Everything related to hernia wrt surgery posting
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from authoritative textbooks to compile a thorough surgery posting answer on hernias. Let me write the complete response.
Hernia - Complete Surgery Posting Notes
Sources: Schwartz's Principles of Surgery 11e, Maingot's Abdominal Operations, Bailey & Love's Short Practice of Surgery 28e, Current Surgical Therapy 14e, Fischer's Mastery of Surgery 8e
Definition
A hernia is an area of weakness or complete disruption of the fibromuscular tissues of the body wall through which structures from the contained cavity herniate. The hernia refers to the actual anatomic defect; hernia contents are the structures that pass through it. - Maingot's Abdominal Operations
Epidemiology
- Inguinal hernia repair is the most common general surgery procedure performed worldwide
- ~700,000 inguinal hernia repairs/year in the US; an additional 450,000 in ambulatory surgery centers
- ~75% of abdominal wall hernias occur in the groin
- 90% of inguinal hernia repairs are in men, 10% in women
- Lifetime risk: men 27%, women 3%
- Bimodal age distribution: peak before 1 year and after 40 years
- Inguinal > Femoral (5:1)
- ~70% of femoral hernia repairs are in women, but the most common groin hernia in both sexes is still indirect inguinal
- Incisional hernias develop in up to 28% of patients after laparotomy - Current Surgical Therapy 14e
Anatomy of the Inguinal Canal

Digital examination of the inguinal canal (Schwartz's Principles of Surgery)
The inguinal canal is an approximately 4-6 cm long cone-shaped region in the anterior pelvis. - Schwartz's Principles of Surgery 11e
| Boundary | Structure |
|---|---|
| Anterior | External oblique aponeurosis |
| Posterior | Transversalis fascia + transversus abdominis |
| Superior | Internal oblique + transversus abdominis |
| Inferior | Inguinal (Poupart's) ligament |
| Deep ring | Hiatus in transversalis fascia |
| Superficial ring | Defect in external oblique aponeurosis |
Key Structures
- Iliopubic tract: aponeurotic band from ASIS to Cooper's ligament; forms inferior margin of internal ring
- Cooper's ligament (pectineal ligament): on the superior surface of the pubic ramus; critical for McVay repair
- Lacunar ligament (Gimbernat's): triangular fanning of the inguinal ligament at the pubic tubercle; forms the medial boundary of the femoral canal
- Conjoined tendon: fusion of internal oblique and transversus abdominis aponeuroses; inserts on pubic tubercle
- Hesselbach's triangle: bounded by inferior epigastric vessels laterally, inguinal ligament inferiorly, rectus sheath medially - site of direct hernias
Spermatic cord contents (3-3-2 rule)
- 3 arteries: testicular, cremasteric, artery of vas deferens
- 3 veins: pampiniform plexus, cremasteric vein, vein of vas
- 2 nerves: ilioinguinal nerve, genital branch of genitofemoral nerve
- Vas deferens
Classification
By Etiology
- Congenital (indirect inguinal) - patent processus vaginalis
- Acquired (direct inguinal, incisional, femoral)
By Clinical State
| Type | Description |
|---|---|
| Reducible | Contents return spontaneously or with gentle pressure |
| Irreducible (Incarcerated) | Contents cannot be reduced; no vascular compromise |
| Obstructed | Bowel in sac with intestinal obstruction, no strangulation |
| Strangulated | Vascular compromise of contents; surgical emergency |
| Richter's hernia | Only the antimesenteric wall of bowel is strangulated - can strangulate without obstruction |
| Maydl's hernia (hernia-en-W) | Two loops in sac, middle loop strangulates inside abdomen |
| Littre's hernia | Meckel's diverticulum in the sac |
| Sliding hernia | Posterior wall of sac formed by a viscus (cecum on right, sigmoid on left) |
| Pantaloon hernia | Combined direct + indirect hernia straddling inferior epigastric vessels |
Nyhus Classification (most widely used grading for inguinal hernias)
| Type | Description |
|---|---|
| I | Indirect, normal internal ring |
| IIA | Direct, small |
| IIB | Direct, large |
| IIIA | Direct |
| IIIB | Indirect, enlarged ring ± sliding or scrotal |
| IIIC | Femoral |
| IV | Recurrent |
Types of Groin Hernia
Indirect Inguinal Hernia
- Passes through the deep (internal) inguinal ring, traverses the canal, exits the superficial ring
- Lateral to the inferior epigastric vessels
- Congenital: due to patent processus vaginalis
- Most common type in both sexes and all ages
