (kidney cannot activate vitamin D)
Cholecalciferol / Ergocalciferol (Vitamin D3 / D2)
- Used when the cause is nutritional vitamin D deficiency
- Dose: 1000-2000 IU daily for 4 weeks (for vitamin D deficiency rickets)
- Requires hepatic and renal activation - not suitable when these organs are impaired
3. Diuretic Adjustment
- Switch from loop diuretics (furosemide - increases urinary Ca²⁺ loss) to thiazide diuretics (reduce urinary calcium excretion)
- This is an adjunct measure, not a direct calcium supplement
4. Oral Magnesium (if hypomagnesemia is present)
- Hypomagnesemia must be corrected alongside calcium - oral or IV magnesium sulfate
- Without correcting Mg²⁺, calcium levels will not normalize regardless of supplementation
Quick Reference Table
| Drug | Dose | Indication |
|---|---|---|
| Calcium carbonate | 1-2 g elemental Ca, TID away from meals | Chronic hypocalcemia (all causes) |
| Calcitriol | 0.25 mcg BID, titrate up | Hypoparathyroidism, CKD, vitamin D resistance |
| Cholecalciferol (D3) | 1000-2000 IU/day | Nutritional vitamin D deficiency |
| Thiazide diuretic | As per standard dosing | Adjunct - reduce urinary Ca²⁺ loss |
| Oral magnesium | As per Mg deficit | If concurrent hypomagnesemia |
Sources: National Kidney Foundation Primer on Kidney Diseases, 8e; Brenner and Rector's The Kidney, 2-Volume Set; Morgan and Mikhail's Clinical Anesthesiology, 7e
Urticaria treatment
Reading File
Finding Sources
Searching PubMed
urticaria treatment management
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive treatment guide for urticaria:
Treatment of Urticaria
Step 1 - Identify and Remove the Trigger
Always the first step. Avoid the inciting agent (drugs, foods, physical stimuli, NSAIDs, infections). Without trigger removal, pharmacological treatment has limited effect.
Treatment Algorithm (EAACI & American Guidelines)
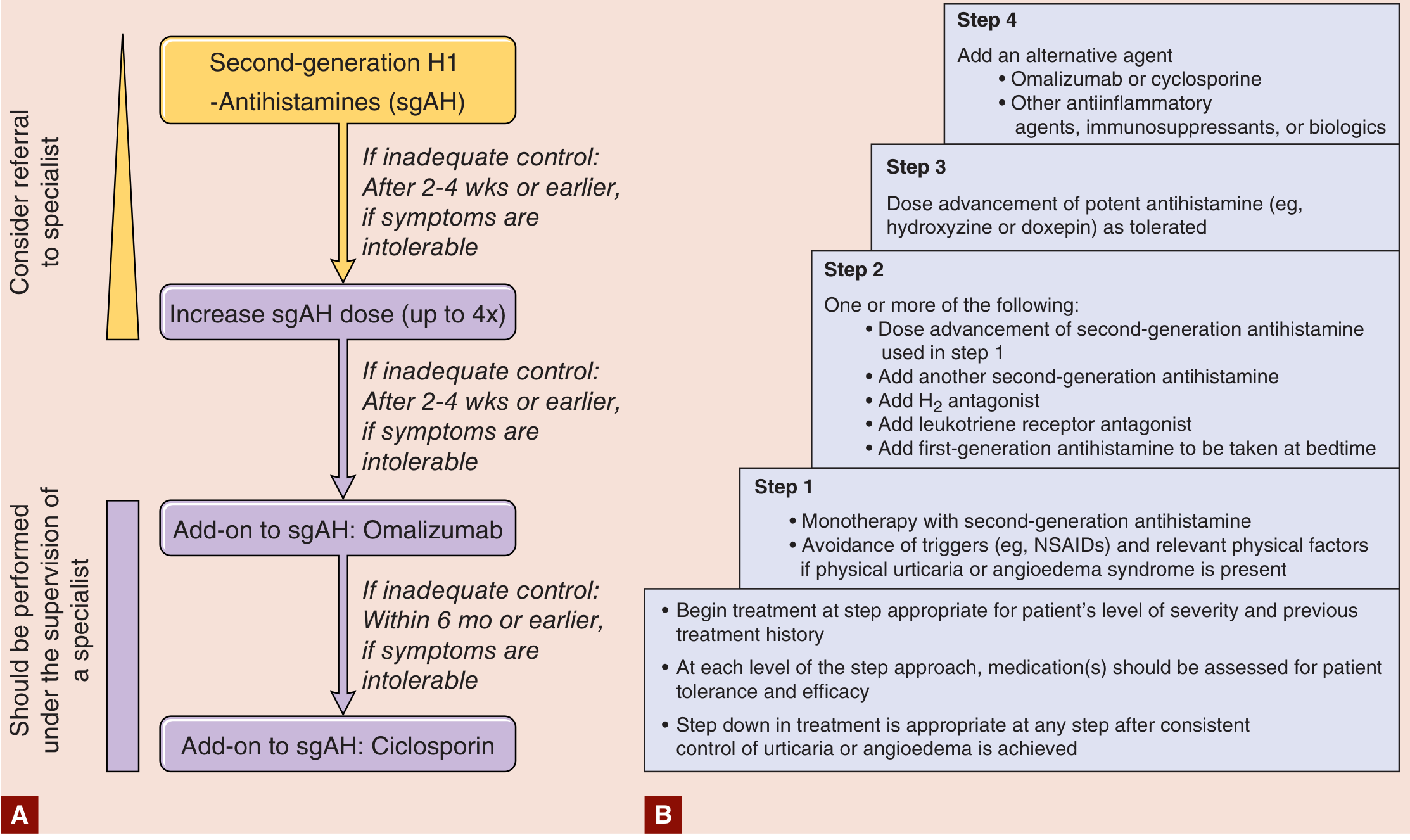
Figure: Stepwise treatment algorithm for urticaria (A = EAACI guideline; B = American Academy of Allergy, Asthma and Immunology)
A. Mild to Moderate Acute Urticaria
First-Generation H1 Antihistamines (sedating)
| Drug | Dose |
|---|---|
| Diphenhydramine | 25-50 mg PO every 4-6 hours |
| Hydroxyzine | 10-25 mg PO every 6 hours |
Second-Generation H1 Antihistamines (non-sedating - preferred)
| Drug | Dose |
|---|---|
| Cetirizine | 5-10 mg/day |
| Levocetirizine | 2.5-5 mg/day |
| Fexofenadine | 180 mg/day |
| Loratadine | 10 mg/day |
Second-generation antihistamines are preferred for long-term use due to better tolerability and no sedation.
