Patient was brought to ER from outside hospital with inferior wall MI, and, uh, on arrival, patient was gasping, and, uh, there was no carotid pulse, and, uh, CPR initiated, and patient was intubated, and, uh, rhythm showed VF, and, uh, uh, we gave shock. After that, again, it was like refractory VF. We gave three shocks, amiodarone infusion was in- started, over 300 mg given, followed by adrenaline every three minutes. Uh, and, uh, uh, suddenly the cardiologist came, and he started giving, uh, told to give atropine and, uh, magnesium sulfate. Uh, why does, why does he say that to give? And, uh, I have this doubt. And after that, uh, he'd done, uh, temporary pacemaker was done, and patient was, uh, ROC obtained, and R adrenaline and adrenaline infusion started, and, uh, and, uh- Uh, patient was shifted to outside hospital, getting AMA. Not willing for admission. Can you explain, like, what about the resuscitation was it correct nd
Overall Assessment: Was the Resuscitation Correct?
Step-by-Step Analysis
1. CPR + Intubation + Rhythm Check - CORRECT
2. Defibrillation for VF - CORRECT
- Defibrillate (200 J biphasic, 360 J monophasic)
- Resume CPR for 2 minutes immediately after - do NOT pause to check rhythm right after shock
- Then reassess
3. Three Shocks Given for Refractory VF - CORRECT
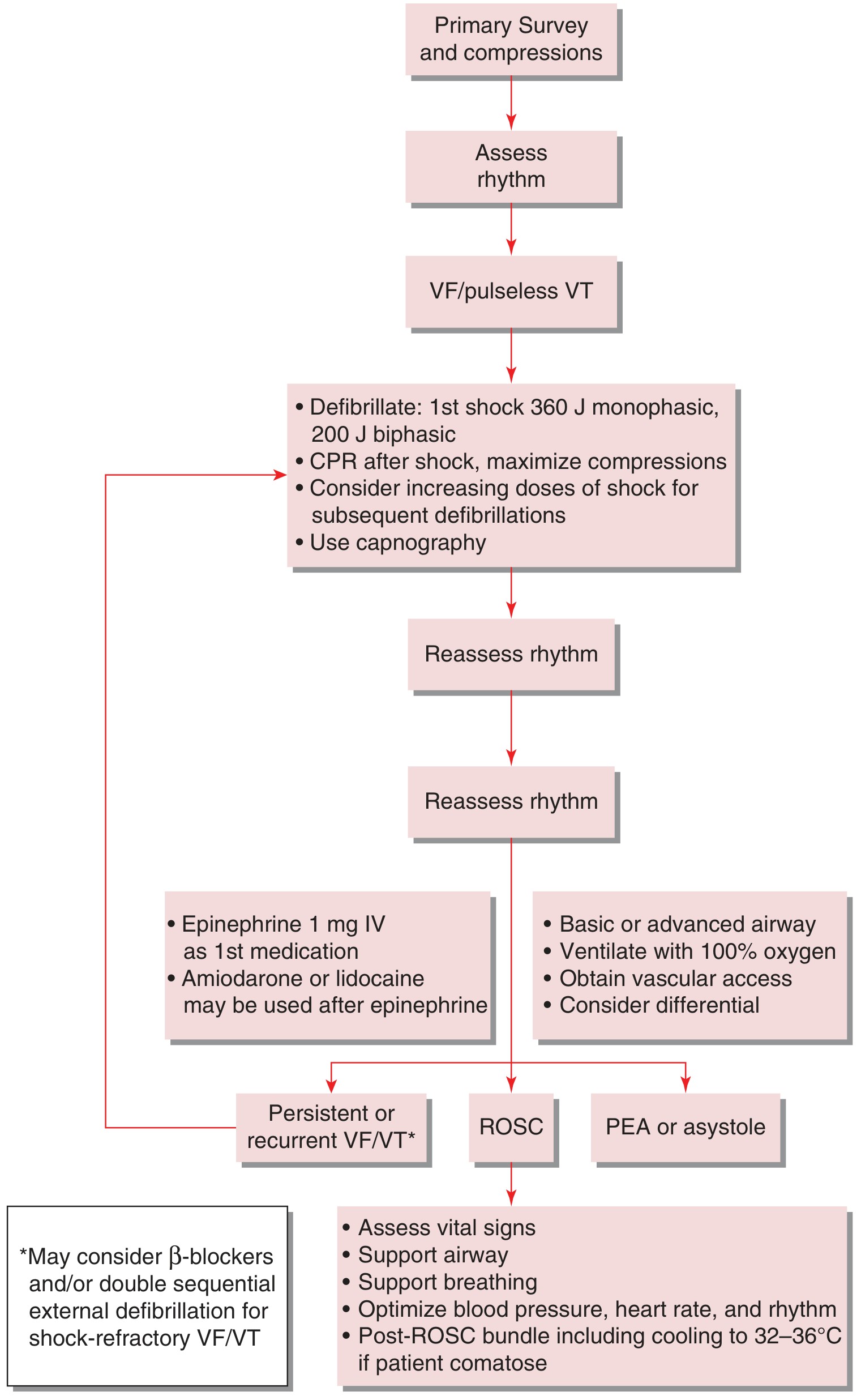
4. Amiodarone 300 mg - CORRECT (with a caveat)
- Dose: 300 mg IV bolus for pulseless VT/VF, followed by a flush. A second 150 mg dose can be given if no response.
- Mechanism: Class III antiarrhythmic with properties of all four Vaughan-Williams classes; lowers defibrillation threshold; causes coronary/peripheral vasodilation.
- Important caveat: A large 2016 multicenter trial (ALPS trial) found amiodarone did NOT improve survival to hospital discharge versus placebo in shock-refractory VF - but it remains in ACLS guidelines as a Class IIb recommendation. (Tintinalli's Emergency Medicine, p. 199)
