congenital anomalies of heart in adults
Reading File
Finding Sources
Finding Sources
Searching PubMed
"congenital heart disease" AND adults
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive content and images. Let me compile the full, detailed answer.
Congenital Heart Disease in Adults
An estimated 2.4 million people live with congenital heart disease (CHD) in the United States, and two thirds of them are adults. This represents a dramatic shift - the median age of patients with severe lesions has risen from childhood to late adolescence and beyond, driven by advances in surgical and medical care. Adult care providers now commonly manage these patients alongside cardiologists and tertiary referral centers.
- Goldman-Cecil Medicine, p. 604-615
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 503-510
Epidemiology
- CHD is diagnosed in ~1% of births; prevalence is 3-4 per 1000 adults
- ~300,000 Americans have severe CHD (two or more abnormalities, typically with cyanosis at birth)
- ~20% of CHD is associated with a chromosomal syndrome or anomaly
- The most common CHD in adults, in order of prevalence:
| Lesion | % of all CHD |
|---|---|
| Bicuspid aortic valve | ~2% of general population; most common |
| Atrial septal defect (ASD) | 30-40% of adult CHD |
| Ventricular septal defect (VSD) | 15-20% overall (less prevalent in adults due to high spontaneous closure) |
| Patent ductus arteriosus (PDA) | 5-10% |
| Pulmonary stenosis / Coarctation | 3-10% each |
| Tetralogy of Fallot | Most common cyanotic CHD in adults |
Genetic Basis
- ~20% of CHD is associated with a chromosomal syndrome
- Down syndrome (trisomy 21): ~50% have endocardial cushion defects and VSDs
- Trisomy 13/18: VSDs in ~90%
- Turner syndrome (45,X): aortic coarctation, aortic stenosis, ASD
- 22q11 deletion (DiGeorge/CATCH-22): ~15% of Tetralogy of Fallot patients
- Familial CHD: offspring/sibling recurrence risk is 2-10x baseline
Classification
CHD is broadly divided into:
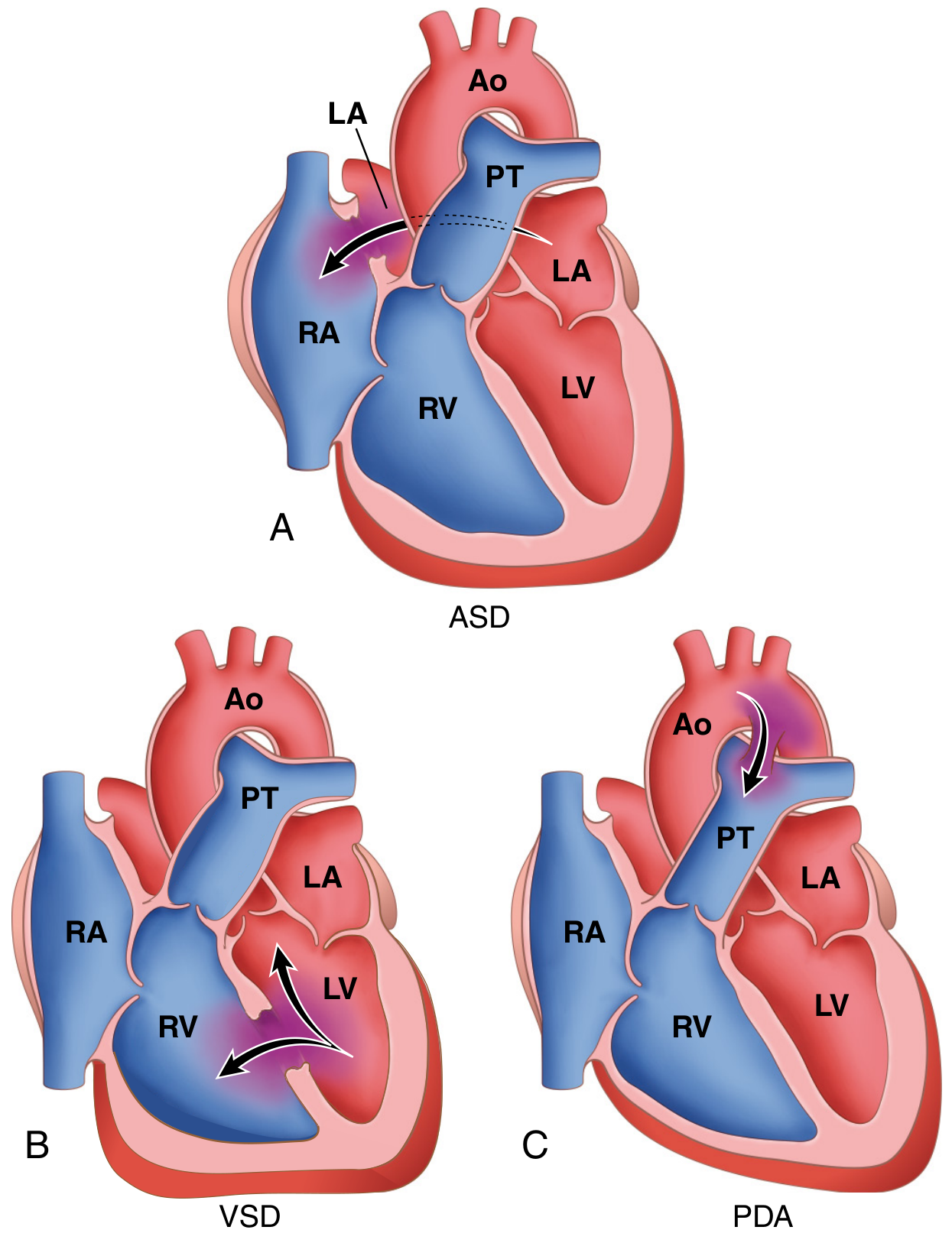
