surface guided radiotherapy in Breast cancer
Reading File
Finding Sources
Searching PubMed
"surface guided radiation therapy" AND "breast cancer"
Searching the Web
surface guided radiotherapy SGRT breast cancer clinical review 2024 2025
Finding Sources
Searching PubMed
"surface guided radiation" AND breast
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC13101108/
Finding Sources
Reading Article
PMID: 35179229
Reading Article
PMID: 37787279
Reading Article
PMID: 36898583
Finding Sources
Reading Article
PMID: 36523797
Reading Article
PMID: 41211452
Searching the Web
SGRT breast cancer DIBH AlignRT Catalyst systems deep inspiration breath hold positioning accuracy tattoo-free
Finding Sources
Searching PubMed
SGRT "deep inspiration breath hold" breast cardiac dose
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC11321775/
Reading Article
PMID: 39537683
Reading Article
PMID: 38047221
Reading Article
PMID: 37087557
Searching Images
surface guided radiotherapy breast cancer SGRT DIBH deep inspiration breath hold
I now have comprehensive data to write a detailed response. Let me compile everything.
Surface-Guided Radiotherapy (SGRT) in Breast Cancer
What is SGRT?
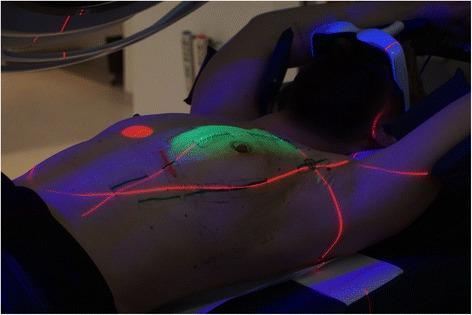
Surface-Guided Radiotherapy (SGRT) uses optical surface imaging — typically stereoscopic cameras and structured light or infrared projection — to map thousands of points on the patient's skin surface in real time. This 3D surface map is continuously compared to a reference surface derived from the planning CT, enabling six-dimensional (6D) monitoring of patient position (translations in x/y/z and rotations in pitch/roll/yaw) without ionizing radiation. In breast cancer, SGRT has become the standard of care for two principal applications: initial patient setup (positioning) and real-time motion monitoring during deep inspiration breath hold (DIBH).
Why SGRT Matters in Breast Cancer
Breast cancer radiotherapy (RT) presents unique challenges:
- The breast and chest wall lie in close proximity to the heart, left anterior descending artery (LAD), and lungs
- Respiratory motion significantly displaces target volumes and organs at risk (OARs)
- Conventional tattoo/laser-based setup has positional isocenter variation up to 4.4 mm in DIBH
- Cardiac dose exposure, especially in left-sided breast cancer, drives long-term radiation-induced cardiotoxicity
SGRT addresses these challenges by providing sub-millimetric positioning accuracy and continuous intrafractional monitoring.