5. Adrenaline (Epinephrine) Every 3 Minutes - CORRECT
Why Did the Cardiologist Order Atropine and Magnesium?
Magnesium Sulfate - Likely Appropriate
-
Hypomagnesemia - a very common finding in MI patients (especially those on diuretics), which can cause ventricular arrhythmias including VF that is resistant to defibrillation. Hypomagnesemia alone can predispose to torsades de pointes, monomorphic VT, and VF that is resistant to standard therapy. (Rosen's Emergency Medicine, Clinical Features; Brenner and Rector's The Kidney)
-
Torsades de pointes - If the VF was actually torsades (which can look like VF on monitor), magnesium is the treatment of choice.
-
Prolonged QT - In the setting of ischemia, QT prolongation is common, and QT-related VF responds to magnesium.
"Magnesium is initial treatment for torsades de pointes and dysrhythmias secondary to hypomagnesemia, cardiac arrest from QT prolongation, or cardiac glycoside toxicity." - Tintinalli's Emergency Medicine, p. 199
Atropine - This Is Questionable
"Atropine is not recommended for PEA or for treatment of cardiac arrest. It is indicated for symptomatic bradycardia." - Tintinalli's Emergency Medicine, p. 200
- He may have been anticipating that after ROSC, the patient (with an inferior wall MI) would likely have bradycardia or heart block - a very common complication. The right coronary artery (RCA), which is occluded in most inferior MIs, supplies the SA node (~60% of people) and AV node (~90% of people). Post-ROSC bradycardia/complete heart block is expected.
- He may have given atropine preemptively for anticipated post-ROSC bradycardia, not for the VF itself.
- At 0.5 mg IV for bradycardia, it is appropriate. Caution: doses below 0.5 mg can paradoxically cause bradycardia and even precipitate VF.