1. Left-to-Right Shunts (Acyanotic)
Initially produce volume overload; can progress to pulmonary hypertension and shunt reversal (Eisenmenger physiology).
2. Right-to-Left Shunts (Cyanotic)
Cause cyanosis early in postnatal life.
3. Obstructive Lesions
Without shunting; pressure overload on the relevant chamber.
Specific Lesions
Atrial Septal Defect (ASD)
Types:
- Secundum (90%) - near center of atrial septum; usually isolated
- Primum (5%) - near AV valves; often associated with AV valve and VSD abnormalities
- Sinus venosus (5%) - near SVC entry; can have anomalous pulmonary venous return
Hemodynamics: Left-to-right shunt; pulmonary flow may be 2-8x normal. ASDs are well tolerated and usually asymptomatic before age 30.
Clinical features in adults:
-
70% become impaired by the 5th decade
- Exercise intolerance, dyspnea, fatigue (RV failure, pulmonary HTN)
- Atrial arrhythmias (AF, flutter), stroke, paradoxical embolism
- Classic auscultation: Wide and fixed splitting of S2 (pathognomonic); soft midsystolic ejection murmur at 2nd left interspace; mid-diastolic murmur at lower left sternal border (high-flow tricuspid)
- ECG: Incomplete right bundle branch block (rSr' pattern); right axis deviation; prolonged PR; AF
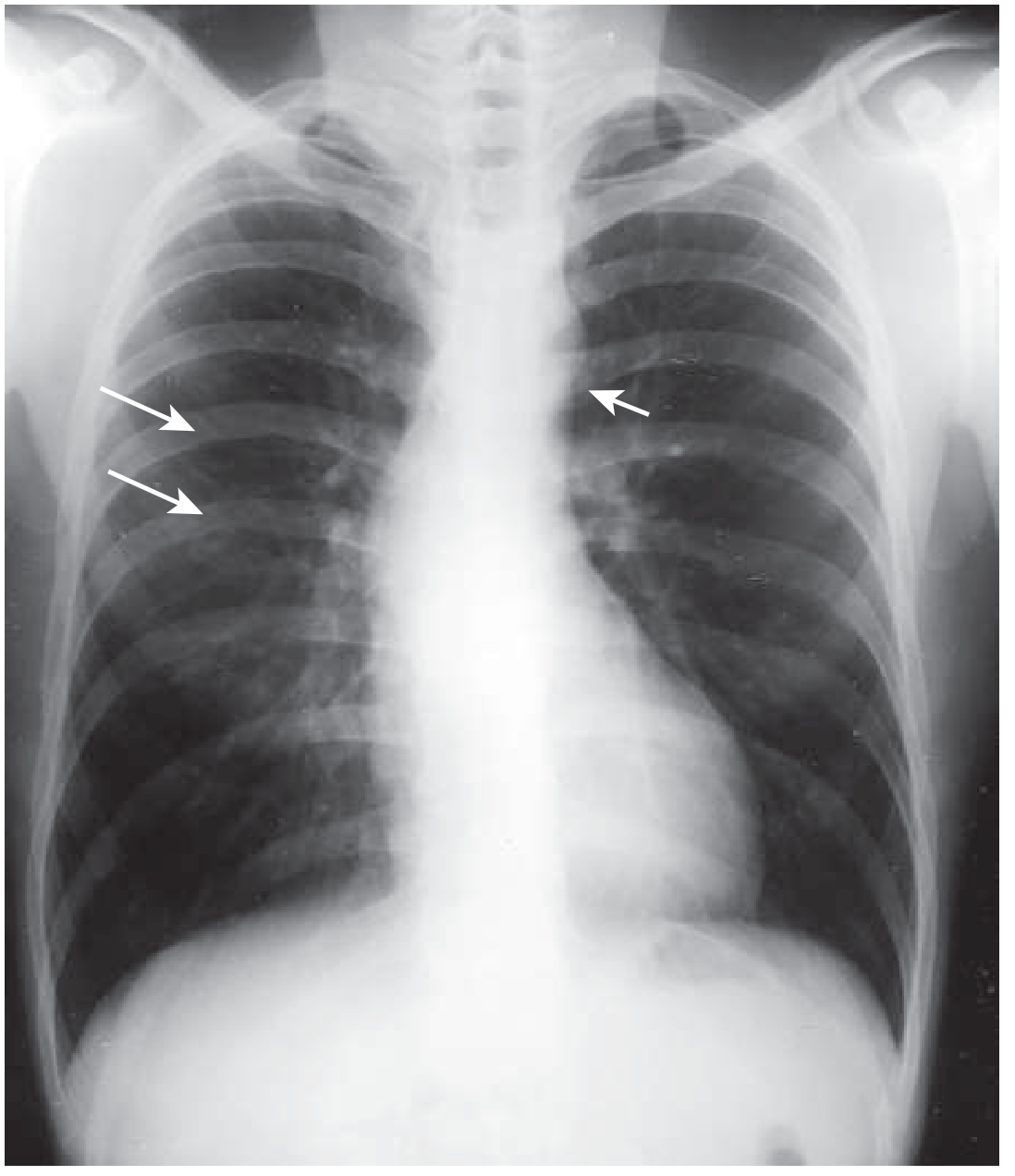
- CXR: Pulmonary plethora, dilated pulmonary arteries, RA and RV enlargement
- Diagnosis confirmed by: Echocardiography (transthoracic for secundum/primum; TEE needed for sinus venosus)
Treatment:
- Closure (percutaneous or surgical) when right-sided heart enlargement is present, with or without symptoms
- Transcatheter device closure for centrally located ASD or PFO up to 3.5 cm
- Closure before age 25 gives long-term outcomes similar to matched controls; still beneficial at age 60+
- Contraindicated if severe irreversible pulmonary vascular disease (PVR > systemic)
Patent Foramen Ovale (PFO)
- Foramen ovale fails to close permanently in ~20% of people
- Not detectable on physical exam or ECG at rest