Clinical Applications
1. Deep Inspiration Breath Hold (DIBH)
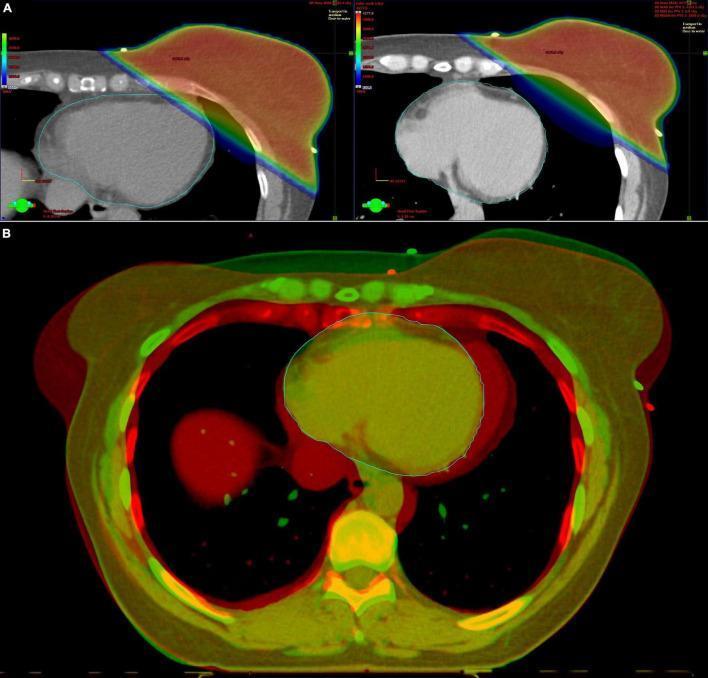
DIBH is the most critical SGRT application in breast RT. During deep inspiration, the lungs expand and physically displace the heart posteriorly and inferiorly away from the anterior chest wall — reducing mean heart dose (MHD) by a median of 43.6% (range 4.2–75.1%) compared to free breathing (Rudat et al., Sci Rep 2024, PMID 39537683).
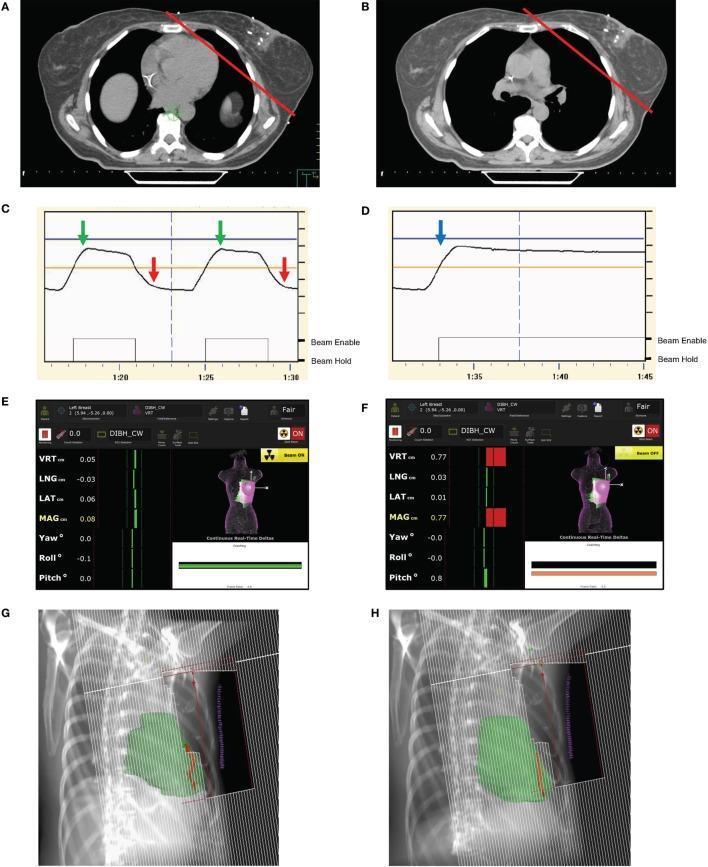
How SGRT guides DIBH:
- Patient takes a deep breath to a pre-defined breath-hold level (BHL)
- SGRT cameras detect the chest surface displacement in real time
- A gating window (typically ±2–3 mm) is set; the linear accelerator beam fires only when the patient is within tolerance ("Beam ON") and holds automatically if they move outside ("Beam Hold")
- Visual biofeedback (goggle displays or ceiling-mounted monitors) guides patients to maintain the target BHL
Key dosimetric benefits of SGRT-DIBH:
- Mean heart dose significantly reduced vs free breathing
- LAD max dose reduced (e.g., 14.6 ± 12.0 Gy → 7.7 ± 7.1 Gy in one RCT)
- Left ventricle V5Gy reduced (2.4% → 0.8%)
- Left lung V20Gy and V30Gy both reduced
- Risk of late cardiac toxicity with SGRT: +1% vs +3.6–20.5% with daily kV-CBCT (due to imaging dose)
2. Patient Setup and Positioning
SGRT provides interactive visual guidance during setup by projecting position correction information directly onto the patient's skin (particularly with Catalyst™ HD system). Studies consistently show:
- SGRT setup is superior to conventional tattoo/laser-based setup in isocenter reproducibility
- In a large comparative study (n=141 patients, 1692 image pairs), AlignRT® achieved the smallest positional variance, followed by Catalyst™, both superior to laser-tattoo setup (Laaksomaa et al., 2022, PMID 36523797)
- Systematic and random errors below 2 mm in all orthogonal directions with SGRT vs CBCT
- Mean setup error between SGRT and CBCT: <0.08 cm (DIBH) and <0.30 cm (free breathing)
- SGRT reduces total treatment time by approximately 20% due to less frequent CBCT requirement
3. Tattoo-Free Radiotherapy
One emerging benefit is elimination of permanent skin tattoos. A 2025 study (Malhotra et al., PMID 41211452) demonstrated:
- SGRT setup was equivalent or faster than tattoo-based setup
- Free-breathing setups: SGRT was 11 seconds faster per fraction
- DIBH setups: equivalent time; SGRT 23 seconds faster for free-breathing
- No significant difference in positional shifts on pre-treatment imaging
- Fiscally feasible and non-inferior to permanent tattoos
This matters because permanent tattoos have a documented negative emotional impact on breast cancer survivors.
SGRT Systems in Clinical Use
| System | Manufacturer | Technology |
|---|---|---|
| AlignRT® | VisionRT (London, UK) | Stereoscopic cameras, structured white light |
| Catalyst™ / Catalyst+ HD | C-RAD (Uppsala, Sweden) | Laser-based scanning, projects guidance light onto patient |