The Temporary Pacemaker - CORRECT and Well-Reasoned
- Inferior MI + refractory VF + post-ROSC instability = high likelihood of complete heart block (CHB) or severe bradycardia
- The RCA supplies the AV node, so inferior STEMI frequently causes 2nd or 3rd degree AV block
- A temporary transvenous pacemaker provides a reliable, rate-controlled rhythm and is the definitive treatment for refractory bradycardia/AV block in this context
- ROSC was obtained after pacemaker placement - this strongly suggests the underlying issue may have been a bradyarrhythmia degenerating into VF (brady-induced VF), not primary VF
Summary Table
| Intervention | Verdict | Comment |
|---|---|---|
| CPR + intubation | Correct | Standard ACLS |
| Defibrillation x3 for VF | Correct | Shockable rhythm |
| Amiodarone 300 mg | Correct | First-line for refractory VF |
| Epinephrine every 3 min | Correct | Standard dosing (1 mg IV q3-5 min) |
| Magnesium sulfate | Clinically reasonable | For possible hypomagnesemia/torsades/QT-related VF |
| Atropine | Questionable for VF; appropriate for anticipated post-ROSC bradycardia | Not indicated during VF itself |
| Temporary pacemaker | Correct and likely key to ROSC | Inferior MI + AV node ischemia = high block risk |
Key Teaching Points
- Inferior MI + refractory VF should make you think of bradycardia-induced VF - treat the root cause (AV block) with pacing, not just chase the arrhythmia.
- Magnesium is appropriate in refractory VF when hypomagnesemia, torsades, or QT prolongation is suspected - especially in MI.
- Atropine has no direct role in VF management, but is indicated for post-ROSC bradycardia in inferior MI.
- ROSC after pacing in this case strongly suggests the pacemaker was the deciding factor - the prior drugs may have stabilized the myocardium enough for pacing to work.
- The patient leaving AMA after ROSC is a clinical and ethical concern - they needed urgent PCI (primary or rescue) for their inferior STEMI, and leaving without it carries very high re-arrest risk.
While giving first shock pt shouted ahh and checked pulse not there but peripheral pulse was there and breathing was there heart beat with stethoscope heard no lub dub
What You Described: The Three Findings
| Finding | What it means |
|---|---|
| Patient shouted "ahh" when shocked | Patient was conscious |
| Peripheral pulse present | Heart was beating |
| No carotid pulse felt | Likely an assessment error |
| No lub-dub on stethoscope | Possibly aortic stenosis muffle, poor technique, or muffled sounds - but this alone does not confirm cardiac arrest |
The Core Problem: You Shocked a Conscious Patient
"Defibrillation is contraindicated for sinus rhythm, conscious patients with a pulse, or when there is danger to the operator." (Tintinalli's Emergency Medicine, Patient Selection - Defibrillation)
- Conscious
- Breathing
- Had a functioning heart
So What Was Actually Happening? - Possible Explanations
1. The Most Likely: Misdiagnosis - Rhythm Was NOT VF
- CPR artifact - if compressions were still being done when rhythm was checked, it mimics VF
- Loose electrode artifact - movement, shivering, tremor can produce a wavy baseline that looks like VF
- Patient movement - a gasping, agitated patient thrashing can create electrical noise on the monitor
- The actual rhythm may have been sinus tachycardia, SVT, or VT with a pulse
2. Missed Carotid Pulse - Very Common
- The patient is vasoconstricted (inferior MI + shock)
- Low blood pressure makes the pulse weak
- The team is stressed and moving quickly
- Peripheral pulse was present - this is the more reliable finding here
3. Absent Heart Sounds on Stethoscope
- Aortic stenosis (calcified valves - common in elderly MI patients) - the A2 component is absent or soft
- Significant pericardial effusion (muffled heart sounds) - worth considering in MI
- Obesity or thick chest wall making auscultation difficult
- Examiner distraction in a high-stress resuscitation
- The fact that there was a peripheral pulse completely overrides silent auscultation
4. Brief ROSC Before Shock Was Delivered
What Should Have Been Done Differently
Before ANY shock:
- Confirm rhythm on monitor - Is it truly VF? Chaotic, no discernible QRS complexes?
- Check for pulse - Use both carotid AND peripheral (radial/femoral). If peripheral pulse is present, do not shock.
