
027bf008-ac4e-4eb5-b2af-0fcd7d6c5c2e.jpeg
I want this answer for the spm exam from standard textbook
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Searching the Web
Park's SPM "rule of halves" hypertension tracking blood pressure
Searching the Web
Park's SPM "cancer registry" PBCR HBCR India types
Searching the Web
Park's SPM RHD rheumatic heart disease epidemiological factors prevention India
Searching the Web
Park SPM obesity epidemiological determinants BMI causes risk factors
Searching the Web
Park SPM "changing concepts" eye health care preventable blindness VISION 2020
Here are complete short-essay answers for all 7 questions from the SPM slip test on NCDs, drawn primarily from Park's Textbook of Preventive and Social Medicine.
Slip Test - NCDs: Short Essay Answers
Q1. Components and Activities of NPCDCS at Various Levels of the Health Care System in India
(Park's Textbook of PSM, Chapter on Non-Communicable Diseases)
Background
India is experiencing rapid health transition with a rising burden of NCDs - particularly cardiovascular disease, diabetes mellitus, cancer, stroke, and chronic lung diseases. NCDs accounted for 60% of deaths in 2016. The National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases and Stroke (NPCDCS) was formed by integrating the earlier NCD programme with the National Cancer Control Programme. During the 11th Five Year Plan, 100 districts in 21 states were covered; during the 12th FYP, the programme expanded to all districts of the country.
Components
A. Diabetes, Cardiovascular Disease and Stroke (DCS) Component
Major Objectives:
- Prevent and control common NCDs through behaviour and lifestyle changes
- Provide early diagnosis and management of common NCDs
- Build capacity at various levels of health care for prevention, diagnosis, and treatment
- Train human resources (doctors, paramedics, nurses) to cope with increasing NCD burden
- Establish capacity for palliative and rehabilitative care
B. Cancer Component
- Common diagnostic services, basic surgery, chemotherapy, and palliative care at 100 district hospitals
- Each district supported with Rs. 1.66 crores per annum
- Chemotherapy drugs for 100 patients per district hospital
- Day care chemotherapy facilities at 100 district hospitals
- Home-based palliative care for chronic cancer patients at 100 districts
- State Cancer Institutes as apex institutions; 45 Tertiary Cancer Centres (TCCs) strengthened
Activities at Various Levels
Sub-Centre Level
- Health promotion for behaviour and lifestyle change through camps, IPC, posters, banners
- Opportunistic screening of population above 30 years using BP measurement and blood glucose (strip method)
- Suspected cases of diabetes and hypertension referred to CHC/higher facility
Community Health Centre (CHC) Level
- NCD Clinic at CHC provides:
- Diagnosis by blood sugar, lipid profile, ultrasound, X-ray, ECG
- Management and stabilization of CVD, diabetes, stroke (OP and IP)
- Home visits by a designated nurse for bedridden cases
- Monthly village clinics on a random basis
- Referral of complicated cases to district hospital
District Hospital Level
- NCD Clinic screens persons >30 years for diabetes, hypertension, CVDs
- Detailed investigations for high-risk individuals referred from CHCs
- Regular management and annual assessment of persons with cancer, diabetes, hypertension
- Management of established CVD cases
- Home-based palliative care for chronic/debilitating/progressive patients
- Health education and counselling to patients and attendants
State and Centre Level
- NCD cells established at state and national levels
- Implementation, monitoring, and coordination of NPCDCS across states
- As of Sept 2015: 36 State NCD Cells, 195 District NCD Cells, 201 District NCD Clinics, 1362 CHC NCD Clinics
Urban Health Check-Up Scheme (for Diabetes and Hypertension)
- Screens urban slum population for diabetes and hypertension
- Targets all persons ≥30 years and all pregnant women
New Initiatives under NPCDCS
- Intervention for prevention and control of Rheumatic Heart Disease (integrated with RBSK)
- Integration of AYUSH with NPCDCS
- Integration of RNTCP with NPCDCS for TB-Diabetes comorbidity management
Q2. Cancer Registry
(Park's Textbook of PSM; National Cancer Registry Programme)
Definition
A cancer registry is an organization responsible for the continued, systematic collection, storage, analysis, interpretation, and reporting of data on persons with cancer, over a defined time, place, and population.
