Cast for schaphoid fracture
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information from the textbooks. Here is the full answer:
Cast for Scaphoid Fracture
The Scaphoid (Thumb Spica) Cast
The standard cast for scaphoid fractures is the thumb spica cast (also called the "scaphoid cast"). The key positioning is:
- Wrist: slight dorsiflexion (slight extension)
- Thumb: abduction and slight flexion - as if holding a glass between the index finger and thumb
- Extent: from just below the elbow to just proximal to the metacarpal necks; on the thumb, to just proximal to the interphalangeal joint
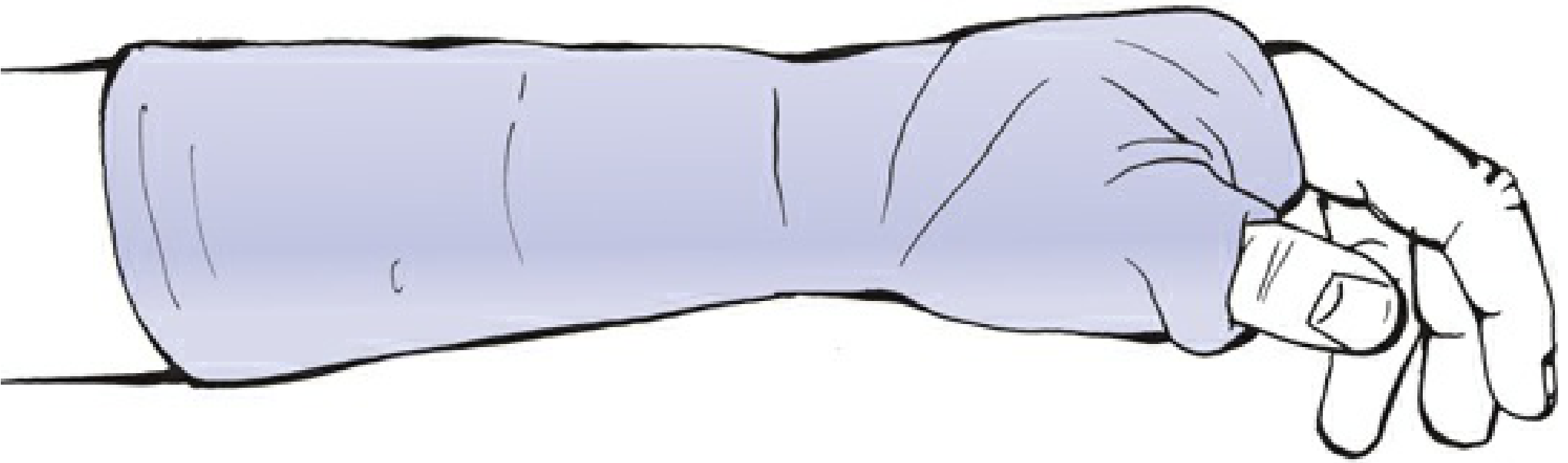
Figure: Standard scaphoid cast (Rockwood & Green's Fractures in Adults, 10th ed., p. 333)
A modification - the extended scaphoid cast - includes the entire thumb and is used for fractures distal to the MCP joint of the thumb.
Cast Type by Fracture Location
| Fracture Location | Cast Type | Duration |
|---|---|---|
| Scaphoid tubercle (distal avulsion) | Short-arm thumb spica | 4-6 weeks |
| Distal third | Short-arm thumb spica | 4-6 weeks |
| Waist (middle third) - nondisplaced | Short-arm cast ± thumb spica | 6-8 weeks (up to 10-12 weeks) |
| Proximal third | Long-arm thumb spica x 6 weeks, then short-arm thumb spica x 6+ weeks | Up to 6 months total |
Above-Elbow vs. Below-Elbow Debate
This has been extensively studied. Multiple randomized trials have shown no advantage to above-elbow (long-arm) casts over below-elbow casts for waist fractures. A biomechanics study confirmed the key motions to prevent scaphoid stress are wrist extension and ulnar deviation - both controlled by a short-arm cast. Immobilization in slight extension is preferred, as immobilization in flexion reduces wrist extension at follow-up without improving union rates.