- Check responsiveness - Call patient's name, tap shoulder. A truly pulseless VF patient will be unresponsive and apneic (or only gasping agonally).
- If rhythm is uncertain - use a second lead, reposition electrodes, stop CPR briefly for a clean trace.
- POCUS (bedside ultrasound) - In a modern ER, point-of-care ultrasound during the pulse check window can confirm or deny cardiac activity immediately. This would have resolved all confusion instantly.
If the patient had a pulse and the rhythm was VT (not VF):
- Hemodynamically unstable VT → Synchronized cardioversion (not defibrillation), and always with sedation first unless the patient is truly unconscious
- Hemodynamically stable VT → amiodarone or lidocaine first; cardioversion is elective
Summary: What Likely Happened
- The patient arrived with a rhythm that looked like VF on the monitor (possibly artifact, or VT)
- The pulse check was incorrect - carotid was missed but peripheral pulse was actually present
- The patient was not in true cardiac arrest at the moment of the first shock
- The shock was delivered inappropriately to a conscious patient with cardiac output
- The vocal response confirmed consciousness; the peripheral pulse confirmed cardiac output
Dopamine or norad to be started for this pt? Or dobutamine He is 26yrs old what could be the cause for mi
norepinephrine dopamine cardiogenic shock mortality
myocardial infarction young adults etiology causes
PMID: 37724944
PMID: 20200382
Part 1: Which Vasopressor/Inotrope?
The Short Answer:
Why Not Dopamine?
- No survival benefit of dopamine over norepinephrine overall
- More arrhythmias with dopamine: 24.1% vs 12.4% (p<0.001)
- Critically - in the cardiogenic shock subgroup specifically, dopamine had INCREASED 28-day mortality compared to norepinephrine (p=0.03)
Why Noradrenaline (Norepinephrine)?
- Potent alpha (α1) effect - vasoconstriction, restores MAP and coronary perfusion pressure
- Moderate beta (β1) effect - positive inotropy without excessive tachycardia
- Maintains diastolic BP - critical for coronary perfusion (coronary arteries fill in diastole)
- Safer arrhythmia profile than dopamine in this context
- Dose: Start at 0.05-0.1 mcg/kg/min, titrate to MAP >65 mmHg
When to Add Dobutamine?
| Sign of Low Cardiac Output | Clinical Finding |
|---|---|
| Cool, clammy extremities | Poor peripheral perfusion |
| Urine output <0.5 mL/kg/hr | Renal hypoperfusion |
| Rising lactate | Tissue oxygen debt |
| POCUS showing poor LV squeeze | EF visually reduced |
- Dose: Start 2-5 mcg/kg/min, titrate up to 20 mcg/kg/min
- Warning: Dobutamine causes vasodilation (β2 effect), which can drop BP - always needs norepinephrine alongside it in hypotensive cardiogenic shock
- Do NOT use dobutamine alone if the patient is hypotensive
What About Epinephrine (Adrenaline Infusion)?
Summary Drug Choice:
Hypotensive post-arrest cardiogenic shock:
1. NOREPINEPHRINE (first-line vasopressor)
2. + DOBUTAMINE (if low-output signs present)
3. AVOID dopamine (pro-arrhythmic, increased mortality in cardiogenic shock)
4. AVOID epinephrine infusion if alternatives available (arrhythmia risk)
Part 2: Why MI at 26 Years Old?
Categories to Consider:
🔴 Most Common in Young Adults
- Strong family history of premature CAD (1st-degree relative <55M / <65F)
- Familial hypercholesterolaemia (FH) - autosomal dominant, LDL >190 without treatment
- Diabetes + dyslipidaemia + smoking combined
- Smoking is the single biggest modifiable risk factor in young MI
- Cocaine - causes intense coronary vasospasm AND promotes thrombus formation. Single most important cause of MI in young people in many populations. Even one-time use can be fatal.