- Sac can reach the scrotum (scrotal hernia)
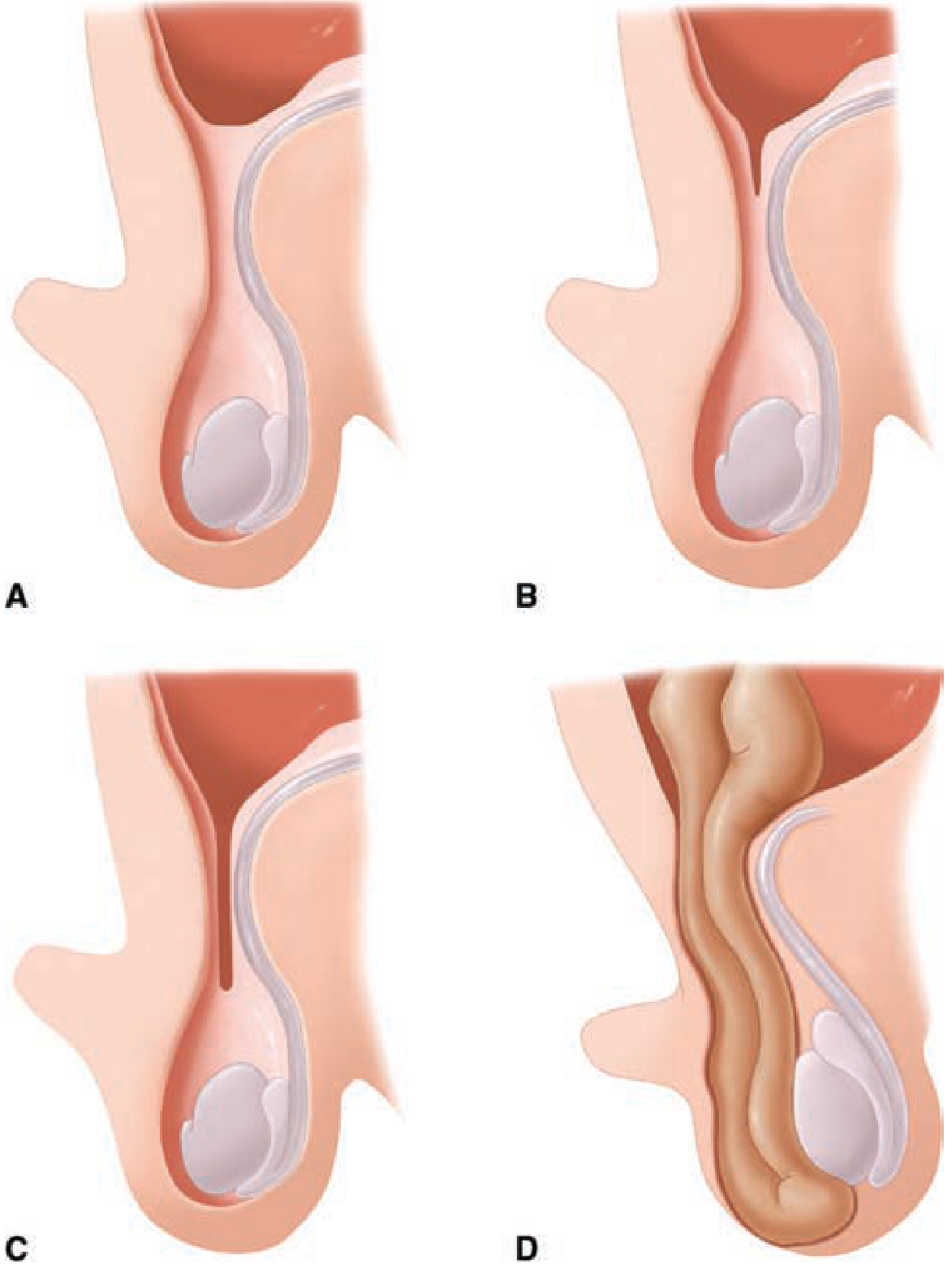
Varying degrees of closure of the processus vaginalis: A. Closed. B. Minimally patent. C. Moderately patent. D. Scrotal hernia. (Schwartz's Principles of Surgery)
Direct Inguinal Hernia
- Protrudes directly through the posterior wall of Hesselbach's triangle
- Medial to the inferior epigastric vessels
- Acquired; due to weakness in transversalis fascia
- Less likely to strangulate (wide neck)
- Common in older men
Differentiating Direct vs Indirect - Key Points
| Feature | Indirect | Direct |
|---|---|---|
| Relation to inf. epigastric | Lateral | Medial |
| Mechanism | Through deep ring | Through Hesselbach's triangle |
| Age | Any (often young) | Older |
| Strangulation risk | Higher | Lower |
| Cough impulse on digital exam | Tip of finger | Dorsum of finger |
| Control on deep ring pressure | Controlled | Not controlled |
Note: Clinical accuracy of differentiating direct from indirect hernia is only slightly better than chance (50%); confirmation is operative. - Schwartz's Principles of Surgery 11e
Femoral Hernia
- Passes through the femoral canal (medial to femoral vein, lateral to lacunar ligament), below the inguinal ligament
- F:M ratio ~3:1 overall; but indirect inguinal is still most common groin hernia in women
- High risk of strangulation due to tight unyielding femoral ring
- Presents as a lump below and lateral to the pubic tubercle (distinguished from inguinal hernia which is above and medial)
- Often presents as an emergency with strangulation
Risk Factors for Hernia
Conditions that raise intra-abdominal pressure
- Chronic cough (COPD)
- Constipation / straining
- Prostatic hypertrophy
- Ascites
- Obesity
- Pregnancy
Connective tissue disorders (Schwartz's)
Marfan syndrome, Ehlers-Danlos, osteogenesis imperfecta, alpha-1 antitrypsin deficiency, polycystic kidney disease, androgen insensitivity syndrome
Other
- Previous surgery (incisional hernia)
- Smoking (collagen defect)
- Family history (hereditary in 3-fold if first-degree relative affected)
- Male sex
Diagnosis
Clinical
- Groin mass that protrudes on standing, coughing, or straining
- May have dragging/aching pain, especially at end of day
- Reducible on lying down
Physical Examination
- Patient examined standing and lying
- Cough impulse test; digital invagination of scrotal skin along the inguinal canal
- Tip of finger impulse = indirect; Dorsum of finger impulse = direct
- For femoral: palpate below the inguinal ligament, lateral to pubic tubercle
- Assess reducibility; if not reducible, assess for strangulation (tenderness, erythema, systemic signs)
Differential Diagnosis of Groin Swelling
Lymph node, lipoma of cord, undescended testis, saphenous varix, femoral artery aneurysm, psoas abscess, hydrocele, sebaceous cyst, hematoma
Imaging
- Not required for obvious hernias
- Ultrasound: sensitivity 86%, specificity 77% for inguinal hernia; first-line imaging
- CT scan: delineates anatomy, detects occult hernias, excludes other pathology
- MRI: best soft tissue differentiation; used for occult/sports hernia
Management
Conservative
- Watchful waiting is acceptable for asymptomatic or minimally symptomatic reducible inguinal hernias in men
- Risk of strangulation: ~0.5-1% per year; decreases from ~5%/year to 1-2%/year after 6 months as defect enlarges
- Watchful waiting is not safe for femoral hernias (high strangulation risk - all should be repaired)
- Trusses: temporary measure only; no evidence of benefit; may worsen matters by preventing natural reduction
Indications for Surgery
- Symptomatic hernia
- Irreducible hernia
- All femoral hernias
- Any complication (obstruction, strangulation)
- Pediatric hernias (repair promptly to avoid incarceration)
- Patient preference
Anesthesia Options (Maingot's)
| Type | Notes |
|---|---|
| Local (preferred for open) | Ilioinguinal + iliohypogastric nerve block or direct infiltration; least postoperative pain/nausea, shortest recovery; superior in RCT vs regional or GA |
| Regional (spinal/epidural) | Larger operative field; risks: urinary retention, hypotension, prolonged effect |
| General | Required for laparoscopic; complete muscle relaxation needed for insufflation |
Surgical Repair Techniques
Principle: Tension-free repair - the gold standard
Simple suture repair (without mesh) has recurrence rates up to 15%. Mesh repair dramatically reduces recurrence rates.
