Axis in ecg
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have all the core material needed for a thorough answer. Here is a complete overview of ECG axis:
ECG Axis
What is the Electrical Axis?
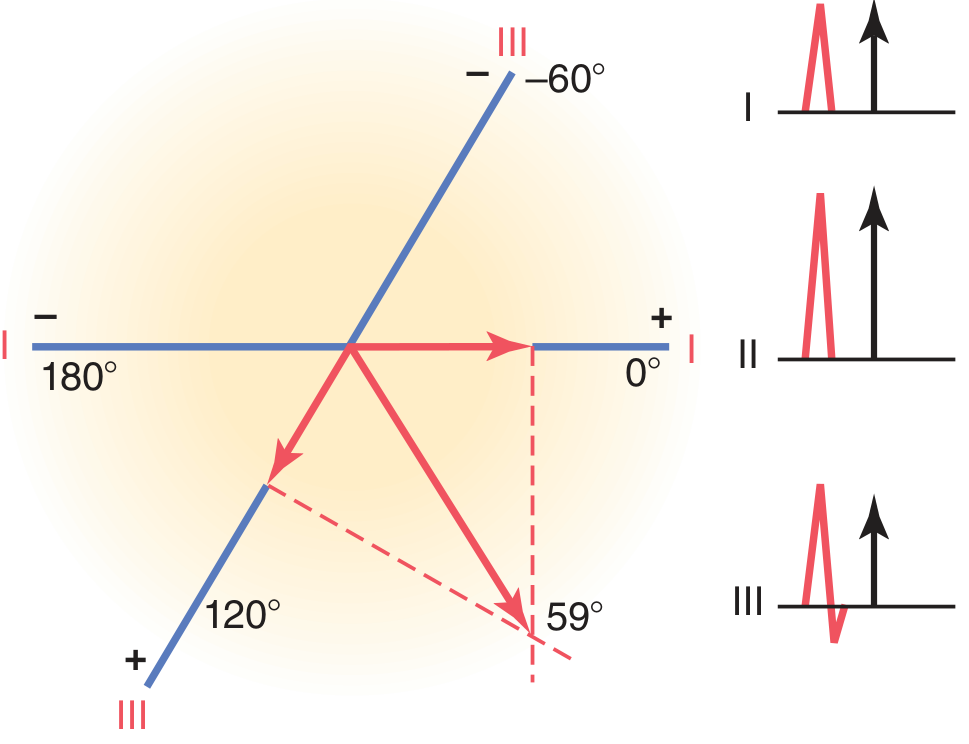
The mean electrical axis of the heart is the average direction of the electrical force (vector) generated during ventricular depolarization (the QRS complex). It represents the net direction of current flow through the ventricles and is expressed as a degree on the frontal plane.
In a normal heart, the apex of the ventricles lies inferiorly and to the left. Because depolarization travels from the base toward the apex, the mean electrical axis in a normal heart points downward and to the left - typically around +59° (normal range: -30° to +90°).