B. Severe Urticaria with or without Angioedema
- H1 antihistamines: Diphenhydramine 25-50 mg PO q4-6h, or 10-50 mg IV/IM q4-6h (max 400 mg/24 hours)
- Corticosteroids:
- Prednisone 10-60 mg PO every morning with taper over 2 weeks
- Triamcinolone 40-60 mg IM single dose
- Dexamethasone 4-20 mg/day IV or IM
C. Anaphylaxis (most severe)
Managed as an emergency (ABC approach):
- Airway: Intubation if needed
- Breathing: Supplemental oxygen
- Circulation: Epinephrine 1:1000 IV + volume expanders (saline)
- IV methylprednisolone 1-2 mg/kg/day
- H1 + H2 antagonists IV: Diphenhydramine 25-50 mg + Famotidine 20 mg IV
D. Chronic Idiopathic / Spontaneous Urticaria (CSU) - Stepwise Approach
Step 1 - Monotherapy
- Second-generation antihistamine (cetirizine 10 mg/day or fexofenadine 60-180 mg once or twice daily)
- Avoid known triggers (NSAIDs, physical factors)
Step 2 - If inadequate control after 2-4 weeks
Add one or more of:
- Increase dose of second-generation antihistamine (up to 4x standard dose)
- Add a second-generation antihistamine
- Add an H2 antagonist: Famotidine 20 mg twice daily or Cimetidine 400 mg twice daily
- Add a leukotriene receptor antagonist: Montelukast 10 mg/day
- Add a first-generation antihistamine at bedtime
Step 3 - If still inadequate (after another 2-4 weeks)
- Dose advancement of a more potent antihistamine: Hydroxyzine or Doxepin as tolerated
Step 4 - Refractory / Specialist-managed
- Omalizumab (anti-IgE monoclonal antibody): 150-300 mg subcutaneously once monthly
- Cyclosporine: 3 mg/kg/day or higher for 8-16 weeks (added to background antihistamine)
E. Refractory and Special Cases
For delayed pressure urticaria and urticarial vasculitis (where antihistamines are often ineffective), options include:
- Systemic corticosteroids
- Dapsone
- Antifibrinolytics (tranexamic acid or epsilon-aminocaproic acid) - especially useful with angioedema
- Methotrexate
- Tacrolimus
- Hydroxychloroquine
- IV immunoglobulin (IVIG)
- Plasmapheresis
- Narrow-band UVB phototherapy
Note: Evidence for these agents is limited and mostly anecdotal. Risks vs. symptom burden must be weighed carefully.
F. Hereditary Angioedema (Bradykinin-mediated)
Distinct from histamine-mediated urticaria - antihistamines are not effective:
- Acute attacks: Icatibant, Ecallantide, or purified/recombinant C1-inhibitor
- Prophylaxis: C1-inhibitor, Lanadelumab
Special Populations
Pregnancy / Lactating Women
- Avoid systemic treatment in the first trimester if possible
- Chlorphenamine preferred (long safety record)
- Cetirizine and loratadine acceptable, preferably after first trimester, when benefits outweigh risks
Pediatric Patients
- Same treatment principles as adults
- Doses follow manufacturer's weight-based recommendations
Quick Summary Table
| Severity | First-line | Add-on / Escalation |
|---|---|---|
| Mild/acute | Non-sedating H1 antihistamine | - |
| Moderate/severe | H1 antihistamine + corticosteroids | H2 antagonist, IV diphenhydramine |
| Chronic (CSU) | 2nd-gen antihistamine | Up-dose to 4x, montelukast, omalizumab |
| Refractory CSU | Omalizumab | Cyclosporine |
| Anaphylaxis | Epinephrine + IV steroids | H1 + H2 IV antihistamines |
| HAE | C1-INH / Icatibant | Lanadelumab (prophylaxis) |
Sources:
- Goldman-Cecil Medicine, International Edition
- Fitzpatrick's Dermatology, Volumes 1 & 2
- EAACI/GA²LEN/EDF/WAO Guideline 2018; AAAAI/ACAAI 2014 Guidelines
Recent evidence (PubMed 2024-2026): A systematic review (PMID 38420865) on acute urticaria treatment and a network meta-analysis (PMID 39673624) on omalizumab dosing for chronic urticaria are available - these are broadly consistent with the stepwise approach above.
This is a shared conversation. Sign in to Orris to start your own chat.