A. OPEN ANTERIOR REPAIRS
1. Lichtenstein Tension-Free Mesh Repair (Gold Standard for Open)
- Described by Lichtenstein in the 1980s
- A flat synthetic mesh (typically polypropylene) is placed as an onlay on the posterior wall of the inguinal canal
- Keyhole in the mesh accommodates the spermatic cord
- Mesh is sutured to the inguinal ligament inferiorly and conjoined tendon superiorly
- Recurrence rate <1% in experienced hands
- Short learning curve; reproducible regardless of hernia size
- Used for direct, indirect, and combined hernias
2. Tissue-Based (Non-Mesh) Repairs
| Repair | Technique | Notes |
|---|---|---|
| Bassini (1884) | Sutures transversalis fascia + internal oblique + transversus abdominis ("triple layer") to inguinal ligament | Revolutionized hernia repair; recurrence ~5-10% |
| Shouldice | Four-layer imbrication of transversalis fascia with running monofilament | Best tissue repair; recurrence ~2-4% at specialist centers; technique-dependent |
| McVay (Cooper's ligament) | Sutures transversalis fascia/conjoined tendon to Cooper's (pectineal) ligament; requires a relaxing incision | Only repair that addresses both inguinal AND femoral defects; used for femoral hernia, large direct hernia |
| Desarda | Uses a strip of external oblique aponeurosis | Newer modification; being evaluated |
The Cooper's ligament repair (McVay) is the only technique that definitively repairs both the inguinal and femoral hernia defects. - Maingot's Abdominal Operations
3. Plug and Patch (Rutkow-Robbins)
- A mesh plug fills the hernia defect + flat mesh reinforces the floor
- Concern about plug migration and chronic pain; less used now
B. LAPAROSCOPIC REPAIRS
The key anatomical difference: laparoscopic approaches repair the hernia posterior to the defect (preperitoneal plane), whereas open approaches repair it anteriorly. - Maingot's Abdominal Operations
Three techniques exist:
1. TAPP - Transabdominal Preperitoneal
- Standard laparoscopy enters the peritoneal cavity
- Peritoneum over the groin is incised and dissected off
- Mesh placed in the preperitoneal space; peritoneum closed over it
- Good visualization; allows concurrent contralateral assessment
- Risk of intraperitoneal injury
2. TEP - Totally Extraperitoneal
- Balloon dissection creates preperitoneal space without entering peritoneum
- Mesh placed directly in preperitoneal space
- Avoids peritoneal entry; less risk of bowel/vessel injury
- Longer learning curve; difficult with previous lower abdominal surgery
- Preferred by many for unilateral primary hernia
3. IPOM - Intraperitoneal Onlay Mesh
- Mesh placed intraperitoneally
- Requires composite/dual-layer mesh to avoid adhesion to bowel
- Less commonly used for inguinal hernia; more for ventral hernias
Laparoscopic vs Open (Key Points)
- Laparoscopic: less postoperative pain, faster return to activity, lower chronic pain rates
- Laparoscopic: longer learning curve (especially TEP), requires GA
- Laparoscopic: preferred for bilateral hernias (both sides repaired through same incisions) and recurrent hernias after open anterior repair
- Open Lichtenstein: preferred for recurrent hernias after laparoscopic repair, heavily scarred preperitoneal space, patients unfit for GA
- Recurrence rates equivalent between laparoscopic and open with mesh
Robotic Repair
- Robotic inguinal hernia repair has grown rapidly: from 0.7% to 28.8% of inguinal repairs (2012-2018, Michigan Surgical Quality Collaborative)
- Provides better ergonomics and 3D visualization
- Similar outcomes to standard laparoscopic; higher cost - Sabiston Textbook of Surgery
C. MESH MATERIALS
Synthetic Mesh
- Polypropylene (most common) and polyester
- Permanent, hydrophobic; induce local inflammatory response leading to fibrosis and incorporation
- Heavyweight: stronger but more scarring, higher chronic pain risk
- Lightweight (titanium-coated PP, PP-poliglecaprone): more elasticity, less surface area contact
- Meta-analysis of 2310 patients: lower chronic pain (RR 0.61) with lightweight; no difference in recurrence
- Lightweight mesh recommended for TEP/TAPP repairs
Biologic Mesh
- Derived from human/animal connective tissue (acellular dermis, porcine SIS, etc.)