The Hexaxial Reference System
All six frontal plane leads (I, II, III, aVR, aVL, aVF) are arranged around a circle at 30° intervals. This is the hexaxial reference system:
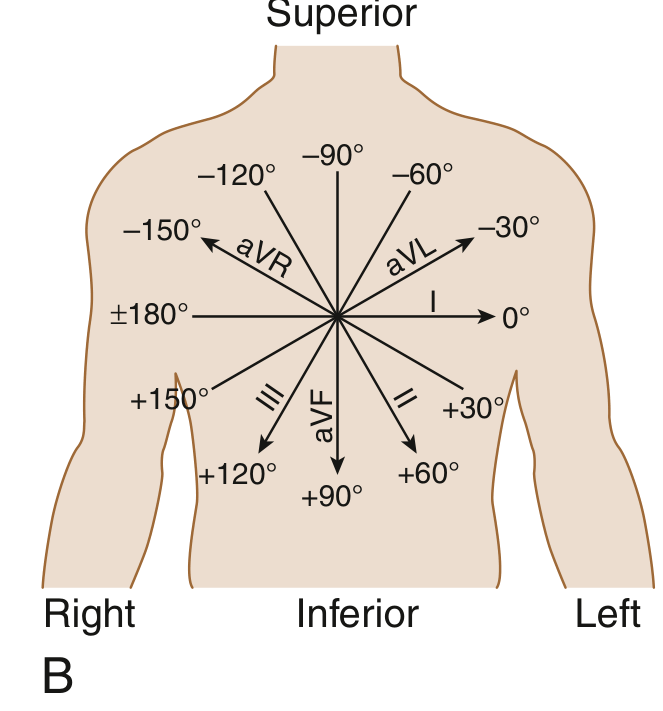
- Lead I = 0°
- Lead II = +60°
- Lead III = +120°
- aVF = +90°
- aVL = -30°
- aVR = -150°
Axis Ranges and Classification
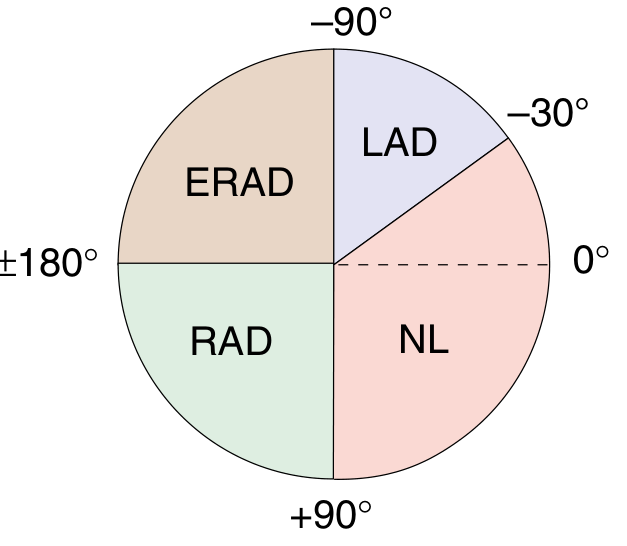
| Axis | Range | Notes |
|---|---|---|
| Normal | -30° to +90° | Average ~+59° |
| Left Axis Deviation (LAD) | -30° to -90° | Moderate: -30 to -45°; Marked: -45 to -90° |
| Right Axis Deviation (RAD) | +90° to +180° | Moderate: +90 to +120°; Marked: +120 to +180° |
| Extreme/Northwest Axis (ERAD) | -90° to ±180° | Also called "no man's land" |
Mild RAD (+90° to +110°) can be a normal variant, especially in children, adolescents, and young adults.
How to Calculate the Axis
Method 1 - Vectorial Method (Lead I + III)
- Measure the net QRS deflection (positive minus negative) in lead I and lead III.
- Plot these values on their respective axes.
- Drop perpendiculars from each point.
- The intersection of the perpendiculars gives the apex of the mean electrical vector.
Method 2 - Quick "Isoelectric Lead" Method
- Find the lead where the QRS is most isoelectric (equal positive and negative deflections - net = 0).
- The mean axis is perpendicular to that lead.
- Then check whether the QRS is positive or negative in the perpendicular lead to confirm direction.