Purpose / Uses
- Measure cancer incidence, trends, and mortality
- Estimate burden and patterns of cancer
- Monitor and assess effectiveness of cancer control activities
- Support planning, evaluation, and development of cancer control programmes
- Facilitate epidemiological research and international comparisons
Types of Cancer Registries
1. Population-Based Cancer Registry (PBCR)
- Collects data on all new cancer cases in a well-defined geographical area (population resident ≥1 year)
- Can measure cancer incidence, prevalence, trends, and mortality
- Unique role in planning and evaluating cancer control at the community level
- Active case finding from multiple sources: hospitals, labs, death certificates
2. Hospital-Based Cancer Registry (HBCR)
- Records information on cancer patients seen in a particular hospital
- Population from which cases arise is NOT defined (depends on referrals)
- Used primarily for:
- Administrative purposes (forecasting equipment, HR needs)
- Reviewing clinical performance
- Research into causes, prevention, and control
3. Pathology-Based Cancer Registry
- Records from one or more laboratories on histologically diagnosed cancers
- Diagnosis is of high quality but population not defined
- Supports laboratory-based services
Cancer Registry in India - NCRP
- The National Cancer Registry Programme (NCRP) started in 1982 with 3 PBCRs and 3 HBCRs, coordinated by ICMR
- Coordinating unit: National Centre for Disease Informatics and Research (NCDIR), Bengaluru (since 1991)
- The Bombay Cancer Registry (1963) was the first PBCR in India (Indian Cancer Society, Mumbai)
- As of recent data: 31 PBCRs and 29 HBCRs functioning in India
- Under NPCDCS, the cancer component uses registry data to guide chemotherapy, surgical, and palliative services
Quality Indicators for PBCR
- Microscopic Verification (MV%) >75%
- Death Certificate Only (DCO%) <20%
- Other and Unspecified sites (O&U%) <15%
- Mortality-to-Incidence ratio (M:I%) monitored
Q3. Rule of Halves in Hypertension + Note on Tracking of BP
(Park's Textbook of PSM)
Rule of Halves in Hypertension
The "Rule of Halves" is an important concept in the epidemiology and control of hypertension. It describes the cascade of deficiencies at each step from hypertension detection to control:
| Step | Proportion |
|---|---|
| Of all hypertensives in the community | 100% |
| Only half are aware of their condition (diagnosed) | ~50% |
| Of those aware, only half are on treatment | ~25% |
| Of those on treatment, only half are adequately controlled | ~12.5% |
Significance:
- Demonstrates the enormous "iceberg" of undetected and uncontrolled hypertension in the community
- Despite advances in treatment, a large proportion of hypertensives remain undetected, untreated, or inadequately controlled
- Highlights the need for mass screening, early detection, and long-term follow-up
- Emphasizes that treatment alone is insufficient without adherence, regular follow-up, and lifestyle modification
Note on Tracking of Blood Pressure
Definition: Tracking of blood pressure refers to the tendency of an individual's blood pressure to remain in the same relative rank within the population over time (i.e., a person with BP in the upper quartile in childhood is likely to remain there in adulthood).
Significance:
- Children with persistently elevated BP are at high risk of developing adult hypertension
- Tracking begins even in infancy and continues through life
- Supports the case for screening children and adolescents for blood pressure
- Early lifestyle interventions (diet, physical activity, weight control) in those with high-normal BP can prevent overt hypertension
Under NPCDCS: Opportunistic screening for BP is done for all persons >30 years at sub-centres and PHCs using standard sphygmomanometry. Referral cutoffs: systolic >140 mmHg or diastolic >90 mmHg.