- Reserved for contaminated fields or patients with high infection risk
- High cost + high recurrence rates; no single biologic is standard
- Cross-linked grafts more durable than non-cross-linked
Important note from resource-limited settings
- Sterilized polypropylene mosquito nets have similar mechanical properties to commercial mesh
- Meta-analysis of 577 hernioplasties: similar short-term complication (6.1%) and recurrence (0.17%) rates
Special Hernia Types
Umbilical Hernia
- Common in neonates (90% close spontaneously by 3-4 years)
- In adults: acquired, associated with obesity, ascites, multiparity
- Repair indicated if persistent after age 4 in children; symptomatic or enlarging in adults
- Cirrhotic patients: high risk (up to 20% incidence with ascites); 15% mortality with urgent repair; optimized elective repair preferred
Incisional (Ventral) Hernia
- Occurs in up to 28% after laparotomy
- Risk factors: obesity (BMI >40 = 50% recurrence), smoking, diabetes (HbA1c >8), COPD, wound infection
- Watchful waiting acceptable for asymptomatic small hernias; ~10-15% will eventually require repair
- Repair: open (sublay/retrorectus mesh) vs laparoscopic IPOM
- Surgeon volume matters: >40 cases/year associated with 30-40% lower reoperation rate
Epigastric Hernia
- Through the linea alba above the umbilicus
- Often contains preperitoneal fat; symptomatic despite small size
- Simple repair with mesh for larger defects
Spigelian Hernia
- Through the spigelian fascia (lateral border of rectus abdominis, at the arcuate line)
- Interparietal hernia - lies between muscle layers; can be missed on exam
- Ultrasound/CT often required for diagnosis; laparoscopic repair preferred
Obturator Hernia
- Through obturator foramen; rare; most common in thin elderly women
- Presents with bowel obstruction + Howship-Romberg sign (inner thigh pain on hip extension/internal rotation due to obturator nerve compression)
- Usually diagnosed at emergency laparotomy for bowel obstruction
Hiatal Hernia
- Type I (Sliding): GE junction slides into the chest; 95% of all hiatal hernias; associated with GERD
- Type II (Paraesophageal/Rolling): GE junction below diaphragm, fundus herniates alongside
- Type III (Mixed): elements of both
- Type IV: other viscera (colon, spleen) in the sac
Internal Hernia
- Through a mesenteric or peritoneal defect; congenital or post-surgical (Roux-en-Y gastric bypass most common cause now)
- Presents with intermittent bowel obstruction; CT diagnosis; laparoscopic repair if caught early
Complications of Hernia
Acute Complications
| Complication | Features | Management |
|---|---|---|
| Incarceration | Irreducible, no vascular compromise; may have obstruction | Emergency surgery if cannot reduce; attempt gentle reduction (taxis) |
| Strangulation | Vascular compromise; tender, erythematous, systemic sepsis | Emergency surgery - no attempt at reduction; resection if bowel non-viable |
| Obstruction | Bowel obstruction without strangulation | Urgent surgery |
Signs of strangulation: local tenderness, erythema, edema of overlying skin, pyrexia, tachycardia, leukocytosis, metabolic acidosis
The larger the palpable defect, the lower the risk of incarceration. Risk is highest in the first few months (5%/year), drops to 1-2%/year after 6 months as the defect enlarges. - Maingot's Abdominal Operations
Post-operative Complications
| Complication | Notes |
|---|---|
| Urinary retention | Common especially after spinal anesthesia or in elderly men with BPH |
| Wound infection | 1-2% with mesh; higher with contaminated cases |
| Hematoma/seroma | Seroma common after laparoscopic TEP; usually resolves |
| Chronic groin pain (CPIIP) | Most important long-term complication; ~10-12%; due to mesh, nerve entrapment |
| Recurrence | <1% with Lichtenstein; 0.5-2% with laparoscopic; increases with infection, poor technique |
| Mesh infection | Rare (1%); may require mesh removal |
| Vas deferens/testicular injury | Risk of ischemic orchitis 0.5-1%; testicular atrophy rare |
| Nerve injury | Ilioinguinal, iliohypogastric, genitofemoral nerves at risk; numbness/neuralgia |
Pediatric Hernias
- Almost all are indirect (due to patent processus vaginalis)
- ~90% of boys with undescended testis have a patent processus vaginalis
- Hernias in children should be repaired promptly - incarceration risk is high in infants
- Herniotomy (high ligation of sac at internal ring) is sufficient - no floor repair needed in children
- Laparoscopic approach allows inspection of the contralateral side; contralateral repair if patent
Key Surgical Principles (Summary)
- Tension-free repair is the standard - mesh reduces recurrence
- Laparoscopic preferred for bilateral inguinal hernias and recurrent (after open) hernias
- Open Lichtenstein preferred for recurrent (after laparoscopic) hernias and patients unfit for GA
- All femoral hernias should be repaired regardless of symptoms
- Lightweight mesh preferred for laparoscopic repairs - less chronic pain
- Local anesthesia superior in RCT for open inguinal hernia repair
- Watchful waiting is safe for asymptomatic male inguinal hernias; not safe for femoral hernias
- Strangulation = emergency surgery; do not attempt reduction if signs of vascular compromise
- Preoperative optimization: smoking cessation, HbA1c <7%, BMI reduction improve outcomes for ventral hernia
- Cooper's ligament (McVay) repair is the only tissue repair that addresses both inguinal and femoral defects simultaneously
Sources: Schwartz's Principles of Surgery 11e (Chapter 37) | Maingot's Abdominal Operations (Chapter 7) | Bailey & Love's Short Practice of Surgery 28e | Current Surgical Therapy 14e | Fischer's Mastery of Surgery 8e | Mulholland & Greenfield's Surgery 7e
How to take case in hernia
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
I have enough material to give a thorough, practical case-taking guide. Here it is:
How to Take a Case in Hernia - Surgery Posting
The standard format: Chief Complaint → History → Examination → Investigations → Diagnosis → Management
PART 1 - PRESENTING COMPLAINT (Chief Complaint)
State it clearly with duration:
"Mr. X, 45-year-old male, presented with a swelling in the right groin for 6 months."
PART 2 - HISTORY OF PRESENTING ILLNESS (HOPI)
About the Swelling - Ask SOCRATES
1. Site
- Which side? Right / Left / Bilateral
- Inguinal (groin)? Scrotal? Umbilical? Femoral region (below inguinal ligament)?
2. Onset
- Sudden or gradual?
- Sudden onset is more concerning - suggests incarceration risk or complication
- Any precipitating event? (heavy lifting, straining, coughing fit)
3. Duration
- Since when?
- Has it been getting bigger over time?
4. Character / Nature of Swelling
- Is it soft or firm?
- Smooth or irregular?
- Any change in size with posture?
5. Reducibility - THE KEY QUESTION
- Does the swelling disappear on lying down? (spontaneous reduction = reducible)
- Can the patient push it back in? (manually reducible)
- Has it ever become irreducible? For how long?
- "Does the swelling go away when you lie down or press it?"
6. Cough Impulse
- Does the swelling appear or increase in size on coughing/straining/standing?
- "Does the swelling become bigger when you cough or stand for long?"
7. Pain / Discomfort
- Is there pain? Dull aching or sharp?