Method 3 - Lead I + Lead aVF (Quadrant Method)
This is the fastest bedside method:
| Lead I | Lead aVF | Axis |
|---|---|---|
| Positive | Positive | Normal (0° to +90°) |
| Positive | Negative | Possible LAD (-30° to 0°) - check aVL |
| Negative | Positive | RAD (+90° to ±180°) |
| Negative | Negative | Extreme axis (northwest) |
Causes of Axis Deviation
Left Axis Deviation (LAD)
- Left anterior fascicular block (LAFB) - most common cause of marked LAD in adults (axis more negative than -45°)
- Left ventricular hypertrophy (LVH)
- Inferior MI (loss of inferior depolarization forces)
- Left bundle branch block (LBBB)
- Wolff-Parkinson-White syndrome (certain accessory pathways)
- Primum ASD (ostium primum - characteristic finding)
- Physiological: obesity, pregnancy, deep expiration (heart rotates horizontal)
Right Axis Deviation (RAD)
- Right ventricular hypertrophy (RVH) - e.g., pulmonary hypertension, pulmonary stenosis, tetralogy of Fallot
- Left posterior fascicular block (LPFB) - rare as an isolated finding
- Lateral MI (loss of lateral LV forces)
- Right bundle branch block (RBBB)
- Wolff-Parkinson-White (left-sided accessory pathway)
- Physiological: tall thin individuals, deep inspiration, neonates/infants (normal until ~6 months)
- Dextrocardia
Extreme Axis Deviation (Northwest Axis)
- Ventricular tachycardia
- Severe RVH
- Artificial pacing
- Hyperkalemia
- Misplaced limb leads
Axis Deviation from Bundle Branch Blocks
- LBBB - shifts axis to the left
- RBBB - shifts axis to the right (right axis deviation)
- Left anterior fascicular block (LAFB) - marked LAD (more negative than -45°) with small q in I/aVL, small r in II/III/aVF
- Left posterior fascicular block (LPFB) - RAD (more than +110-120°) with small r in I/aVL, small q in II/III/aVF - diagnosis of exclusion
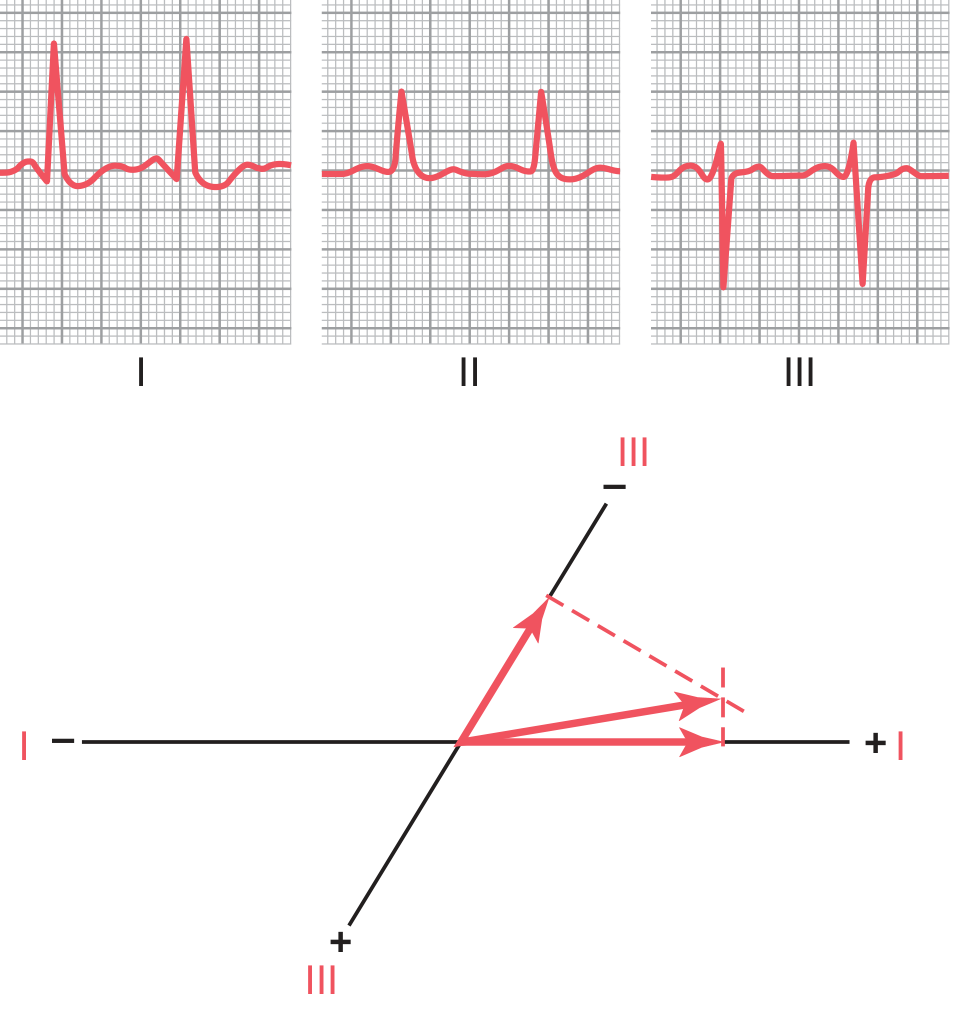
The ECG below shows left axis deviation from left ventricular hypertrophy, with vectorial analysis demonstrating the mean axis at -15°:
Clinical Significance Summary
| Finding | Key Associations |
|---|---|
| LAD | LAFB, LVH, inferior MI, LBBB, primum ASD |
| RAD | RVH, pulmonary HTN, LPFB, lateral MI, RBBB |
