Post streptococcal glomerulonephritis
Reading File
Finding Sources
Searching PubMed
"post-streptococcal glomerulonephritis"[MeSH Terms]
Reading File
Finding Sources
Reading File
Finding Sources
Searching Images
post streptococcal glomerulonephritis histology kidney biopsy
Reading File
Loading Image
Reading File
Reading File
Loading Image
I now have comprehensive information to provide a complete answer. Let me compile it:
Post-Streptococcal Glomerulonephritis (PSGN)
Definition & Overview
PSGN is a postinfectious, immune complex–mediated glomerulonephritis that follows skin (impetigo) or throat (pharyngitis) infection by nephritogenic strains of Group A β-hemolytic streptococci (S. pyogenes). Occasionally Groups C or G streptococci are implicated. It is the prototype of the nephritic syndrome and of immune complex glomerulonephritis.
Epidemiology
| Feature | Detail |
|---|---|
| Incidence | ~9/100,000/year in developing countries; declining in developed nations |
| Age | Primarily children 2–18 years; severe adult disease documented |
| Sex | Male : Female = 2 : 1 |
| Form | Epidemic (after pharyngitis outbreaks) or sporadic |
| Subclinical : Clinical ratio | 4–5 : 1 (microscopic hematuria + ↓complement only) |
Pathogenesis
PSGN is an acute immune complex disease:
- Nephritogenic strains of Group A strep produce antigens (e.g., nephritis-associated plasmin receptor [NAPlr], streptococcal pyrogenic exotoxin B [SpeB])
- Host forms antibodies against these streptococcal antigens
- Immune complexes deposit (or form in situ) in glomerular capillary walls
- Complement activation (classic pathway) → consumption of C3 (↓ in >90% of cases)
- Inflammatory response: infiltration of monocytes and PMNs → glomerular injury
Latent Period
| Site of Infection | Latent Period |
|---|---|
| Throat (pharyngitis) | 7–10 days (some say 10–14 days) |
| Skin (impetigo/pyoderma) | 2–4 weeks |
This latent period distinguishes PSGN from IgA nephropathy (which has synpharyngitic hematuria, i.e., concurrent or within 1–2 days).
Clinical Presentation
The classic presentation is acute nephritic syndrome:
| Feature | Details |
|---|---|
| Hematuria | Gross (tea/cola-colored urine) or microscopic; RBC casts pathognomonic |
| Proteinuria | Usually sub-nephrotic; occasionally nephrotic-range |
| Hypertension | Due to sodium/water retention |
| Edema | Facial (periorbital) and peripheral — from salt/water retention |
| Oliguria | Reduced urine output |
| Azotemia | Elevated BUN and creatinine (more common and severe in elderly) |
Rare presentations:
- Nephrotic syndrome
- Rapidly progressive (crescentic) glomerulonephritis
- In elderly: azotemia, heart failure, and nephrotic-range proteinuria predominate
Pathology
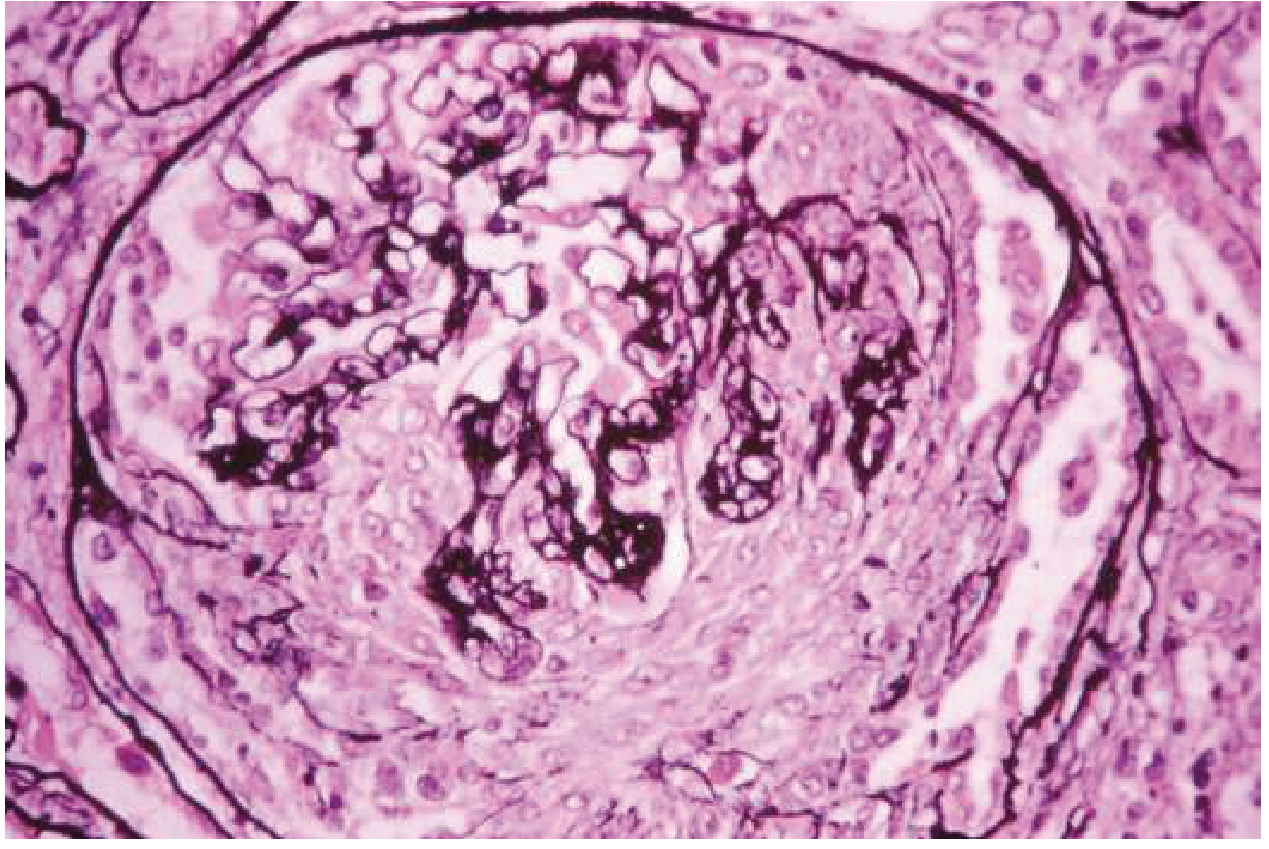
Light Microscopy (Fig. 107-9)
Glomeruli are markedly enlarged, often filling Bowman's space. Key features:
- Diffuse endocapillary hypercellularity — proliferation of mesangial and endothelial cells
- Infiltration by monocytes and polymorphonuclear (PMN) leukocytes
- Compressed capillary lumens
- Occasional extracapillary crescents in severe cases
Immunofluorescence
- Coarse granular ("starry sky") deposits of IgG, IgM, and C3 along capillary walls
- "Hump-like" deposits
Electron Microscopy
- Large, dome-shaped, subepithelial electron-dense deposits ("humps") — pathognomonic