- Worse at end of day / after standing long? (typical for reducible hernia)
- Sudden severe pain = danger sign - may suggest strangulation
- Referred pain to scrotum, inner thigh = nerve compression by sac
8. Aggravating and Relieving Factors
- Aggravated by: standing, walking, coughing, straining, heavy lifting
- Relieved by: lying down, manually reducing
9. Complications - Screen Specifically
Ask about:
- Obstruction signs: Vomiting, absolute constipation, abdominal distension, colicky pain
- Strangulation signs: Sudden onset of severe pain in swelling, swelling that was previously reducible but is now NOT, fever, vomiting, redness/heat over swelling → EMERGENCY
- Urinary symptoms: Difficulty in micturition, frequency (especially if bladder is in sliding hernia)
Precipitating Factors - Ask About Causes of Raised IAP
These are important to mention in your case and determine surgical planning:
| Factor | Ask |
|---|---|
| Chronic cough | Any long-standing cough? Smoker? COPD? |
| Constipation | Any difficulty in passing stools? Straining? |
| Urinary obstruction | Any difficulty in passing urine? (BPH) |
| Ascites | Any abdominal swelling / liver disease? |
| Obesity | BMI |
| Heavy manual work | Occupation? |
| Previous surgery | Any prior abdominal operations? (for incisional hernia) |
PART 3 - PAST HISTORY
- Any previous hernia on either side? Was it operated? When? What type of repair? (important for recurrent hernia)
- Any previous abdominal surgeries? (appendicectomy, laparotomy, colostomy - for incisional hernia)
- Any medical illnesses: DM, COPD, cardiac disease, liver disease/cirrhosis
- Drug history: steroids (wound healing), anticoagulants
- Allergy history
PART 4 - PERSONAL HISTORY
- Occupation: manual labour, heavy lifting (aetiological factor)
- Diet / Bowel habits: constipation?
- Bladder habits: retention, BPH symptoms
- Smoking / Alcohol: smoking = collagen defect, wound infection risk
- Sleep: positional change in hernia size
PART 5 - FAMILY HISTORY
- Hernia has a significant hereditary component - 3-fold increased risk if first-degree relative affected - Schwartz's Principles of Surgery 11e
- Ask: "Does anyone in your family have a similar swelling or hernia?"
PART 6 - GENERAL EXAMINATION (Before Local Examination)
- Built and nourishment: thin elderly woman with groin swelling - think femoral hernia
- Pallor, Icterus, Cyanosis, Clubbing, Lymphadenopathy, Edema (routine PICCLE)
- Vital signs: pulse, BP, temperature (fever in strangulation)
- Note obesity (BMI), any signs of chronic liver disease (for cirrhotic hernia risk), COPD (barrel chest, wheeze)
PART 7 - LOCAL EXAMINATION
A. INSPECTION
Patient should be examined standing first (increases intra-abdominal pressure and makes hernia visible). Then lying down.
Look for:
- Site and extent of swelling - inguinal vs femoral vs scrotal vs umbilical
- Shape and size - rounded, ovoid, elongated (descending into scrotum = indirect inguinal)
- Skin over swelling - normal / erythematous / edematous (red + tender = strangulation)
- Any scars - previous hernia repair scar, laparotomy scar (incisional hernia)
- Asymmetry - compare both sides
- Visible cough impulse - ask patient to cough; visible expansion of swelling = cough impulse present
With patient asked to cough or strain:
- Does the swelling appear or enlarge? = Cough impulse positive - strongly suggests hernia
B. PALPATION
Step 1: Examine with patient lying down first
- Gently palpate the swelling:
- Temperature: normal or raised (raised in strangulation)
- Tenderness: non-tender in reducible; tender in incarceration/strangulation
- Consistency: soft/compressible (reducible), firm/tense (irreducible)
- Surface: smooth
- Edge: well-defined or diffuse
Step 2: Test for Reducibility
- Ask patient to lie down; try gentle pressure to reduce the swelling back into the abdomen
- Reducible hernia: disappears on lying / with gentle pressure
- Note: do NOT forcibly reduce if any doubt about strangulation
Step 3: Deep Ring Occlusion Test (Zieman's Test for type)
- Reduce the hernia (patient lying down)
- Press firmly over the deep inguinal ring (1.25 cm above midpoint of inguinal ligament / mid-inguinal point)
- Ask patient to cough or stand:
- If hernia is controlled = Indirect inguinal hernia (sac has to go through deep ring)
- If hernia reappears despite occlusion = Direct inguinal hernia (comes through Hesselbach's triangle, medial to your finger)
Step 4: Digital Invagination of Inguinal Canal
- Invaginate the scrotal skin with the index finger and push it up into the inguinal canal toward the external ring
- Ask patient to cough:
- Impulse felt at tip of finger = Indirect hernia (sac comes through deep ring, hits finger tip)
- Impulse felt at dorsum (side) of finger = Direct hernia (sac bulges anteriorly from behind)
Step 5: Translucency Test (for scrotal swellings)
- Use a torch: hernia is NOT transilluminant (solid/omentum-containing)
- Hydrocele IS transilluminant - helps distinguish
Step 6: Can you get above the swelling?
- If you cannot get above the swelling = it is coming from the abdomen = hernia
- If you can get above the swelling = it is purely in the scrotum = epididymal cyst, hydrocele of testis, etc.
Step 7: Assess the testis separately
- Feel for the testis separately within the scrotum (is it normal, separate from swelling?)