| Extreme axis | VT, pacemaker rhythm, hyperkalemia |
| Neonatal RAD | Normal (RV dominant at birth) |
Sources:
- Guyton and Hall Textbook of Medical Physiology, p. 156-158
- Harrison's Principles of Internal Medicine 22E, Chapter 247
- Goldman-Cecil Medicine, Chapter 42
Ecg interpretation
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive material for a complete ECG interpretation guide. Here is the full reference:
ECG Interpretation - A Systematic Guide
The ECG Paper
Before interpreting, understand the grid:
- Small square = 1 mm = 0.04 sec (40 ms) horizontally; 0.1 mV vertically
- Large square = 5 mm = 0.20 sec (200 ms) horizontally; 0.5 mV vertically
- Standard recording speed = 25 mm/sec; standard calibration = 10 mm = 1 mV
- A standard ECG records 10 seconds across 12 leads
The ECG Waveforms

| Wave/Interval | Represents |
|---|---|
| P wave | Atrial depolarization |
| PR interval | Atrial depolarization + AV node conduction delay |
| QRS complex | Ventricular depolarization |
| ST segment | Plateau phase of ventricular action potential (isoelectric) |
| T wave | Ventricular repolarization |
| QT interval | Total ventricular depolarization + repolarization |
| U wave | Possibly slow repolarization of Purkinje fibers (small, same direction as T) |
Atrial repolarization is NOT seen on a normal ECG because it is buried within the QRS complex.
Stepwise Approach to ECG Interpretation
A systematic approach prevents missing findings (Goldman-Cecil Medicine):
Step 1 - Rate
Normal rate: 50-100 bpm (physiologically, 50-90 bpm at rest)
Quick methods:
- Regular rhythm: Divide 300 by the number of large squares between two R waves
- 1 box = 300 bpm, 2 = 150, 3 = 100, 4 = 75, 5 = 60, 6 = 50
- Irregular rhythm: Count the number of QRS complexes in a 10-second strip × 6
- Formula: HR = 60,000 ÷ RR interval (in ms)
| Rate | Interpretation |
|---|---|
| < 60 bpm | Bradycardia |
| 60-100 bpm | Normal |
| > 100 bpm | Tachycardia |
Step 2 - Rhythm
Is it regular or irregular?
- Check RR intervals - are they equal?
- Regularly irregular vs. irregularly irregular (e.g., atrial fibrillation)
Identify the pacemaker:
- Is there a P wave before every QRS?