- Amphetamines / methamphetamine - same mechanism
- Anabolic steroids - used by young athletes/bodybuilders; cause dyslipidaemia, polycythaemia, hypercoagulability
- Ask specifically - patients often deny but family may disclose
🟡 Non-Atherosclerotic Causes
- Tear in the inner wall of a coronary artery without atherosclerosis
- Most common in young women (20-50 yrs), especially peripartum
- If this patient is female: SCAD is a top diagnosis
- Standard PCI can be dangerous - conservative management often preferred
- Severe transient spasm of a normal coronary artery
- Occurs at rest, often at night
- Associated with smoking, cocaine, cold exposure
- ECG shows transient ST elevation that resolves
- Infective endocarditis - vegetation breaks off into a coronary artery
- Atrial fibrillation / structural heart disease - thrombus from LA appendage
- Patent foramen ovale (PFO) - paradoxical embolism from DVT/PE
- Prosthetic valves, antiphospholipid syndrome
- Antiphospholipid antibody syndrome (APLAS) - very important in young adults
- Polycythaemia vera, essential thrombocythaemia (thrombotic blood disorders)
- Factor V Leiden, Protein C/S deficiency
- Nephrotic syndrome (hypercoagulable)
- OCP use in women (especially combined with smoking - very high risk)
- Anomalous origin of coronary artery (e.g., ALCAPA - left coronary from pulmonary artery)
- Often presents in young adults during exertion
- Missed on standard imaging; requires CT coronary angiography
- History of Kawasaki in childhood causing coronary artery aneurysms
- Aneurysms can develop thrombus decades later
- Takayasu's arteritis (young women, Asian)
- Polyarteritis nodosa
- Lupus (SLE) vasculitis
Practical Workup for This 26-Year-Old
| Test | What you're looking for |
|---|---|
| Fasting lipids, LDL | Familial hypercholesterolaemia |
| Blood glucose, HbA1c | Diabetes |
| Urine drug screen | Cocaine, amphetamines |
| APLA panel (anticardiolipin, anti-β2GP1, lupus anticoagulant) | Antiphospholipid syndrome |
| ANA, anti-dsDNA | Lupus |
| CBC + peripheral smear | Polycythaemia, thrombocytosis |
| Thrombophilia screen (Protein C/S, Factor V Leiden, ATIII) | Hereditary thrombophilia |
| Echocardiogram | Structural abnormality, LV function, vegetations |
| CT coronary angiogram (when stable) | Anomalous origin, SCAD if conventional PCI not done |
| Family history | Premature CAD, FH |
| Social history | Smoking, cocaine, steroids, OCP |
Both norad and adrenaline was started Cardiology gave lidocaine And he also told to bicarbonate and calcium gluconate abg showed ph-7.2 Hco3-18 K-4.5
ABG Interpretation First
| Parameter | Value | Normal | Interpretation |
|---|---|---|---|
| pH | 7.2 | 7.35-7.45 | Acidaemia |
| HCO3 | 18 mEq/L | 22-26 | Low - metabolic component |
| K+ | 4.5 mEq/L | 3.5-5.0 | Normal |
Analysis of Each Drug Ordered
1. Bicarbonate - Partially Justified, But Not Straightforward
"Routine use during cardiac arrest is no longer recommended... In undifferentiated cardiac arrest, sodium bicarbonate does not benefit and may be harmful... The 2015 AHA guidelines recommend against routine use in cardiac arrest." - Tintinalli's Emergency Medicine
- pH 7.2 is significant but not severe enough to meet the "pH <7.1" threshold for automatic bicarbonate use
- HCO3 of 18 is low but not critically so
- K+ is 4.5 - completely normal - removes the hyperkalemia indication
- This is post-ROSC, patient is intubated - this is the most justifiable scenario for bicarbonate
- Produces CO2 internally → worsens intracellular acidosis if ventilation inadequate
- Causes alkalosis → oxyhemoglobin curve shifts left → less O2 delivery to tissues
- Hypernatraemia and hyperosmolality
- Can cause paradoxical CNS acidosis (CO2 crosses blood-brain barrier, HCO3 does not)
- MUST increase ventilator rate after giving bicarb to blow off the CO2 produced
2. Calcium Gluconate - NOT INDICATED. Potentially HARMFUL
- Hyperkalemia (K+ high, threatening cardiac conduction)
- Hypocalcaemia
- Hypermagnesaemia (Mg2+ toxicity)
- Calcium channel blocker overdose
- Beta-blocker overdose (high-dose insulin + calcium protocol)
- Mitochondrial dysfunction
- Activation of proteases and lipases
- Contraction band necrosis
- Cell death
"Calcium is not recommended for routine administration for VF/pulseless VT or PEA."