- Also mesangial and subendothelial deposits
Diagnosis
Serological Markers
| Test | Finding |
|---|---|
| ASO (Antistreptolysin O) | ↑ in pharyngitis (>95% positive) |
| Anti-DNase B | ↑ in skin infections (>85% positive); more sensitive for pyoderma |
| Streptozyme panel (ASO + AHT + antistreptokinase + anti-DNase) | Broad coverage |
| Serum C3 | Low in >90% of acute episodes; normalizes in 6–8 weeks |
| C4 | Usually normal (distinguishes from SLE, MPGN type II) |
- Antibody rise occurs 7–14 days after disease onset, peaks at 3–4 weeks
- A rising titer is more indicative than a single high titer
When to Biopsy
Biopsy is rarely necessary if the classic triad is present:
- Acute nephritic episode after documented strep infection
- Rising streptococcal antibody titer
- Depressed serum complement
Biopsy indications:
- Diagnostic doubt
- Complement fails to normalize by 8 weeks (consider MPGN, lupus)
- Rapidly deteriorating renal function
Differential Diagnosis (Other causes of low complement + nephritis)
| Condition | C3 | C4 | Key Distinguishing Feature |
|---|---|---|---|
| PSGN | ↓ | Normal | Post-strep latency, granular IF, humps on EM |
| MPGN Type I/III | ↓ | ↓ | Persistent low C3, double contour on LM |
| SLE nephritis | ↓ | ↓ | Anti-dsDNA, ANA, low C4 |
| Cryoglobulinemia | ↓ | ↓ | Serum cryoglobulins, hepatitis C |
| Endocarditis GN | ↓ | ↓/N | Murmur, positive blood cultures |
| IgA nephropathy | Normal | Normal | Synpharyngitic, mesangial IgA on IF |
Treatment
Active Infection
- If active streptococcal infection is still present: Benzathine penicillin G 1.2 million units IM — treats the infection and prevents spread of the nephritogenic strain
Supportive Management
| Problem | Treatment |
|---|---|
| Volume overload / edema | Loop diuretics (furosemide) + salt restriction |
| Hypertension | Antihypertensives (CCBs, ACEi in non-oliguric patients) |
| Severe oliguria/uremia | Dialysis if necessary |
There is no role for corticosteroids or immunosuppression in uncomplicated PSGN; management is purely supportive.
Prognosis
| Population | Prognosis |
|---|---|
| Children | Excellent — symptoms resolve in 2–7 days; complete recovery in >95% |
| Adults | More guarded — morbidity from pre-existing cardiovascular disease |
| Elderly | Higher risk of azotemia, volume overload, heart failure |
| ESRD | Uncommon unless comorbidities (e.g., diabetes) are present |
| Complement (C3) | Normalizes within 6–8 weeks; failure to normalize suggests alternative diagnosis |
| Hematuria | May persist as microscopic hematuria for months |
| Proteinuria | May persist for 1–2 years |
Key Memory Points
- Mechanism: Immune complex deposition → complement activation → ↓C3 (C4 normal)
- Latency: 1–2 weeks post-pharyngitis; 3–4 weeks post-impetigo
- Classic triad: Hematuria + HTN + edema (nephritic syndrome)
- Pathognomonic EM finding: Subepithelial "humps"
- Best antibody for pyoderma: Anti-DNase B (ASO often negative in skin infections)
- Normalisation: C3 normalizes by 6–8 weeks; if not → consider MPGN or lupus
- Treatment: Penicillin (if infection active) + supportive care only
Sources: Goldman-Cecil Medicine International Edition, Chapters 107 & 269; Brenner and Rector's The Kidney
Minimal change disease
Finding Sources
Searching PubMed
"minimal change disease" AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.