- Are the P waves upright in leads I, II, aVF? (Sinus origin)
- Normal sinus rhythm: upright P in II, I, aVF; inverted in aVR
Common rhythms:
| Rhythm | Key Feature |
|---|---|
| Normal sinus | P before every QRS, rate 60-100, P upright in II |
| Sinus bradycardia | Same as above, rate < 60 |
| Sinus tachycardia | Same as above, rate > 100 |
| Atrial fibrillation | No clear P waves, irregularly irregular QRS |
| Atrial flutter | Sawtooth P waves at ~300/min, regular QRS (often 2:1 block) |
| Junctional rhythm | Inverted or absent P waves, rate 40-60 |
| Ventricular rhythm | Wide QRS, no P, rate 20-40 |
Step 3 - Intervals
Normal ECG intervals (Goldman-Cecil Medicine):
| Parameter | Normal Range |
|---|---|
| P wave duration | < 120 ms (< 3 small squares) |
| PR interval | 120-200 ms (3-5 small squares) |
| QRS duration | 75-110 ms (< 3 small squares) |
| QTc | Males: 390-450 ms; Females: 390-460 ms |
PR Interval
- Short PR (< 120 ms): Pre-excitation (WPW), accelerated AV conduction, junctional rhythm
- Long PR (> 200 ms): 1st degree heart block (AV node disease, digoxin, beta-blocker, inferior MI)
- Progressively lengthening PR until dropped beat: 2nd degree Mobitz I (Wenckebach)
- Constant PR with dropped beats: 2nd degree Mobitz II (more serious - infranodal)
- No relationship between P and QRS: 3rd degree (complete) heart block
QRS Duration
- > 120 ms (3 small squares): Bundle branch block or ventricular origin
- RBBB: rSR' (rabbit ears) in V1, wide slurred S in I and V6
- LBBB: Broad notched R in I, aVL, V5-V6; QS or rS in V1; no septal q
- Fascicular blocks: Axis deviation only, QRS < 120 ms
Bundle Branch Block Criteria (Goldman-Cecil Medicine):
| Condition | QRS | Axis | V1 Morphology | Lateral leads |
|---|---|---|---|---|
| LAFB | < 120 ms | -45° to -90° | Normal | qR in aVL |
| LPFB | < 120 ms | +90° to +180° | Normal | rS in I, aVL; qR in III, aVF |
| RBBB | ≥ 120 ms | Normal | rsr'/rSR' in V1 | Wide S in I, V5-V6 |
| LBBB | ≥ 120 ms | Variable | QS or rS in V1 | Wide notched R in I, aVL, V5-V6 |
QT Interval - Corrected QT (QTc)
Bazett's formula:
$$QTc = \frac{QT}{\sqrt{RR}}$$
(where QT and RR are both in seconds)
- Normal QTc: Males < 450 ms; Females < 460 ms
- Prolonged QTc > 500 ms: High risk for Torsades de Pointes
- Causes of prolonged QT: Hypokalemia, hypomagnesemia, hypocalcemia; drugs (amiodarone, sotalol, quinolones, macrolides, antipsychotics, tricyclics); congenital long QT syndromes; hypothyroidism; hypothermia
- Short QT: Hypercalcemia, digoxin toxicity, congenital short QT
Step 4 - Axis
(Covered in detail in the previous session)
| Axis | Range |
|---|---|
| Normal | -30° to +90° |
| LAD | -30° to -90° |
| RAD | +90° to +180° |
| Extreme (NW) | -90° to ±180° |
Quick check: If QRS is positive in both Lead I and Lead II, the axis is normal.