- Risk of paradoxical embolism with transient right-sided pressure rises (Valsalva, coughing)
- Diagnosis: TEE with agitated saline (bubble study) during Valsalva
- Closure reduces recurrent cryptogenic stroke; not recommended for migraine headache
Ventricular Septal Defect (VSD)
Types by location:
- Membranous/perimembranous (80%) - beneath aortic valve; most common
- Infundibular/supracristal - above crista supraventricularis, below pulmonary valve
- Inlet defects - at crux; associated with AV canal anomalies
- Muscular - may be multiple; can close spontaneously
Adults with VSD: Usually an isolated defect when first detected in adulthood (associated complex anomalies typically present earlier).
Hemodynamics by shunt size:
- Small (Qp:Qs <1.5): Normal PA pressure and resistance; well tolerated; endocarditis risk
- Moderate (Qp:Qs >1.2): Elevated PA pressure but normal resistance; LA and LV dilation
- Large (Qp:Qs ≥1.5): High PA pressure AND elevated resistance; risk of Eisenmenger syndrome
Clinical features:
- Holosystolic murmur at left sternal border; thrill with larger defects
- With large shunts: biventricular failure, cyanosis if Eisenmenger syndrome develops
Spontaneous closure: ~50% of small muscular VSDs close; highest rate in first decade; unusual in adult life.
Treatment: Closure for moderate-to-large VSDs with Qp:Qs >1.5 and elevated PA pressure (but not irreversible pulmonary vascular disease).
Patent Ductus Arteriosus (PDA)
- Ductus arteriosus should close within 1-2 days after birth (structurally obliterated within months)
- ~7% of CHD; 90% are isolated defects
- Classic murmur: Loud continuous "machinery" murmur (systole + diastole), often with thrill, heard at left infraclavicular area
Hemodynamics: Left-to-right shunt (aorta → pulmonary artery); no cyanosis initially. With large shunts: volume overload, pulmonary hypertension, and eventual shunt reversal with differential cyanosis (lower limbs cyanosed and clubbed; upper limbs spared - because right-to-left flow enters aorta distal to subclavian origin).