Q4. Epidemiological Factors in RHD and Its Prevention
(Park's Textbook of PSM; WHO)
Definition
Rheumatic Heart Disease (RHD) is permanent damage to the heart valves (mitral, aortic) caused by repeated episodes of Acute Rheumatic Fever (ARF), which is itself an autoimmune response to Group A Beta-haemolytic Streptococcal (GABHS) pharyngitis.
Epidemiological Factors
Agent:
- Group A Beta-haemolytic Streptococcus (Streptococcus pyogenes)
- Spreads via droplets from throat of infected persons
- Certain streptococcal serotypes are more rheumatogenic than others
Host Factors:
- Age: Most common in children 5-15 years; ARF peaks at 5-15 years; RHD manifests in adolescence/early adulthood
- Sex: Females are more susceptible to RHD (especially mitral stenosis); RF affects both sexes equally in childhood
- Genetics: Familial predisposition; certain HLA types associated
- Immunity: Repeated episodes of ARF worsen valve damage; previous streptococcal infection → sensitized immune response
- Nutritional status: Low BMI, protein-energy malnutrition impair immune response to GAS, predisposing to ARF and RHD
- Social class: RHD is a disease of poverty
Environmental Factors:
- Overcrowding: Facilitates spread of streptococcal infection
- Poor housing and ventilation
- Low socioeconomic status: Limited access to healthcare, antibiotics
- Undernutrition
- Climate: Cold, damp climates favour upper respiratory infections
- Seasonality: ARF is more common in winter/spring (when GABHS pharyngitis peaks)
Prevention
Primordial Prevention:
- Improvement of socioeconomic conditions, housing, nutrition
- Reduction of overcrowding
Primary Prevention:
- Prompt identification and treatment of GABHS pharyngitis with benzathine penicillin G (single IM injection of 1.2 million units) or oral penicillin V for 10 days
- Health education about sore throat and when to seek care
Secondary Prevention (most important):
- Prevents recurrent ARF in established cases
- Benzathine penicillin G 1.2 million units IM every 3-4 weeks for a minimum of 5-10 years or until age 25 (whichever is longer), and lifelong if significant RHD present
- Secondary prophylaxis is the most cost-effective intervention
- National programme: NPCDCS and RBSK include interventions for RHD prevention
Tertiary Prevention:
- Surgical correction (valvotomy, valve replacement) for established valvular disease
- Management of complications: heart failure, atrial fibrillation, stroke
Q5. Epidemiological Determinants in Obesity
(Park's Textbook of PSM)
Definition
Obesity is defined as abnormal or excessive accumulation of fat that presents a risk to health. By WHO criteria:
- Overweight: BMI ≥ 25 kg/m²
- Obesity: BMI ≥ 30 kg/m²
- For Asians/Indians: Overweight ≥ 23, Obesity ≥ 25 kg/m²
Waist-Hip Ratio (WHR): Abdominal (central) obesity when WHR >1.0 (male), >0.85 (female).