| ExacTrac Dynamic | Brainlab | SGRT + stereoscopic X-ray hybrid |
| Sentinel | C-RAD | Free-breathing surface reference; used with Catalyst |
All three major systems (AlignRT, Catalyst, RPM+lasers) have been compared in large multicenter studies, with SGRT consistently outperforming conventional laser-tattoo positioning.
SGRT in Locoregional Breast Radiotherapy
When regional nodal irradiation (RNI) is added (axilla, supraclavicular fossa, internal mammary nodes), SGRT-DIBH is especially beneficial but technically more complex:
- Arm position significantly affects lymph node dose; the arms are outside the field of view of most SGRT systems, creating a limitation
- Locoregional lymph node positions cannot always be accurately predicted from surface anatomy alone
- SGRT shows 6D monitoring of chest position, posture, and movement throughout treatment
- For right-sided breast + RNI, SGRT-DIBH reduces liver mean dose dramatically (from 916.9 cGy to 281.2 cGy), as well as heart and right coronary artery dose (Lai et al., 2023, PMID 37087557)
Key Technical Considerations and Challenges
Region of Interest (ROI) Selection
The ROI defined on the CT surface for SGRT tracking must be chosen carefully:
- Chest-only ROI is standard but may miss abdominally-driven DIBH patients
- ~15% of left-sided breast cancer patients are "abdominal DIBH" (A-DIBH) with minimal vertical chest elevation (≤5 mm) — these patients require an abdominal ROI or surrogate to ensure adequate heart sparing; conventional chest-only SGRT will incorrectly trigger beam-on while the heart remains in an elevated position (Zeng et al., 2023, PMID 38047221)
Systematic Errors
- Reference surface capture timing matters: tissue swelling after CT simulation can cause systematic errors if surface was captured at simulation
- Acquiring a new reference surface after the first IGRT-corrected fraction reduces systematic posture errors
- Setup images (CBCT/kV) are still recommended, particularly in the first 2 weeks; a combined protocol of daily SGRT + CBCT 3×/week (mandatory in weeks 1–2) optimizes accuracy and efficiency
Breath-Hold Level (BHL) Management
- If the BHL is inconsistently achieved, SGRT detects this and withholds beam
- Clinicians can raise/lower BHL windows or re-acquire DIBH surfaces mid-course
Skin Dressings
- Prophylactic skin dressings (for radiation dermatitis) can disrupt SGRT surface tracking; studies confirm this effect must be accounted for in workflow design (PMID 38525921)
Comparison with Mechanically-Assisted DIBH
- In a 2023 RCT (Vander Veken et al., PMID 36898583), mechanically-assisted non-invasive ventilation DIBH (MANIV-DIBH) achieved equivalent positional breast accuracy to voluntary SGRT-guided DIBH (sDIBH), but provided better OAR sparing (LAD near-max dose 7.7 vs 14.6 Gy; left ventricle V5Gy 0.8% vs 2.4%). This suggests SGRT-guided voluntary DIBH, while excellent, may be surpassed by mechanically-assisted techniques for high-risk cardiac anatomy.