- In large inguinoscrotal hernia, testis may be difficult to feel separately
C. PERCUSSION
- Hernia containing bowel: resonant on percussion
- Hernia containing omentum or bladder: dull
D. AUSCULTATION
- Listen over the swelling with a stethoscope
- Bowel sounds audible over the swelling = bowel is in the sac (confirms intestinal contents)
- Absent sounds in a tense swelling = may suggest strangulation
E. SPECIAL TESTS (Case Differentials)
| Test | What it tells you |
|---|---|
| Cough impulse | Confirms hernia |
| Reducibility | Reducible vs incarcerated |
| Deep ring occlusion | Direct vs indirect |
| Digital invagination | Direct (dorsum) vs indirect (tip) |
| Transillumination | Hernia (opaque) vs hydrocele (transilluminant) |
| Get above swelling | Cannot get above = inguinoscrotal hernia |
| Femoral site | Swelling below and lateral to pubic tubercle = femoral hernia |
| Zieman's 3-finger test | Index finger on deep ring, middle finger on superficial ring, ring finger on femoral canal - cough impulse at each finger tells which type |
F. REGIONAL LYMPH NODES
- Palpate inguinal lymph nodes - rule out lymphadenopathy as a differential
- Not enlarged in uncomplicated hernia
G. ABDOMINAL EXAMINATION
Always examine the abdomen in hernia cases:
- Distension? (bowel obstruction - strangulation)
- Tenderness, guarding, rigidity? (peritonitis from strangulation)
- Other hernial orifices? (examine all four - inguinal, femoral, umbilical, incisional)
- Always examine the contralateral side for occult hernia
- Digital rectal examination: prostate size (BPH causing straining), rectal malignancy causing raised IAP
PART 8 - PRESENTING YOUR DIAGNOSIS
After examination, present your clinical diagnosis like this:
"On the basis of history and examination, this is a case of [right/left] [direct/indirect] [reducible/irreducible/obstructed/strangulated] inguinal hernia."
Or: "...right inguinoscrotal hernia, most likely indirect inguinal hernia."
PART 9 - INVESTIGATIONS
Routine Preoperative
| Investigation | Purpose |
|---|---|
| CBC | Anemia, leukocytosis (infection/strangulation) |
| Blood glucose (FBS/RBS) | Diabetes - wound healing |
| Renal function tests, electrolytes | Preoperative baseline |
| Chest X-ray | Cardiopulmonary status; chronic cough workup |
| ECG | Preoperative cardiac assessment |
| Blood group and crossmatch | Routine preop |
| Urine routine | Infection, proteinuria |
| LFT, coagulation | If cirrhosis suspected |
| HbA1c | If diabetic - ideally <7% before elective repair |
Specific Investigations
| Investigation | Indication |
|---|---|
| Ultrasound groin | Occult hernia, differential diagnosis, sensitivity 86% |
| CT scan abdomen/pelvis | Large complex hernias, suspected incarceration, recurrent hernias |
| MRI groin | Sports hernia, occult/atypical presentations |
| PSA / urological workup | If BPH/bladder outlet obstruction is a contributing factor |
| Colonoscopy | If change in bowel habits - rule out colonic malignancy as precipitating cause |
PART 10 - MANAGEMENT (Briefly, in Case Presentation)
State:
- Conservative - watchful waiting if asymptomatic, elderly/unfit patient
- Indication for surgery - symptomatic, irreducible, all femoral hernias, all pediatric hernias
- Type of repair - open Lichtenstein mesh repair (gold standard) vs laparoscopic (TEP/TAPP) for bilateral or recurrent
- Anesthesia - local (preferred for open), general (required for laparoscopic)
- Complications to mention - recurrence, chronic pain, testicular atrophy, mesh infection
SUMMARY - HOW TO PRESENT THE CASE (Script)
"Mr. X is a 45-year-old male farmer who presented with a right groin swelling for 4 months. The swelling appears on standing and coughing, reduces on lying down, and is not tender. There is no history of vomiting, constipation, or urinary symptoms. He is a chronic smoker with occasional constipation.
On examination, a 4x3 cm soft, non-tender, reducible, cough-impulse-positive swelling was seen in the right groin above and medial to the pubic tubercle. The swelling was opaque on transillumination. Digital invagination of the inguinal canal showed the impulse at the tip of the finger. The deep ring occlusion test controlled the swelling. The testis was palpable separately in the scrotum. Bowel sounds were heard on auscultation of the swelling. The abdomen was soft and non-tender.
Based on history and examination, this is a case of right indirect inguinal hernia, reducible, with no signs of complications.
I would like to confirm with ultrasound groin if in doubt, obtain routine preoperative investigations, and plan for elective open Lichtenstein tension-free mesh hernioplasty under local/spinal anesthesia."
RED FLAGS - Must Not Miss in Any Hernia Case
| Sign | Significance |
|---|---|
| Suddenly irreducible, previously reducible | Incarceration - urgent surgery |
| Severe pain + tenderness + erythema | Strangulation - emergency surgery |
| Fever + tachycardia + vomiting | Strangulation with systemic sepsis |
| Abdominal distension + absolute constipation | Obstructed hernia |
| Howship-Romberg sign (inner thigh pain) | Obturator hernia |
| Swelling below inguinal ligament in elderly woman | Femoral hernia - repair regardless |
| Change in bowel habits with hernia | Rule out underlying malignancy |
Sources: Schwartz's Principles of Surgery 11e | Maingot's Abdominal Operations | S Das Manual of Clinical Surgery 13e | Bailey & Love's Short Practice of Surgery 28e
I am not getting hopi
Let me give you the HOPI for hernia in a simple, step-by-step conversational format — exactly how you'd ask a real patient in the ward.
HOPI in Hernia - Detailed Breakdown
The chief complaint in hernia is almost always:
"Swelling in the groin / abdomen / scrotum" ± pain
So your entire HOPI revolves around characterizing this swelling and screening for complications.
Step 1 - First, Establish the Swelling Itself
Ask these in order:
1. When did you first notice the swelling?
- This gives you duration
- "How long have you had this swelling?"
- Note: sudden onset is more alarming than gradual
2. How did it start?
- Gradually noticed it one day? Or suddenly appeared after lifting something heavy / coughing episode?
- Precipitating event - heavy lifting, severe coughing, straining at stool
- This establishes the onset and precipitating cause
3. Where exactly is the swelling?
- Patient usually points to the groin / scrotum / umbilicus
- Ask if it is only in the groin or has it gone down into the scrotum
- "Has the swelling come down into your private area / testicle?" → inguinoscrotal hernia
4. What is the size - has it grown?
- Same size since it appeared? Or increasing gradually?
- "Is it the same size as when you first noticed it, or has it grown bigger?"
- Progressive enlargement = hernia is getting worse
5. THE MOST IMPORTANT QUESTION - Does it go away?
This tells you if it is reducible or irreducible.
Ask in simple language:
- "Does the swelling disappear when you lie down?"
- "Can you push it back in with your hand?"
- "Does it come back when you stand up again?"