Epidemiological Determinants (Using Epidemiological Triad)
A. Agent Factors (Nutrition)
- Energy imbalance: Excessive caloric intake relative to energy expenditure is the proximate cause
- High fat, high sugar diet: ice creams, fast foods, refined carbohydrates
- Low dietary fibre intake
- High-calorie dense foods
- Protective foods: salads, whole grains, cereals, vegetables
B. Host Factors
- Age: Obesity increases with age (declining BMR, reduced physical activity); childhood obesity predicts adult obesity
- Sex: Women have higher body fat % than men at same BMI; post-menopausal women are especially prone
- Genetics: Strong hereditary predisposition; children of obese parents have 70-80% risk; polygenic inheritance
- Endocrine disorders: Hypothyroidism, Cushing's syndrome, PCOS, hypothalamic disorders
- Psychological factors: Emotional eating, depression, binge eating disorder
- Drugs: Corticosteroids, antipsychotics, insulin, oral contraceptives
- Sleep: Short sleep duration increases obesity risk (↑ ghrelin, ↓ leptin)
C. Environmental Factors
- Physical inactivity / sedentary lifestyle: TV watching, screen time, motorized transport, desk jobs
- Urbanization: "Obesogenic environment" - easy availability of calorie-dense foods, reduced physical activity
- Socioeconomic status: Paradoxically, both poverty (poor diet quality) and affluence (sedentary jobs) increase risk; in developing countries, higher SES women are more obese
- Food environment: Marketing of unhealthy foods, fast food availability
- Occupation: Sedentary occupations vs. manual labour
Consequences of Obesity
- Type 2 diabetes mellitus
- Hypertension, coronary heart disease, stroke
- Dyslipidaemia
- Obstructive sleep apnoea
- Osteoarthritis
- Cancers: endometrium, breast, colon, prostate, kidney, gall bladder
- Psychological effects: depression, low self-esteem
Q6. Changing Concepts in Eye Health Care and a Note on Preventable Blindness
(Park's Textbook of PSM; VISION 2020)
Changing Concepts in Eye Health Care
Old (Traditional) Concept:
- Eye care was curative and hospital-based
- Focus on treatment of established disease
- Specialist-dependent (ophthalmologist-centred)
- No community-based approach
- Blindness considered largely inevitable
New (Modern) Concept:
- Community-based, integrated eye care within primary health care system
- Emphasis on prevention and early detection
- Comprehensive eye care: promotive, preventive, curative, rehabilitative
- Task-shifting to ophthalmic assistants, primary health workers for screening
- VISION 2020: The Right to Sight - WHO/IAPB global initiative launched in 1999 to eliminate avoidable blindness by 2020
- Eye care as a human right and development issue
- Integration with national health systems (NHM in India)
- Focus on cost-effective interventions: cataract surgery, refractive error correction, vitamin A supplementation, trachoma control
Principles of VISION 2020 (ISEE acronym):
- I - Integrated approach
- S - Sustainable services
- E - Equity
- E - Evidence-based interventions
National Programme for Control of Blindness (NPCB), India:
- Launched in 1976; now National Programme for Control of Blindness and Visual Impairment (NPCB&VI)
- Goal: Reduce prevalence of blindness from 1.1% to 0.3%
- Activities: Free cataract surgery (IOL implantation), school eye screening, vitamin A distribution, training of ophthalmic personnel
Note on Preventable Blindness
Definition: Blindness that can be prevented, treated, or reversed with available cost-effective interventions.
Globally: ~80% of all blindness is avoidable (preventable or treatable).
Causes of blindness (global and India):
| Cause | Nature |
|---|---|
| Cataract (~66% in India) | Treatable (surgery) |
| Refractive errors | Correctable (spectacles) |
| Glaucoma | Preventable if detected early |
| Trachoma | Preventable (SAFE strategy: Surgery, Antibiotics, Face washing, Environmental improvement) |
| Vitamin A deficiency / Corneal blindness | Preventable (Vit A supplementation, measles vaccination) |
| Diabetic retinopathy | Preventable with diabetes control |
| Retinopathy of prematurity | Preventable with proper neonatal care |
Non-preventable (unavoidable) causes:
- Macular degeneration (age-related)
- Retinitis pigmentosa (hereditary)
- Optic atrophy
Key interventions in India:
- Free IOL cataract surgery under NPCB
- Vitamin A prophylaxis (200,000 IU every 6 months to children 1-5 years)
- Trachoma control (SAFE strategy)
- School eye screening (spectacles for refractive errors)
- Screening for diabetic retinopathy and glaucoma
Q7. Human and Environmental Factors in Road Traffic Accidents
(Park's Textbook of PSM, Chapter on Accidents)
Introduction
Road Traffic Accidents (RTAs) are a leading public health problem. Globally, ~1.25 million people die annually from road accidents. In India, 218,876 deaths occurred due to road injuries in 2017 (age-standardized death rate: 17.2/100,000). Road injury was the leading cause of death in males aged 15-39 years in India in 2017.