Step 5 - P Wave Morphology
- Normal P wave: < 120 ms duration, < 2.5 mm amplitude, upright in I, II, aVF; inverted in aVR
- P-pulmonale (Right atrial overload): Tall peaked P waves ≥ 2.5 mm, best seen in lead II
- P-mitrale (Left atrial abnormality): Broad bifid P wave ≥ 120 ms in lead II (M-shaped); biphasic P with broad negative component in V1
Step 6 - QRS Morphology
Normal R-wave progression (precordial leads):
- V1: Small r, deep S (rS pattern)
- V2-V3: Transitional
- V3-V4: Transition zone (R = S)
- V5-V6: Tall R, small or absent S
Abnormalities:
- Poor R-wave progression (loss of R waves V1-V4): Anterior MI, LBBB, LVH, COPD
- Clockwise rotation (transition at V5 or later): COPD, RVH
- Counterclockwise rotation (transition at V2 or earlier): LVH, normal variant
Pathological Q waves:
- Duration ≥ 40 ms (1 small square) OR amplitude > 25% of R wave height
- Indicate transmural infarction or scar (appear hours to days after MI; may persist)
- Q waves are normal in aVR, III, V1 (septal q waves in V5-V6 are normal)
Voltage criteria:
- LVH: S in V1 + R in V5 or V6 > 35 mm (Sokolov-Lyon); R in aVL > 11 mm
- RVH: R > S in V1; right axis deviation; persistent S waves V5-V6
Step 7 - ST Segment
The ST segment is normally isoelectric (flat at baseline).
| Finding | Significance |
|---|---|
| ST elevation ≥ 1 mm in limb leads or ≥ 2 mm in precordial leads | STEMI, Prinzmetal angina, pericarditis, Brugada, LBBB, LV aneurysm |
| ST depression | NSTEMI/UA, subendocardial ischemia, RVH, digoxin effect |
| Saddle-shaped ST elevation (diffuse, with PR depression) | Pericarditis |
| Coved ST elevation in V1-V2 + RBBB morphology | Brugada pattern |
STEMI territories:
| Territory | Leads with ST elevation | Culprit artery |
|---|---|---|
| Inferior | II, III, aVF | RCA |
| Anterior | V1-V4 | LAD |