3. Lidocaine Post-ROSC - Reasonable, Acceptable
- Suppresses recurrent VT/VF - in a post-MI, post-arrest irritable myocardium, a maintenance infusion reduces risk of re-fibrillation
- Alternative if amiodarone already used - some cardiologists use lidocaine as the infusion agent after amiodarone was used for the acute arrest, to avoid cumulative amiodarone toxicity
4. Both Norad AND Adrenaline Running Together - Potentially Problematic
- Noradrenaline: α1 >> β1 - vasoconstriction + mild inotropy
- Adrenaline: β1 + β2 + α1 - strong inotropy + chronotropy + vasoconstriction
- Extreme tachycardia → increases myocardial oxygen demand in an already ischaemic heart
- Severe vasoconstriction → increases afterload → makes the failing LV work harder
- Pro-arrhythmic - both together can re-trigger VF
- Rosen's Emergency Medicine specifically notes: "Recent data suggest epinephrine, alone or with other agents, is associated with an increased risk of death in cardiogenic shock."
Summary: Scorecard for the Cardiologist's Orders
| Drug | Indication Present? | Verdict |
|---|---|---|
| Lidocaine infusion | Yes - post-VF arrest suppression | ✅ Correct |
| Bicarbonate | Borderline - pH 7.2 post-ROSC, intubated | ⚠️ Acceptable but not mandatory; optimise ventilator first |
| Calcium gluconate | No - K+ 4.5 is NORMAL, no other indication | ❌ Not indicated; potentially harmful in MI |
| Both norad + adrenaline | Redundant, pro-arrhythmic combination | ⚠️ Wean adrenaline; use norad + dobutamine instead |
What Should Have Been Done for the ABG
- Check pCO2 on the ABG (you didn't mention it) - is the ventilator compensating correctly? Adjust RR to target pCO2 ~33-37 mmHg
- Treat the cause - the acidosis is from low cardiac output → fix the underlying shock (reperfusion with PCI is the only real cure for this)
- Bicarbonate only if pH remains <7.1 after ventilator optimisation, or if hyperkalemia develops
- Serial ABGs every 1-2 hours to track lactate clearance - rising lactate = worsening shock; falling = responding
Junction rhythm image and what it means while checking for rhthym
junctional escape rhythm ECG example image inferior MI AV node
What is Junctional Rhythm?