SGRT vs CBCT: Imaging Dose Comparison
A critical advantage of SGRT over daily kV-CBCT is the elimination of imaging-associated radiation exposure:
| Imaging Strategy | Additional Cardiac Toxicity Risk |
|---|---|
| SGRT (optical, no radiation) | +1% |
| Daily kV-CBCT | +3.6% to +20.5% |
This makes SGRT the preferred setup modality from a radiation safety perspective when sufficient positional accuracy is achievable.
Current Guidelines and Standards
The AAPM Task Group Report 302 (Al-Hallaq et al., Med Phys 2022, PMID 35179229) — the definitive technical guideline for SGRT — recommends:
- SGRT for initial patient positioning (all sites)
- SGRT as the standard for breast DIBH treatment guidance
- Commissioning and ongoing QA requirements for all video-based SGRT systems
- Workflow integration with IGRT (CBCT/kV imaging), not replacement of it
Clinical Summary
| Application | Evidence Level | Key Benefit |
|---|---|---|
| DIBH guidance (left breast) | Strong | Cardiac/LAD dose reduction |
| DIBH guidance (right breast + RNI) | Moderate | Liver/heart/RCA dose reduction |
| Patient setup (all breast) | Strong | Sub-mm accuracy, superior to lasers |
| Tattoo-free treatment | Moderate | Non-inferior accuracy, patient quality of life |
| Motion monitoring (intrafractional) | Strong | Real-time gating, beam hold on movement |
| Reduction in CBCT frequency | Moderate | ~20% treatment time reduction, less imaging dose |
SGRT in breast cancer represents one of the most clinically impactful applications of image guidance in modern radiation oncology — combining cardiac protection through DIBH optimization with improved setup accuracy, reduced imaging dose, and enhanced patient experience through tattoo-free workflows.
Key References:
- AAPM TG-302: Al-Hallaq et al., Med Phys 2022 [PMID: 35179229]
- Rudat et al., Sci Rep 2024 (DIBH + SGRT OAR impact) [PMID: 39537683]
- Laaksomaa et al., Rep Pract Oncol Radiother 2022 (AlignRT vs Catalyst vs laser) [PMID: 36523797]
- Vander Veken et al., Radiother Oncol 2023 RCT (voluntary vs mechanical DIBH) [PMID: 36898583]
- Zeng et al., Adv Radiat Oncol 2023 (abdominal DIBH pitfall) [PMID: 38047221]
- Lai et al., J Appl Clin Med Phys 2023 (right-sided breast + RNI) [PMID: 37087557]
- Malhotra et al., Tech Innov Patient Support Radiat Oncol 2025 (tattoo-free) [PMID: 41211452]
- Bellala et al., J Cancer Res Ther 2023 (clinical review, 533 patients) [PMID: 37787279]
This is a shared conversation. Sign in to Orris to start your own chat.