Giddiness under evaluation
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Now I have a thorough picture from multiple textbooks. Let me compile the comprehensive answer.
Giddiness (Dizziness) Under Evaluation
"Giddiness" is the lay term for dizziness - a broad, imprecise symptom. The first task in evaluation is to characterize exactly what the patient means by it, because the word covers four mechanistically distinct conditions that have completely different differentials and workups.
Step 1 - Characterize the Symptom
Ask: "What does it feel like when you are dizzy?"
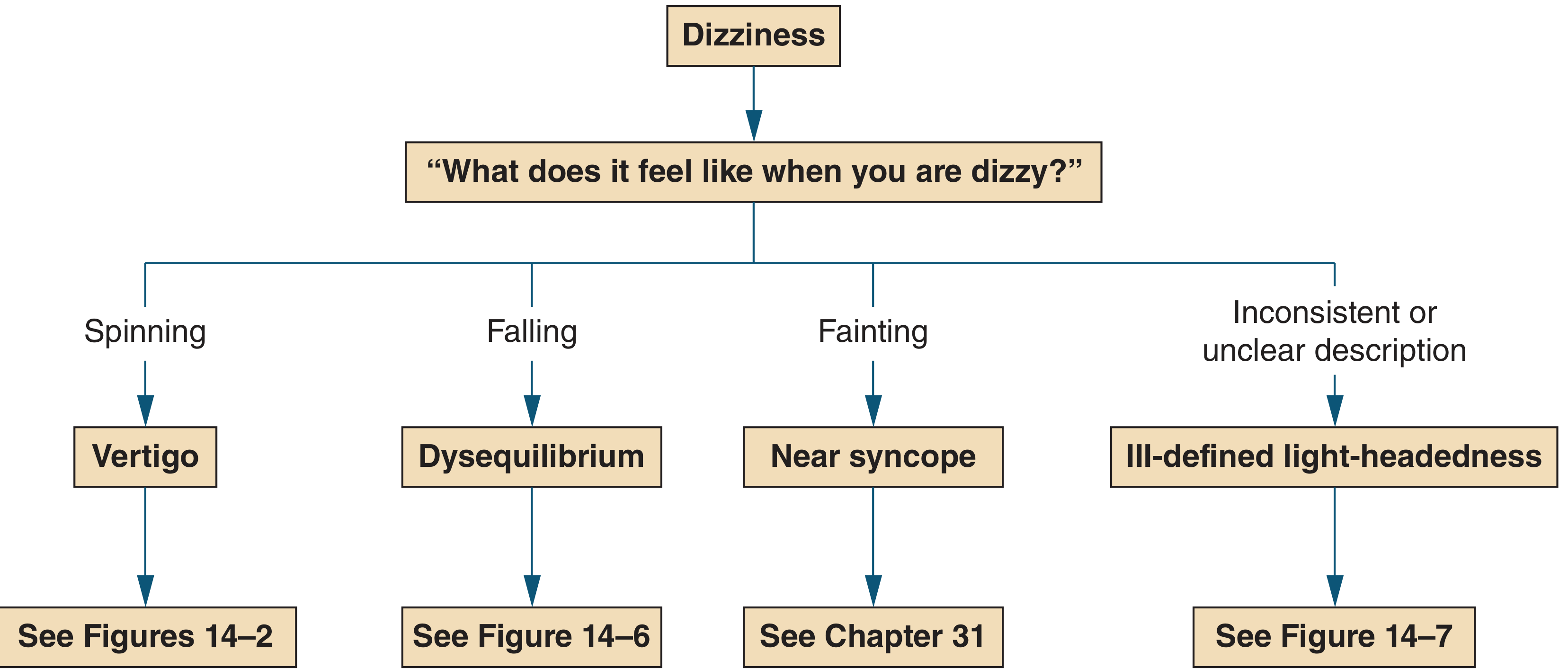
Diagnostic approach to dizziness (Symptom to Diagnosis, 4th Ed.)
| Type | Patient's Description | Trigger | Differential |
|---|---|---|---|
| Vertigo | Spinning, sense of self-motion | Head movement, turning in bed | BPPV, vestibular neuritis, Meniere's, brainstem/cerebellar stroke, MS |
| Near syncope | Impending loss of consciousness, faintness | Standing up, exertion | Orthostatic hypotension, arrhythmia, aortic stenosis, vasovagal, hemorrhage |
| Dysequilibrium | Falling, imbalance, unstable walking | Walking | Parkinson's, cerebellar disease, B12 deficiency, neuropathy, NPH |
| Ill-defined light-headedness | Floating, vague | Stress | Depression, anxiety, panic, medications, subtle vertigo/syncope |
Important caveat: patients often cannot reliably distinguish between these, so the symptom description alone is insufficient - history, examination, and time-course are all required. - Harrison's Principles of Internal Medicine 22E
Step 2 - Evaluate for Dangerous / Central Causes First (Vertigo pathway)
If the symptom is vertigo, the first pivotal question is: Are there CNS symptoms or signs?
