
17830680998696136587022335214655.jpg
What is the treatment for above condition
Reading File
Finding Sources
Searching PubMed
"endometrial hyperplasia" AND "atypical" AND treatment
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is a comprehensive, evidence-based treatment guide for Endometrium - Complex Papillary Hyperplasia with Atypia (also called Endometrial Intraepithelial Neoplasia / EIN in newer nomenclature):
Diagnosis Summary
The pathology report shows Complex Endometrial Hyperplasia with Atypia - a premalignant lesion. Key facts:
- ~29% risk of progression to endometrial carcinoma if untreated
- Up to 40-50% of women with atypical hyperplasia may have a concurrent undiagnosed carcinoma found at hysterectomy
- No definitive invasive carcinoma is seen on this biopsy, but correlation with radiology is advised
Treatment - Based on Fertility Desire
Management Flowchart
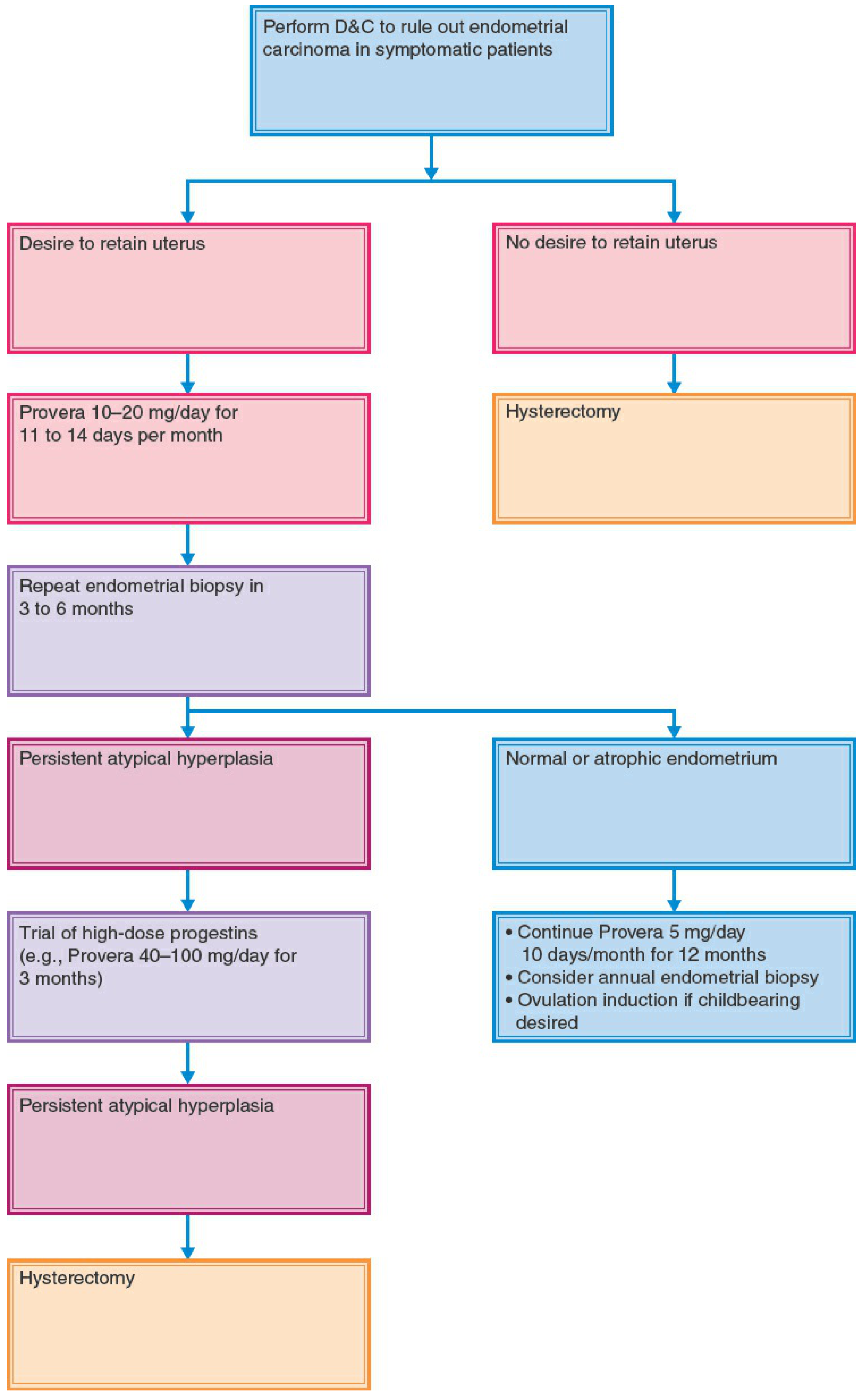
Option A: Does NOT Desire Fertility (Standard / Definitive Treatment)
Total Hysterectomy is the recommended definitive treatment.