Treatment: All isolated PDAs should be closed; options include NSAIDs (in infants), percutaneous coil/device occlusion, or surgical ligation.
Coarctation of the Aorta
- Discrete narrowing of the aorta, usually at the level of the ductus arteriosus (juxtaductal)
- Associated with bicuspid aortic valve (~50%), Turner syndrome
Clinical presentation in adults:
- Hypertension in the upper extremities; diminished or absent femoral pulses
- Differential blood pressure between arms and legs (>20 mmHg)
- Radial-femoral pulse delay
- Continuous murmur over the back (collateral circulation)
CXR findings:
- "3 sign" - dilated subclavian artery above and poststenotic aorta below
- Rib notching (inferior surface of posterior ribs 4-8) due to intercostal collaterals
Treatment: Balloon dilation ± stenting (percutaneous preferred in adults); surgical repair for complex anatomy. Early repair reduces but does not eliminate lifelong cardiovascular risk (residual hypertension, aortic complications).
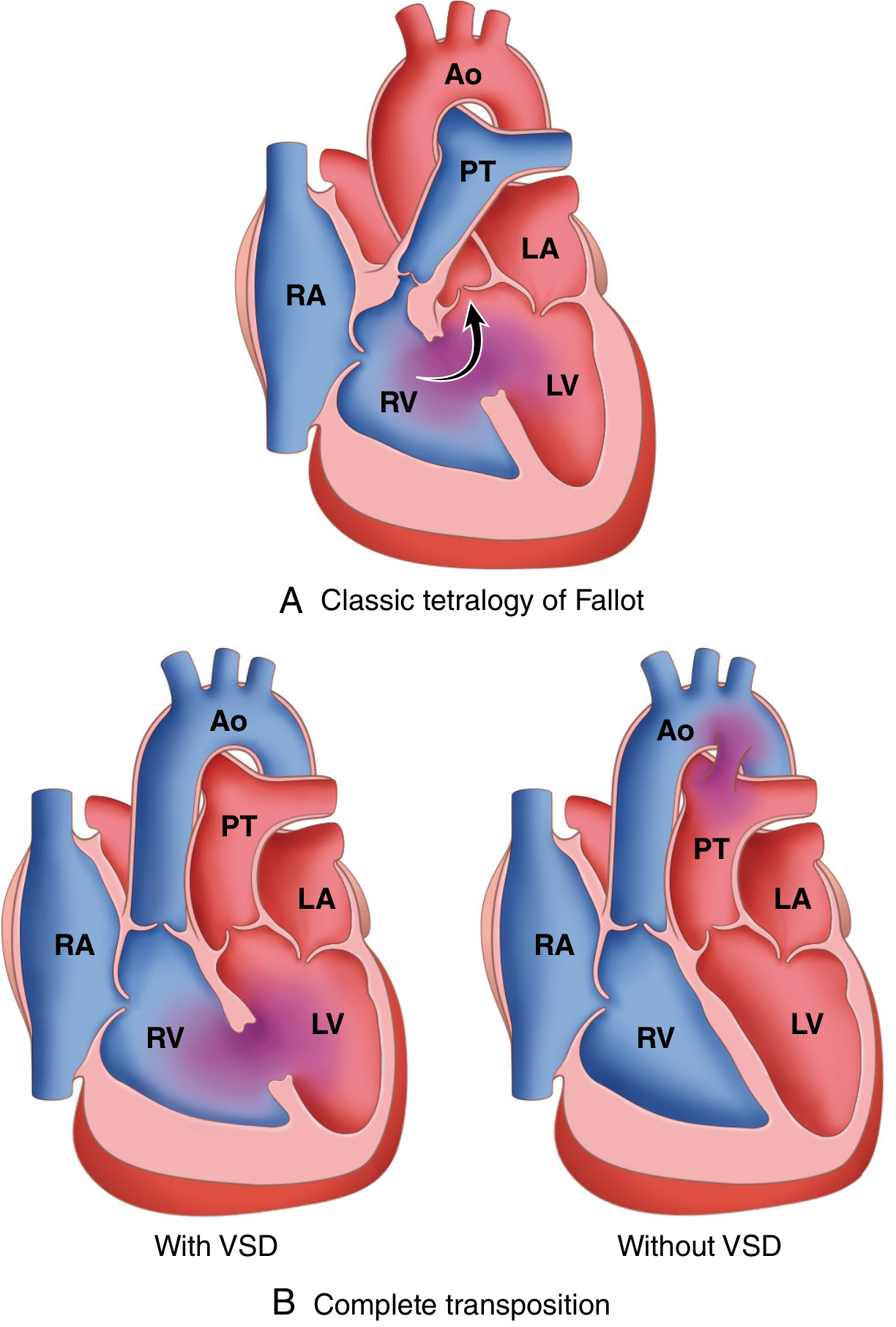
Tetralogy of Fallot (TOF)
The most common cyanotic CHD in adults. Results from anterosuperior displacement of the infundibular septum.