Normal Pacemaker Hierarchy
| Pacemaker | Location | Intrinsic Rate |
|---|---|---|
| SA node | Right atrium | 60-100 bpm ← normal |
| AV node / Junction | AV junction | 40-60 bpm ← junctional |
| Bundle of His / Purkinje | Ventricles | 20-40 bpm ← ventricular |
ECG Appearances
Image 1: Junctional escape beat after a PVC pause
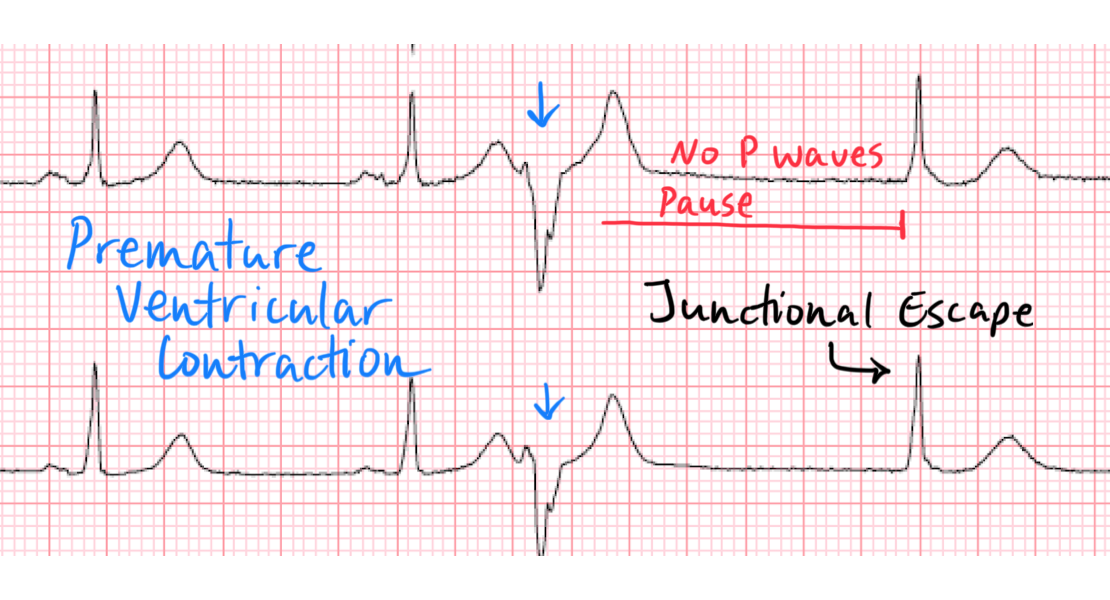
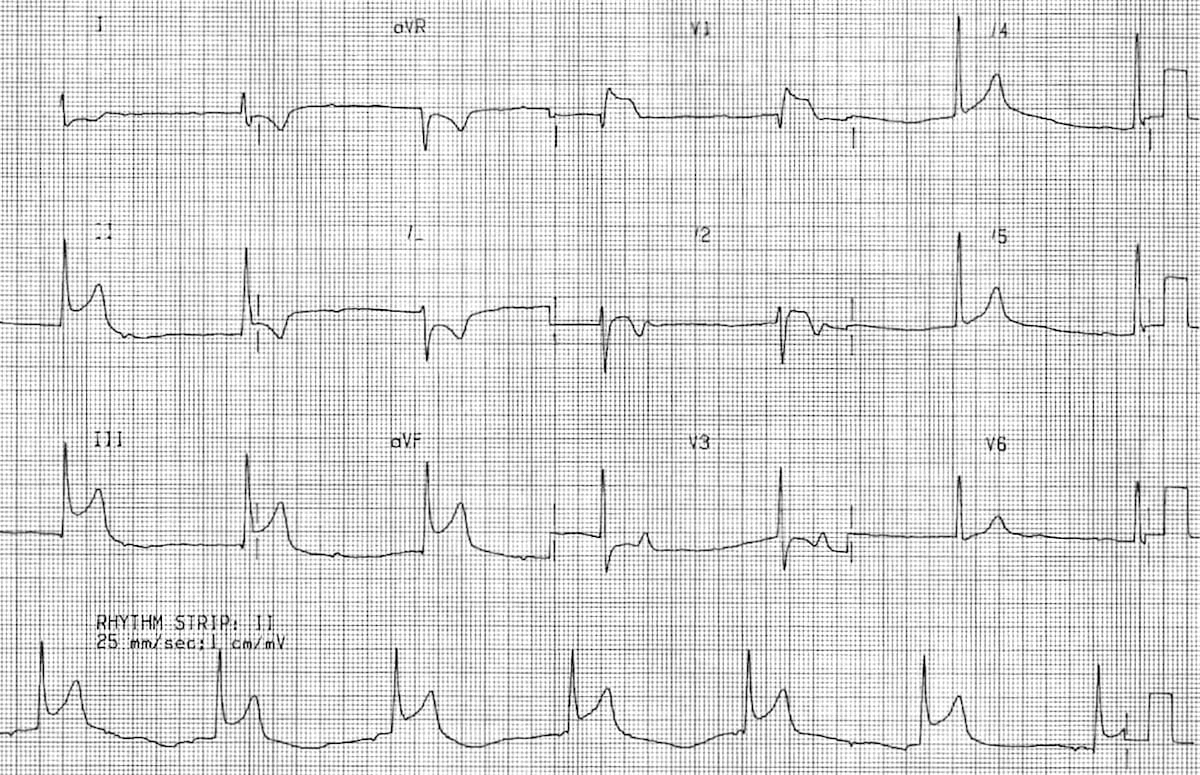
Image 2: Inferior STEMI with sinus node dysfunction and junctional rhythm
ECG Features - How to Recognise It
| Feature | What you see |
|---|---|
| P waves | Absent (most common) - no P waves at all |
| Or | Inverted P wave - immediately before OR after QRS (retrograde conduction back to atria) |
| PR interval | Absent or very short (<0.12 sec if P visible) |
| QRS complex | Narrow (<0.12 sec) - because ventricles activate normally via His-Purkinje |
| Rate | 40-60 bpm (junctional escape) |
| Rhythm | Regular |
Three possible P-wave patterns:
Type A - No P wave at all:
[QRS] [QRS] [QRS] [QRS] ← most common
Type B - Inverted P BEFORE QRS:
[P̂][QRS] [P̂][QRS] ← atria activated first, retrogradely
Type C - Inverted P AFTER QRS:
[QRS][P̂] [QRS][P̂] ← ventricles activated first
Three Types of Junctional Rhythm by Rate
| Type | Rate | Meaning |
|---|---|---|
| Junctional escape rhythm | 40-60 bpm | SA node failed - AV node taking over protectively |
| Accelerated junctional rhythm | 60-100 bpm | AV node has increased automaticity |
| Junctional tachycardia | >100 bpm | Pathologically enhanced AV node firing |
What Does Junctional Rhythm Mean in YOUR Patient?