- Rules out concurrent carcinoma (present in 25-43% of atypical hyperplasia cases)
- Bilateral salpingo-oophorectomy (BSO) may also be considered
- No further hormonal treatment needed post-operatively if benign at final pathology
"For women with atypical complex hyperplasia who no longer desire fertility, hysterectomy is recommended." - Berek & Novak's Gynecology
Option B: Desires Fertility Preservation (Conservative / Hormonal Treatment)
Step 1 - First-line Progestin Therapy:
| Agent | Dose | Duration |
|---|---|---|
| Megestrol acetate (Megace) | 40-160 mg/day orally (continuous) | 3-6 months minimum |
| Medroxyprogesterone acetate (Provera) | 10-20 mg/day for 11-14 days/month | 3-6 months |
| Levonorgestrel-IUD (Mirena) | Intrauterine insertion | Ongoing |
- Levonorgestrel-IUD is an effective alternative with fewer systemic side effects
- Overall response rate to progestin therapy: ~76%
- Median time to regression: 12 weeks
Step 2 - Follow-up Endometrial Biopsy at 3-6 months:
- If normal/atrophic endometrium: Continue Provera 5 mg/day x 10 days/month for 12 months + annual biopsy. Consider ovulation induction if pregnancy desired.
- If persistent atypical hyperplasia: Escalate to high-dose progestins (Provera 40-100 mg/day for 3 months)
- If still persistent after high-dose: Proceed to hysterectomy
Adjunct - Metformin:
A 2024 meta-analysis (PMID 38503850) supports combining metformin with progestins in atypical hyperplasia - it improves complete response rates and may reduce recurrence.
Special Notes
-
This biopsy specifically states "invasive carcinoma not seen" - but this does NOT exclude carcinoma. Up to 43% of atypical hyperplasia patients are found to have carcinoma at hysterectomy.
-
MRI of the pelvis should be done to evaluate myometrial invasion depth before any fertility-sparing decision.
-
Recurrence after progestin treatment is ~24-50% - most within 1 year. Surveillance is mandatory.
-
Progestin therapy is a temporary bridge, not a definitive cure in atypical hyperplasia - hysterectomy remains the gold standard once fertility is no longer desired.
-
The report advises radiologic correlation - this must be done (MRI pelvis) before finalizing management.
Sources: Berek & Novak's Gynecology (p. 2145-2146); Schwartz's Principles of Surgery, 11th Ed.; Robbins Pathologic Basis of Disease; Cochrane Review 2025 - PMID 40626388; Meta-analysis 2024 - PMID 38503850
Can medical abortion tablet can be given in a patient of seizure disorder
Reading File
Finding Sources
Finding Sources
Searching PubMed
mifepristone misoprostol epilepsy seizure
Finding Sources
Finding Sources
Searching the Web
mifepristone misoprostol medical abortion contraindication seizure disorder epilepsy safety
Reading Web Page
https://societyfp.org/_documents/resources/guidelines2012-2.…
Finding Sources
Finding Sources
Reading File
Reading File
Here is a complete, evidence-based answer:
Medical Abortion (Mifepristone + Misoprostol) in Seizure Disorder - Can it be Given?