RTAs are a complex phenomenon of multiple causation. The aetiological factors are classified into human and environmental factors. Up to 90% of factors responsible for accidents are attributed to human failure.
PRIMARY FACTORS IN ACCIDENTS (Epidemiological Classification)
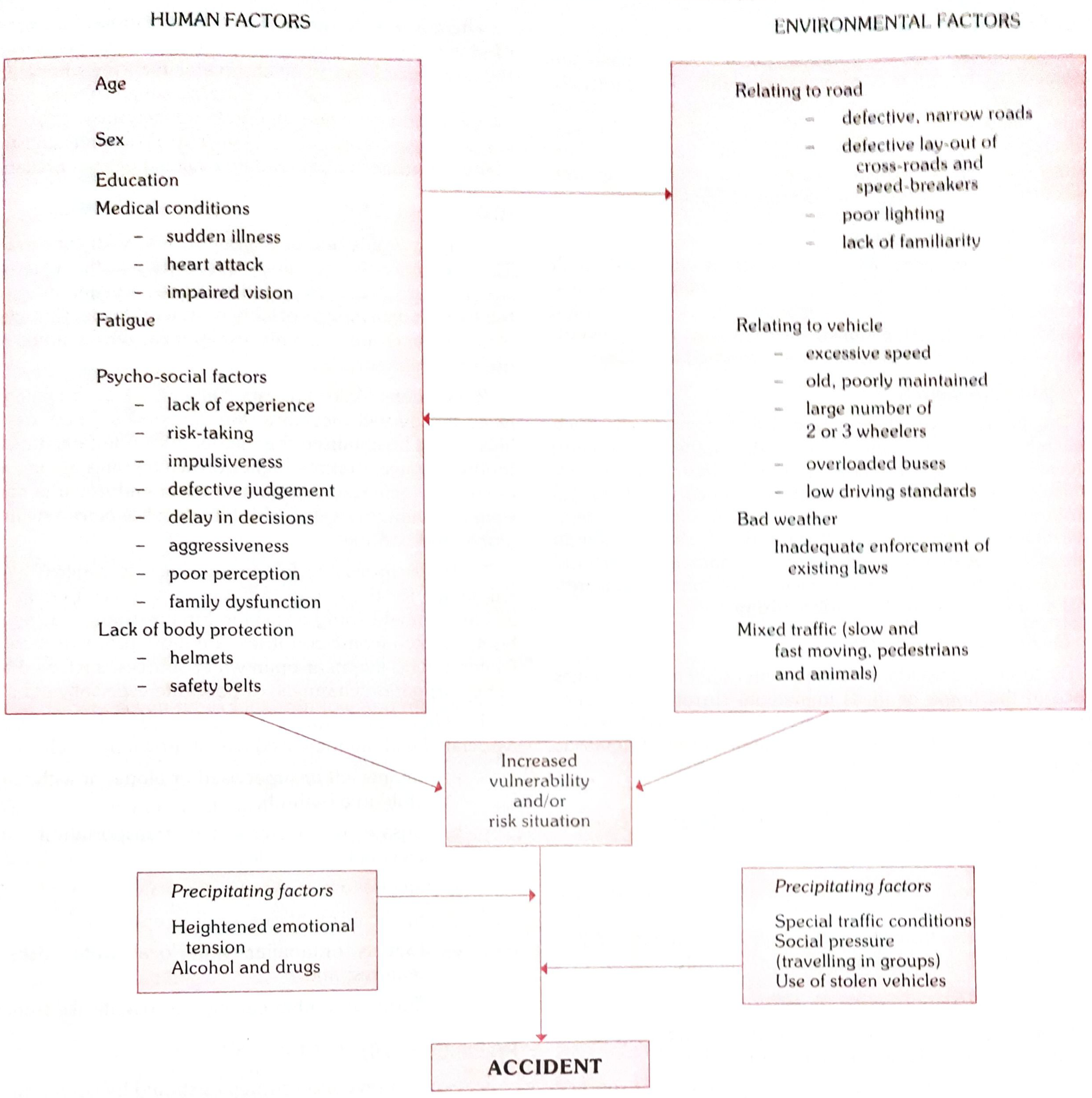
Fig. 1 - Primary factors in accidents (Park's PSM)
A. HUMAN FACTORS
Human factors include characteristics of the driver, pedestrian, or other road user that contribute to crashes.