"The junctional escape rhythm in this case is most likely the result of an inferior myocardial infarction in the distribution of the right coronary artery, which supplies the SA and AV nodes. Possible underlying conduction disturbances include sinus arrest, sinus bradycardia, and heart block."
- SA node in ~60% of people
- AV node in ~90% of people
- SA node ischaemia → slows or stops → no sinus P waves
- AV node ischaemia → blocks conduction OR escapes at 40-60 bpm
- Result: Junctional rhythm appears
- The heart HAD electrical activity (this is NOT asystole)
- The SA node was suppressed or failing due to RCA territory ischaemia
- The AV node was firing as an escape mechanism at 40-60 bpm
- The ventricles were responding normally (narrow QRS)
- But the slow rate (40-60) was likely causing haemodynamic compromise
- This slow junctional rate is what likely degenerated into VF - bradycardia-induced VF is a recognised mechanism in inferior MI
Why This Matters for Management
| Finding on Rhythm Check | Action |
|---|---|
| Junctional rhythm + pulse present | This is NOT a shockable rhythm - do NOT defibrillate |
| Junctional rhythm + haemodynamically unstable | Atropine 0.5 mg IV, then temporary pacing |
| Junctional rhythm + no pulse (junctional PEA) | CPR + epinephrine, treat as PEA, consider pacing |
| Junctional converting to VF | Shows the slow rate was the trigger - pacing is the cure |
Junctional vs Idioventricular - Don't Confuse Them
| Feature | Junctional Rhythm | Idioventricular Rhythm |
|---|---|---|
| QRS width | Narrow (<0.12 sec) | Wide (>0.12 sec) |
| Rate | 40-60 bpm | 30-50 bpm |
| Origin | AV node / Bundle of His | Ventricle itself |
| P waves | Absent or retrograde | Absent |
| Significance | AV node is still working | Very low backup, dangerous |
| Shockable? | No | No |