What the answers mean:
- Swelling disappears on lying down / can push it in = Reducible hernia ✓
- Swelling was going away before but now it doesn't = Newly irreducible = Incarcerated ⚠️ - urgent!
- Swelling never went away from the start = Chronically irreducible
6. Does the swelling appear or become bigger on coughing / straining?
- "Does the swelling come out when you cough, pass stools, or lift heavy things?"
- This is the cough impulse in history
- Yes = classic hernia behavior (raised intra-abdominal pressure pushes contents through the defect)
7. Is there any pain or discomfort?
- Reducible hernia: dull aching / dragging discomfort, worse at end of day after standing, relieved by lying down
- Incarcerated hernia: constant pain in the swelling, not relieved by lying down
- Strangulated hernia: sudden severe pain, continuous, getting worse - emergency
Ask:
- "Is there any pain in the swelling?"
- "Is the pain constant or does it come and go?"
- "Did the pain start suddenly or gradually?"
- "Does it go away when you lie down?"
- Any pain going into the scrotum or inner thigh? → nerve compression (ilioinguinal / genitofemoral nerve)
Step 2 - Screen for Complications (Very Important)
These questions tell you if the hernia is complicated right now.
8. Is the swelling painful and tender NOW?
- "Is the swelling painful to touch right now?"
- Tender + irreducible = incarcerated / strangulated
9. Is there any redness or warmth over the swelling?
- "Has the skin over the swelling become red or hot?"
- Yes = strangulation until proven otherwise → surgical emergency
10. Any vomiting?
- "Have you been vomiting?"
- Vomiting in a patient with irreducible hernia = obstructed / strangulated hernia
- Note: how many times, bilious or not
11. Are you passing stools and gas?
- "Are you passing motions and wind normally?"
- Absolute constipation (no flatus, no stool) = bowel obstruction from hernia = emergency
- This is the single most important question in a patient with irreducible hernia
12. Any fever?
- "Have you had fever?"
- Fever + tense painful hernia = strangulation with systemic sepsis
Step 3 - Ask About Contributing Causes (Why Did This Hernia Form?)
These go at the end of HOPI or in personal/past history - but ask them:
13. Any chronic cough?
- "Do you have a long-standing cough?"
- Chronic cough = chronic raised intra-abdominal pressure = direct cause of hernia
- If yes - ask about smoking, TB, COPD
14. Any difficulty passing stools? Straining?
- "Do you have to strain hard to pass stools?"
- Constipation / straining at stool = raised IAP
15. Any difficulty passing urine? Dribbling?
- "Any difficulty in urination? Do you have to strain to pass urine?"
- Urinary obstruction (BPH, stricture) = raised IAP → causes hernia
- Also important because bladder may be content of a sliding hernia
16. Any previous similar swelling on this side or other side?
- "Have you had this swelling before and was it treated?"
- Previous repair = recurrent hernia
- Bilateral = ask about both sides
17. Any previous abdominal operations?
- "Have you had any surgery on your abdomen before?"
- Prior surgery + swelling at scar site = incisional hernia
How to Put the Whole HOPI Together - Write it Like This
Mr. X, a 45-year-old male, noticed a swelling in the right groin 4 months back. The swelling appeared gradually, without any precipitating event. It is located in the right groin and has gradually increased in size over the past 4 months.
The swelling appears on standing, coughing, and straining and disappears completely on lying down. The patient is able to push it back manually. The swelling is associated with a dull aching discomfort in the right groin, worse after prolonged standing, relieved on lying down. There is no sudden severe pain. The swelling does not become tender.
There is no history of vomiting, no abdominal distension, and the patient is passing stools and flatus normally. No fever.
The patient is a daily laborer doing heavy lifting. He gives a history of chronic cough for 2 years, for which he is not on any treatment. He is a chronic smoker. He gives no history of difficulty in urination, no constipation. No previous surgeries. No similar swelling on the left side.
Quick Summary Table - HOPI Questions and What They Tell You
| Question | What you are finding out |
|---|---|
| When did it start, how? | Duration, onset, precipitating event |
| Where exactly? Gone into scrotum? | Site and extent |
| Bigger over time? | Progression |
| Goes away on lying down? | Reducible vs irreducible |
| Appears on coughing/straining? | Cough impulse history |
| Pain - dull ache vs sudden severe | Uncomplicated vs strangulated |
| Vomiting? | Obstruction / strangulation |
| Passing stools and gas? | Obstruction - most important |
| Fever? Redness? | Strangulation / infection |
| Chronic cough? | Cause of raised IAP |
| Straining at stool / urine? | Cause of raised IAP |
| Previous surgery at same site? | Recurrent hernia |
| Previous abdominal surgery? | Incisional hernia |
The key insight: in HOPI, you are telling the story of the swelling from the day it appeared to today, and along the way you are screening for complications (obstruction and strangulation) which change emergency management completely.
I I need mnemonics ti oearn
Mnemonics for Hernia - Surgery Posting
1. HOPI of Hernia Swelling - "SO CRISP RCA"
Every swelling in surgery is described using these 10 points:
| Letter | Stands for | What to ask |
|---|---|---|
| S | Site | Which groin? Right/left? Gone into scrotum? |
| O | Onset | Sudden or gradual? Any precipitating event? |
| C | Course | Getting bigger over time? |
| R | Reducibility | Goes away on lying down? Can push it back? |
| I | Impulse on cough | Appears/enlarges on coughing, straining? |
| S | Size | Approximate size at first, size now |
| P | Pain | Dull ache vs sudden severe pain |
| R | Related symptoms | Vomiting? Constipation? Fever? Redness? |
| C | Causes (contributing) | Chronic cough? Straining? BPH? Heavy lifting? |
| A | Associated / prior | Previous surgery? Previous hernia repair? |
Recall: "SO CRISP RCA" = the story of any surgical swelling
2. Complications of Hernia - "RIOSS"
| Letter | Complication |
|---|---|
| R | Reducible (normal state - not a complication) |
| I | Irreducible (Incarcerated) |
| O | Obstructed |
| S | Strangulated |
| S | Sliding |
Think of it as a ladder of severity: R → I → O → S
3. Special Types of Hernia - "RLMP"
| Letter | Type | Key point |
|---|---|---|
| R | Richter's | Only antimesenteric wall caught - can strangulate WITHOUT obstruction |
| L | Littre's | Meckel's diverticulum in sac |
| M | Maydl's (W hernia) | Two loops in sac, middle loop strangulates INSIDE abdomen |
| P | Pantaloon | Direct + Indirect together, straddles inferior epigastric vessels |
4. Contents of Inguinal Canal (Spermatic Cord) - "3-3-2-1"
| Number | Contents |
|---|---|
| 3 arteries | Testicular, Cremasteric, Artery of vas deferens |
| 3 veins | Pampiniform plexus, Cremasteric vein, Vein of vas |
| 2 nerves | Ilioinguinal nerve, Genital branch of genitofemoral nerve |
| 1 vas | Vas deferens |
"3 arteries, 3 veins, 2 nerves, 1 vas" - easy to recite!