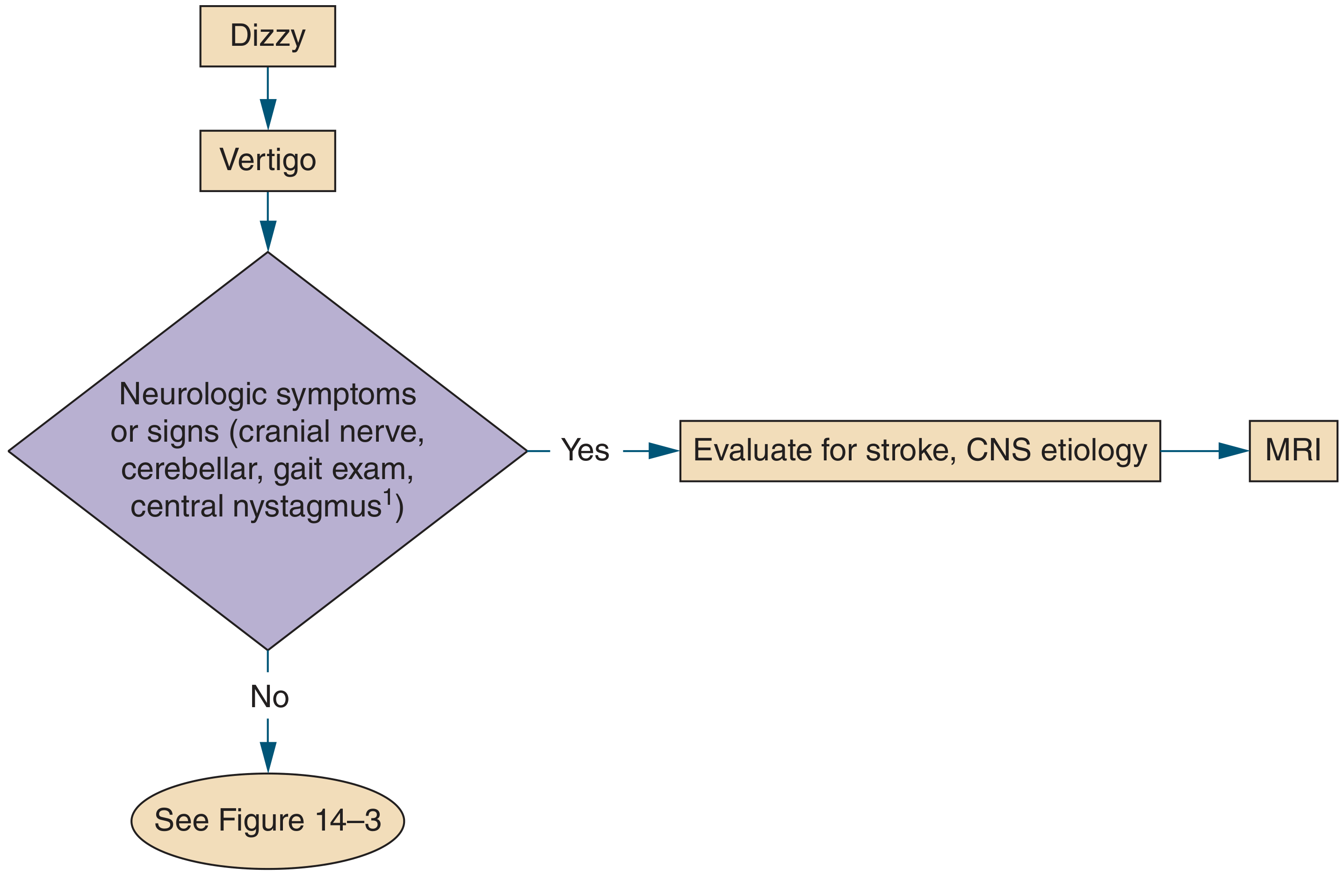
- If YES (headache, dysarthria, diplopia, ataxia, cranial nerve palsies, limb weakness/numbness) → Evaluate for stroke/CNS etiology → MRI brain
- If NO → Proceed to Step 3 (time-course and trigger analysis)
Step 3 - Time-Course and Trigger Analysis (No CNS Signs)
This narrows the peripheral vs central distinction even further:
Group 1: Brief episodes (<1 min) triggered by head movement
- Virtually always BPPV
- Evaluate with the Dix-Hallpike maneuver
- Treat with Epley repositioning maneuver
Group 2: Recurrent episodes lasting minutes to hours, spontaneous (not purely triggered)
- Differential: TIA (posterior circulation), vestibular migraine, Meniere's disease
- Clues:
- Cardiovascular risk factors → TIA
- Prior headache history → Vestibular migraine
- Tinnitus + hearing loss + aural fullness → Meniere's disease
Group 3: Continuous vertigo lasting days, worsened by motion (Acute Vestibular Syndrome)
- Differential: Vestibular neuritis vs posterior circulation stroke
- This group requires the most careful evaluation because small brainstem strokes can mimic peripheral disease
Step 4 - Examination Focused on Vertigo
Ocular Motility
- Smooth pursuit and saccades - dysmetric saccades suggest cerebellar pathology
- Assess for spontaneous nystagmus
Nystagmus: Peripheral vs Central
| Feature | Peripheral | Central |
|---|---|---|
| Direction | Unidirectional, fast phase away from lesion | May change direction with gaze |
| Suppression by fixation | Yes | No |
| Duration | < 1 min, fatigues | > 1 min, does not fatigue |
| Type | Horizonto-rotatory | Pure vertical or pure torsional = central sign |
| Associated findings | Unilateral hearing loss | Diplopia, dysarthria, limb ataxia |
Head Impulse Test (HIT / HINTS)
- Rapidly rotate the head ~20 degrees; patient fixates on a target
- Catch-up saccade present (after rotation toward affected side) = peripheral vestibular lesion (VOR deficient)
- Normal HIT in a patient with acute prolonged vertigo = suggests central cause (stroke until proven otherwise)