Short Answer: Yes, with important precautions - seizure disorder is NOT a contraindication, but drug interactions with antiepileptic drugs (AEDs) must be managed carefully.
Established Contraindications to Medical Abortion
The standard contraindications to mifepristone/misoprostol are:
- Confirmed/suspected ectopic pregnancy
- IUD in place (must be removed first)
- Chronic adrenal failure
- Long-term corticosteroid therapy
- Allergy to mifepristone, misoprostol, or other prostaglandins
- Hemorrhagic disorder / coagulopathy
- Inherited porphyria
Epilepsy/seizure disorder is NOT listed as a contraindication.
- Berek & Novak's Gynecology, p. 781
- Ipas Clinical Guidelines
The Key Issue: Drug Interaction with Enzyme-Inducing AEDs
This is the most clinically significant concern:
Mifepristone is metabolized by CYP3A4. Several AEDs are potent CYP3A4 inducers and will significantly reduce mifepristone plasma levels, potentially reducing its efficacy.
| AED | CYP Induction Effect on Mifepristone |
|---|---|
| Phenytoin | Strongly reduces mifepristone levels |
| Phenobarbital | Strongly reduces mifepristone levels |
| Carbamazepine | Strongly reduces mifepristone levels |
| Oxcarbazepine | Reduces mifepristone levels |
| Valproate, levetiracetam, lamotrigine | Minimal/no CYP3A4 induction - less concern |
"The dose of mifepristone may be increased in patients who take antiepileptic drugs that augment the hepatic P450 system that metabolizes mifepristone (i.e., phenytoin, phenobarbital, carbamazepine, and oxcarbazepine)." - Society of Family Planning Guidelines
Management Recommendations
1. Dose Adjustment
- If the patient is on enzyme-inducing AEDs (phenytoin, phenobarbital, carbamazepine, oxcarbazepine), consider increasing mifepristone dose up to 600 mg (maximum approved safe dose, compared to the standard 200 mg)
- No specific research data define the exact adjusted dose - clinical judgment applies
2. Route of Misoprostol
- Vaginal or buccal misoprostol is preferred over oral in patients with risk factors, as absorption is more reliable
- Misoprostol itself does not lower the seizure threshold in standard doses; no direct seizure risk has been established
3. AED Levels
- The stress of the abortion procedure and associated nausea/vomiting (which can impair AED absorption) may temporarily affect seizure control
- Ensure the patient maintains AED dosing before and after the procedure
- Vaginal/buccal misoprostol avoids GI absorption issues that could impair AED levels
4. Setting
- For women on multiple AEDs or with poorly controlled epilepsy, abortion should be performed in a hospital or supervised clinical setting rather than at home
- Have seizure rescue medications (e.g., benzodiazepines) accessible
5. If Mifepristone is Still a Concern
- A misoprostol-only regimen (800 mcg vaginally, repeated in 24 hours if needed) is an effective alternative, with ~91% complete abortion rate up to 56 days of amenorrhea
- Surgical vacuum aspiration remains the safest option when there is genuine uncertainty about medical management
Summary Table
| Consideration | Recommendation |
|---|---|
| Seizure disorder alone | NOT a contraindication to medical abortion |
| Enzyme-inducing AEDs (phenytoin, carbamazepine, phenobarbital) | Increase mifepristone dose up to 600 mg |
| Non-enzyme-inducing AEDs (valproate, levetiracetam) | Standard 200 mg mifepristone dose |
| Poorly controlled seizures | Hospital-based setting preferred |
| Nausea/vomiting risk with oral AEDs | Use vaginal/buccal misoprostol; monitor AED levels |
| If in doubt | Surgical abortion is the safer alternative |
Sources: Berek & Novak's Gynecology (p. 781); Katzung's Basic & Clinical Pharmacology 16th Ed. (CYP3A4 induction); Society of Family Planning Guidelines - First-trimester abortion in women with medical conditions; Ipas Medical Abortion Contraindications
This is a shared conversation. Sign in to Orris to start your own chat.