Four features:
- Large VSD
- Subpulmonic stenosis (RVOT obstruction)
- Overriding aorta (aortic valve overrides the VSD)
- Right ventricular hypertrophy (secondary to pressure overload)
Classic CXR: Boot-shaped heart (coeur en sabot) due to marked RVH and upturned cardiac apex; pulmonary oligemia.
Clinical course: Degree of cyanosis depends on severity of subpulmonic stenosis. Most adults presenting now had corrective surgery in childhood. Post-repair complications include:
- Pulmonary regurgitation (most common late complication after transannular patch repair)
- Right ventricular dilation and failure
- Ventricular arrhythmias and sudden cardiac death
- Residual RVOT obstruction or VSD
- Atrial and ventricular arrhythmias (particularly right bundle branch block + left anterior fascicular block = "bifascicular block on steroids" pattern)
Tet spells (hypercyanotic episodes) - paroxysmal hyperpnea, worsening cyanosis, syncope; triggered by crying, feeding, exertion. Treatment: knee-chest position, morphine, propranolol, phenylephrine.
Bicuspid Aortic Valve
- Present in ~2% of the general population - the most common congenital cardiac anomaly in adults
- Accounts for up to half of all surgical aortic stenosis cases in adults
- Associated with thoracic aortic aneurysm (ascending aorta); inherent aortic wall weakness regardless of valve function
- Complications: progressive aortic stenosis, aortic regurgitation, infective endocarditis, aortic dissection
Eisenmenger Syndrome
- Long-standing large left-to-right shunt (ASD, VSD, PDA, AVSD) → irreversible pulmonary arterial hypertension → shunt reversal to right-to-left → cyanosis
- Once established, correction of the underlying defect is contraindicated
- Complications: polycythemia, hyperviscosity, paradoxical embolism, hemoptysis, right heart failure, sudden death
- Treatment: PAH-targeted therapy (endothelin antagonists, PDE-5 inhibitors, prostacyclin analogues); lung transplantation is the only cure
Other Lesions Encountered in Adults
| Condition | Key Features |
|---|---|
| Pulmonary stenosis | Exertional dyspnea, RVH; systolic ejection murmur at 2nd left interspace; ejection click; percutaneous balloon valvuloplasty is effective |
| Ebstein anomaly | Apical displacement of tricuspid valve; massive RA enlargement; WPW in ~25%; "Ebstein's ECG": tall P waves, incomplete RBBB, accessory pathway |
| Congenitally corrected TGA (L-TGA) | Morphologic RV serves as systemic ventricle; progressive systemic RV failure; complete heart block over time |
| Coronary artery fistulas | Arise from RCA or LCA, drain to RV/RA/PA; continuous murmur; angina from coronary steal |
| Sinus of Valsalva aneurysm | Rupture causes sudden continuous murmur, biventricular failure; requires urgent repair |
| Anomalous coronary origins | Left main from right sinus (most dangerous): sudden death in young adults during exercise; coronary course between aorta and PA determines prognosis |
Principles of Management in Adults
General principles:
- All adults with complex CHD should be managed at centers with specialized ACHD expertise (ACC/AHA classification: Simple, Moderate, Complex)
- Endocarditis prophylaxis is recommended for: unrepaired cyanotic CHD; CHD repaired with prosthetic material within 6 months; repaired CHD with residual defects at/near patch; prior endocarditis
- Anticoagulation: Rate/rhythm control for AF; anticoagulate when appropriate; INR target per valve type
- Pregnancy: High-risk in Eisenmenger syndrome (maternal mortality up to 50%), Marfan with dilated aorta, systemic ventricular dysfunction; ACHD team should guide counseling
- Exercise: Tailored to lesion severity; isometric exercise generally avoided in obstructive/cyanotic lesions
Regular surveillance includes: ECG, Holter monitoring, echocardiography, cardiac MRI (especially post-TOF repair for RV volumes/function), 6-minute walk test, CPET.
Sources: Goldman-Cecil Medicine (International Edition), pp. 604-615 | Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 503-510 | Sabiston Textbook of Surgery, 21e
This is a shared conversation. Sign in to Orris to start your own chat.