- HINTS exam (Head Impulse, Nystagmus, Test of Skew) - if any one component is "central," imaging is warranted
Romberg Test, Gait, Finger-Nose Test
- Severe imbalance unable to walk = more likely central
- Wide-based gait = cerebellar disease
- Shuffling gait = parkinsonism
Step 5 - Investigations
| Clinical Scenario | Investigation |
|---|---|
| Suspected central/stroke | MRI brain (preferred over CT for posterior fossa) |
| Acute peripheral vertigo (typical) | No neuroimaging needed if HINTS is reassuring |
| Meniere's suspected | Audiogram, gadolinium-enhanced MRI inner ear |
| Near syncope | ECG, orthostatic BP, Holter monitor, echocardiogram |
| Dysequilibrium | CBC, B12, HbA1c, nerve conduction studies |
| Medication-induced | Review drug list (aminoglycosides, loop diuretics, anticonvulsants) |
Key Peripheral Causes in Brief
| Condition | Key Features | Treatment |
|---|---|---|
| BPPV | Brief positional, Dix-Hallpike positive, torsional-upbeat nystagmus | Epley maneuver |
| Vestibular neuritis | Sudden, continuous, days; follows URI; no hearing loss | Supportive; short vestibular suppressants; vestibular rehab |
| Meniere's disease | Episodic vertigo hours + unilateral SNHL + tinnitus + aural fullness | Low-salt diet, diuretics, betahistine; intratympanic steroids/gentamicin for refractory cases |
| Labyrinthitis | Like vestibular neuritis but with hearing loss | Antivirals if herpetic; steroids |
Central Red Flags Requiring Urgent Workup
- New severe headache ("thunderclap") with vertigo
- Diplopia, facial numbness, dysarthria, dysphagia
- Limb ataxia or hemiparesis
- Normal head impulse test in acute prolonged vertigo
- Vertical (pure upbeat or downbeat) or direction-changing nystagmus
- Inability to walk at all (out of proportion to vestibular symptoms)
- Older patient with vascular risk factors - even without localizing signs
Sources: Symptom to Diagnosis (4th Ed.), Harrison's Principles of Internal Medicine 22E, Rosen's Emergency Medicine
Tb nose
Reading File
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.