1. Age:
- Children and young people under 25 years account for >30% of those killed and injured
- Young male drivers (<25 years) are almost 3 times more likely to be killed than young females
- Road injury is the leading cause of death in males 15-39 years in India
2. Sex:
- Males are more likely to be involved in crashes at all ages
- In India, age-standardized death rate: males 25.7/100,000 vs. females 8.5/100,000
3. Alcohol and Drugs:
- Alcohol is the direct cause of 30-50% of severe road accidents
- Risk of crash increases significantly above a BAC of 0.04 g/dl
- Barbiturates, amphetamines, cannabis also impair driving
- Sobriety checkpoints can reduce alcohol-related crashes by ~20%
4. Speed:
- Excessive speed directly increases likelihood of crash and severity of injury
- Pedestrians have 90% survival chance at ≤30 km/h vs. <50% at ≥45 km/h
- Speed zones of 30 km/h are recommended in areas with vulnerable road users
5. Non-use of safety devices:
- Not wearing helmets: wearing a motorcycle helmet correctly can reduce risk of death by 40% and severe injury by 70%
- Not wearing seat belts: seat belts reduce fatality risk by 40-50% (front seat) and 25-75% (rear seat)
- Lack of child restraints
6. Distracted Driving:
- Use of mobile phones, texting while driving
- Driver fatigue and drowsiness
- Emotional disturbance
7. Driver's physical/psychological condition:
- Visual defects, hearing impairment
- Fatigue, stress, emotional disturbance
- Medical conditions (epilepsy, diabetes)
- Poor vehicle maintenance habits
8. Pedestrian behaviour:
- Jaywalking, crossing at inappropriate places
- Lack of awareness of traffic rules
- Children playing on roads
B. ENVIRONMENTAL FACTORS
1. Road Factors:
- Poor road design: sharp curves, narrow roads, absence of median dividers
- Bad road conditions: potholes, poor lighting, absence of signage
- Absence of footpaths/sidewalks for pedestrians
- Absence of speed breakers near schools/residential areas
2. Vehicle Factors:
- Defective brakes, steering, or tyres
- Poor vehicle design (no crumple zones in older vehicles)
- Absence of airbags
- Overloading of vehicles
3. Weather and Climatic Conditions:
- Rain reduces visibility and traction
- Fog: poor visibility
- Glare (sunlight/headlights)
4. Traffic Conditions:
- Mixed traffic (pedestrians + vehicles of varying speeds on same road)
- Lack of traffic signals or non-functional signals
- Poorly designed intersections
5. Socioeconomic Environment:
-
90% of road traffic deaths occur in low and middle-income countries
- People from lower socioeconomic backgrounds are at higher risk
Prevention of RTAs (Brief)
- Data collection - Reporting system of all accidents
- Safety education - "If accident is a disease, education is its vaccine"
- Safety measures - Helmet, seat belt, child restraints, door locks
- Alcohol control - Breath testing, BAC laws, enforcement
- Primary care - Emergency medical services at accident site, transport, hospital
- Elimination of causative factors - Road improvement, speed limits, marking danger points
- Enforcement of laws - Driving tests, medical fitness, periodic re-examination of drivers >55 years
- Rehabilitation - Disability care after accidents
All answers based on: Park's Textbook of Preventive and Social Medicine (Park J.E., Bhanot Publications). Additional reference for Cancer Registry: National Cancer Registry Programme (ICMR-NCDIR).
This is a shared conversation. Sign in to Orris to start your own chat.