5. Boundaries of Inguinal Canal - "MALT PIE"
| Letter | Boundary | Structure |
|---|---|---|
| M | ediAL end (deep ring) | Transversalis fascia hiatus |
| A | nterior wall | External oblique Aponeurosis |
| L | ateral/superior wall | Internal oblique + Transversus abdominis (Loup = superior) |
| T | ransversalis | Posterior wall = Transversalis fascia + TA |
| P | oupart's ligament | Floor (Inferior wall) = Inguinal ligament |
| I | nferior exit | Superficial ring = External oblique defect |
| E | xit contents | Spermatic cord (male) / Round ligament (female) |
6. Hesselbach's Triangle - "RIM"
Boundaries of the triangle (site of DIRECT hernia):
| Letter | Boundary |
|---|---|
| R | Rectus abdominis (medial) |
| I | Inferior epigastric vessels (lateral) |
| M | inguinal ligaMent (inferior) |
Direct hernia goes through the RIM
7. Direct vs Indirect - "DIME"
| Direct | Indirect | |
|---|---|---|
| Defect location | Direct through Hesselbach's | Through Deep ring |
| Inferior epigastric | Is medial to it | Is lateral to it |
| Mainly in | Middle-aged / older men | May be in any age, often young |
| Emergency risk | Easy - less strangulation (wide neck) | Elevated strangulation risk |
8. Cough Impulse Test Finger Rule - "DTI"
Dorsum = Direct Tip = indirect
- Impulse at Tip of finger = Indirect (T = T)
- Impulse at Dorsum of finger = Direct (D = D)
9. Femoral Canal Boundaries - "NAVEL"
From lateral to medial, structures under the inguinal ligament:
| Letter | Structure |
|---|---|
| N | Nerve (femoral) |
| A | Artery (femoral) |
| V | Vein (femoral) |
| E | Empty space = femoral canal (where femoral hernia comes through) |
| L | Lymphatics (+ Lacunar ligament medially) |
Femoral hernia comes through the E (empty space = femoral canal)
10. Femoral Hernia vs Inguinal Hernia - "AFIB"
| Feature | Femoral | Inguinal |
|---|---|---|
| Above/Below inguinal ligament | Below | Above |
| Frequency in women | More common in women | Less common in women |
| Incarceration risk | High - always repair | Lower in direct |
| Bone landmark | Lateral to pubic tubercle | Above and medial to pubic tubercle |
11. Causes of Raised IAP (Why hernias form) - "COPS BOP"
| Letter | Cause |
|---|---|
| C | Chronic cough (COPD, TB, smoking) |
| O | Obesity |
| P | Pregnancy |
| S | Straining at stool (Constipation) |
| B | Bladder outflow obstruction (BPH) |
| O | Obstruction (intestinal) |
| P | Previous surgery (incisional hernia) |
12. Repair Types - "BMS - LTR"
Tissue repairs (BMS):
| Letter | Repair |
|---|---|
| B | Bassini |
| M | McVay (Cooper's ligament) |
| S | Shouldice |
Laparoscopic mesh repairs (LTR):
| Letter | Repair |
|---|---|
| L | Lichtenstein (open - gold standard) |
| T | TAPP (Transabdominal preperitoneal) |
| T | TEP (Totally extraperitoneal) |
McVay is the only repair fixing BOTH inguinal AND femoral defects - "McVay covers the whole groin"
13. Screening Questions for Complications - "FAST VP"
When the hernia is irreducible, always ask these:
| Letter | Question |
|---|---|
| F | Fever? |
| A | Abdomen - distension? |
| S | Stools - passing? (absolute constipation = obstruction) |
| T | Tenderness over swelling? Redness? |
| V | Vomiting? |
| P | Pain - sudden severe onset? |
FAST VP = emergency screening in any irreducible hernia
14. Preoperative Investigations - "CBC RULE"
| Letter | Investigation |
|---|---|
| C | CBC (complete blood count) |
| B | Blood glucose / HbA1c |
| C | Coagulation / LFT (if cirrhosis) |
| R | Renal function tests |
| U | Urine routine |
| L | LFT + ECG |
| E | Echo / CXR (if indicated) |
15. Post-op Complications of Hernia Repair - "RUNT HIM"
| Letter | Complication |
|---|---|
| R | Recurrence |
| U | Urinary retention |
| N | Nerve injury (ilioinguinal, iliohypogastric, genitofemoral) |
| T | Testicular atrophy / ischemic orchitis |
| H | Hematoma / seroma |
| I | Infection (wound / mesh) |
| M | Mesh-related chronic pain (CPIIP) |
Quick Recall Sheet
HOPI swelling → SO CRISP RCA
Complications → RIOSS (ladder)
Special types → RLMP
Cord contents → 3-3-2-1
Hesselbach's → RIM
Direct vs Indirect→ DIME
Finger test → DTI (Dorsum=Direct, Tip=indirecT)
Femoral canal → NAVEL
Femoral vs Ing. → AFIB
Causes hernia → COPS BOP
Repair types → BMS + LTR
Emergency check → FAST VP
Pre-op workup → CBC RULE
Post-op compl. → RUNT HIM
Pin this up on your ward shelf - you'll be able to take any hernia case without missing a single point!
This is a shared conversation. Sign in to Orris to start your own chat.