| Lateral | I, aVL, V5-V6 | LCx |
| Posterior | ST depression V1-V3 (reciprocal); tall R in V1 | RCA or LCx |
| Right ventricle | V3R, V4R | RCA (proximal) |
Step 8 - T Waves
- Normal: Same polarity as QRS; upright in I, II, V3-V6; inverted in aVR (always)
- Peaked (hyperacute) T waves: Hyperkalemia; earliest sign of STEMI
- Inverted T waves: Ischemia, RVH strain (V1-V3), LVH strain (V5-V6), RBBB/LBBB (secondary changes), pulmonary embolism (V1-V4 inversion + S1Q3T3)
- Wellens pattern: Deep symmetric T inversion in V2-V3 = critical proximal LAD stenosis (high-risk finding)
- Flattened T waves: Hypokalemia, early ischemia
U waves: Small deflection after T wave (best seen V2-V3). Prominent U wave = hypokalemia. Inverted U wave = ischemia or LVH.
Normal 12-Lead ECG - Example
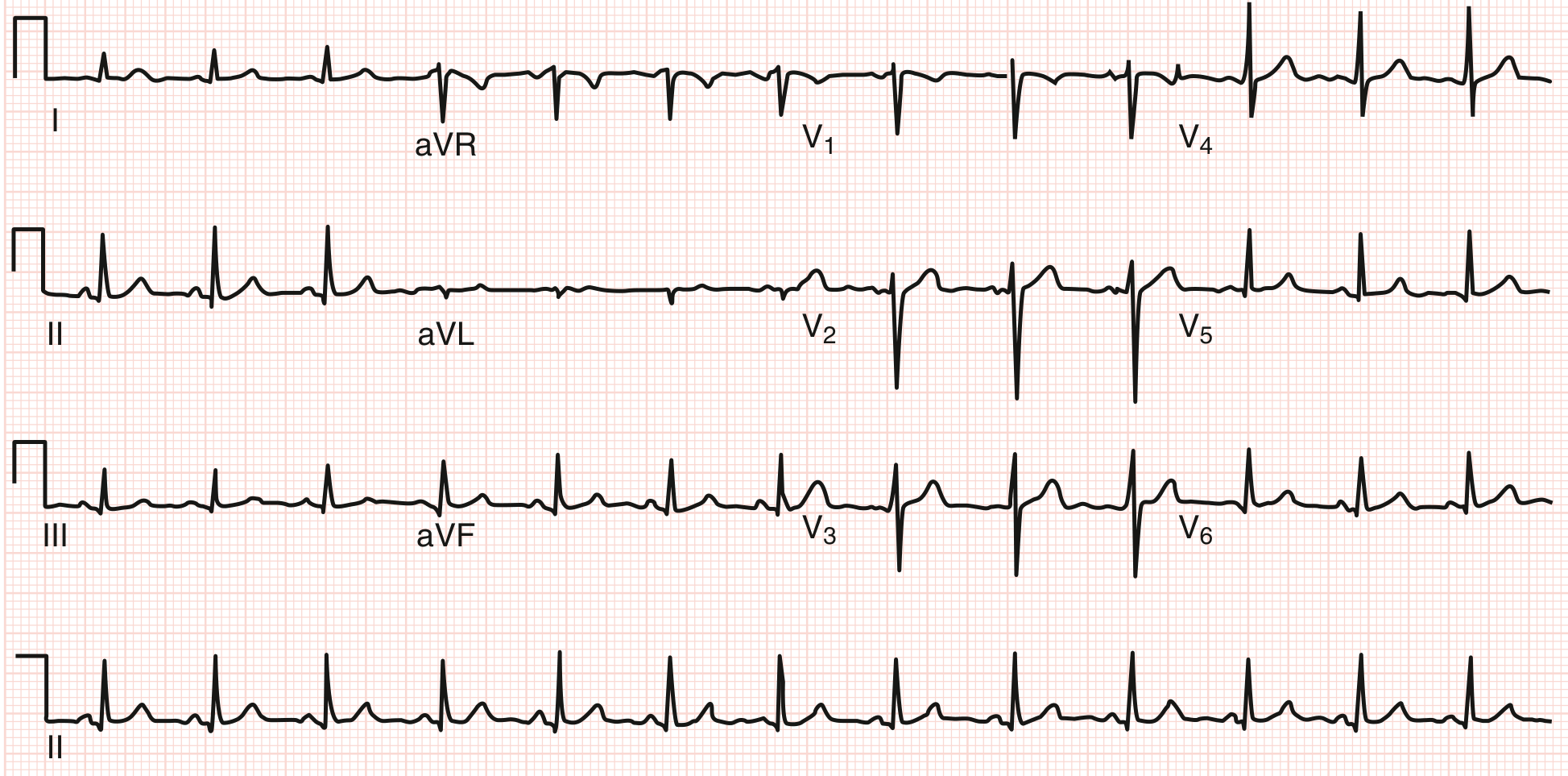
Normal ECG: sinus rhythm, regular rate, normal intervals, normal axis, normal R-wave progression.
Summary Checklist
1. RATE - Calculate from RR interval (bradycardia / normal / tachycardia)
2. RHYTHM - Regular or irregular? P before every QRS?
3. PR INTERVAL - 120-200 ms? Short (WPW)? Long (heart block)?
4. QRS DURATION - < 110 ms? Wide (BBB, pacemaker, hyperkalemia)?
5. QT INTERVAL - Calculate QTc; is it prolonged?
6. AXIS - Normal (-30° to +90°)? LAD? RAD?
7. P WAVE - Morphology: pulmonale, mitrale?
8. QRS MORPHO - Q waves? R progression? Voltage (LVH/RVH)?
9. ST SEGMENT - Elevation or depression? Which territory?
10. T WAVES - Inverted? Hyperacute? Wellens?
11. U WAVES - Prominent (hypokalemia)?
Sources:
- Goldman-Cecil Medicine, Chapter 42 (Electrocardiography)
- Costanzo Physiology 7th Edition, Chapter 4
- Harrison's Principles of Internal Medicine 22E, Chapter 247
- Guyton and Hall Textbook of Medical Physiology, Chapter 12
This is a shared conversation. Sign in to Orris to start your own chat.