Current evidence therefore supports short-arm (below-elbow) cast as the preferred method for nondisplaced waist fractures, rather than the classic long-arm or scaphoid cast.
Management Protocol
Suspected fracture (radiograph negative, snuffbox tender):
- Apply short-arm thumb spica cast immediately
- Re-examine + repeat X-ray at 2-3 weeks
- If still tender but no fracture visible: re-cast for 2-3 more weeks
- If still no fracture on repeat imaging and tenderness resolves: no fracture was present
Confirmed nondisplaced fracture:
- Short-arm cast for 6 weeks, then CT to assess healing
- If <50% healed on CT: extend cast another 2-4 weeks
- If >50% healed: begin active mobilization
- CT confirmation of union at ~3 months; return to forceful activity only after clear radiographic union (typically 4-6 months)
Displaced fracture (gap >2 mm, scapholunate angle >60°, radiolunate angle >15°): Refer for surgical fixation (percutaneous screw).
Key Clinical Points
- Always immobilize when snuffbox tenderness is present, even with negative initial X-rays - scaphoid fractures are notoriously occult on early plain films
- Nondisplaced fractures achieve >90% union with cast alone
- Proximal pole and displaced fractures carry higher risk of avascular necrosis and nonunion - these often need operative management or orthopedic consultation
- Complications to counsel the patient about: AVN, delayed union, nonunion, and wrist arthritis
Sources: Rockwood & Green's Fractures in Adults, 10th ed. (2025), pp. 333, 1895-1900; Pfenninger & Fowler's Procedures for Primary Care, 3rd ed., p. 1322; Textbook of Family Medicine, 9th ed.
Anatomy of schaphoid bone
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
I now have all the information needed for a comprehensive anatomy answer. Here it is:
Anatomy of the Scaphoid Bone
Overview
The scaphoid (from Greek skaphe = boat) is also called the navicular bone of the wrist. It is the largest bone of the proximal carpal row, located on the radial aspect of the wrist. It is a small, irregular, S-shaped tubular bone lying entirely within the wrist joint, oriented at a 45-degree angle to both the longitudinal and horizontal axes of the wrist.
Its long axis runs distally, laterally, and volarly - so it bridges the proximal and distal carpal rows simultaneously, which makes it unique.
Parts of the Scaphoid
The scaphoid is divided into three regions:
| Region | Features |
|---|---|
| Proximal pole | Convex articular surface; articulates with the radius |
| Waist | Narrowest part; most common fracture site (~70% of fractures here) |
| Distal pole (tubercle) | Palpable volar prominence; has two facets for trapezium and trapezoid |
The scaphoid tubercle is a palpable prominence on the volar (palmar) surface where the transverse carpal ligament (flexor retinaculum) attaches. It is a key surgical landmark and the site of entry for the volar blood supply.
The dorsal ridge (nonarticular dorsoradial surface) runs across the bone and carries the critical dorsal vessels and ligament attachments.
Articulations
The scaphoid articulates with 5 bones - more than any other carpal bone:
| Surface | Articulates With |
|---|---|
| Proximal/lateral | Radius (radial fossa) |
| Distal (2 facets) | Trapezium and Trapezoid - forms the STT (scaphotrapezio-trapezoid) joint |
| Medial (ulnar side) | Lunate and Capitate (head of capitate fits into a sulcus on the scaphoid's ulnar surface) |
Over 80% of the scaphoid's surface is covered with articular cartilage, leaving very little periosteal surface for bone healing - this is a major reason for the high rate of nonunion.
Blood Supply
The blood supply is precarious and largely retrograde - entering distally and flowing proximally - supplied by two pedicles from the radial artery:
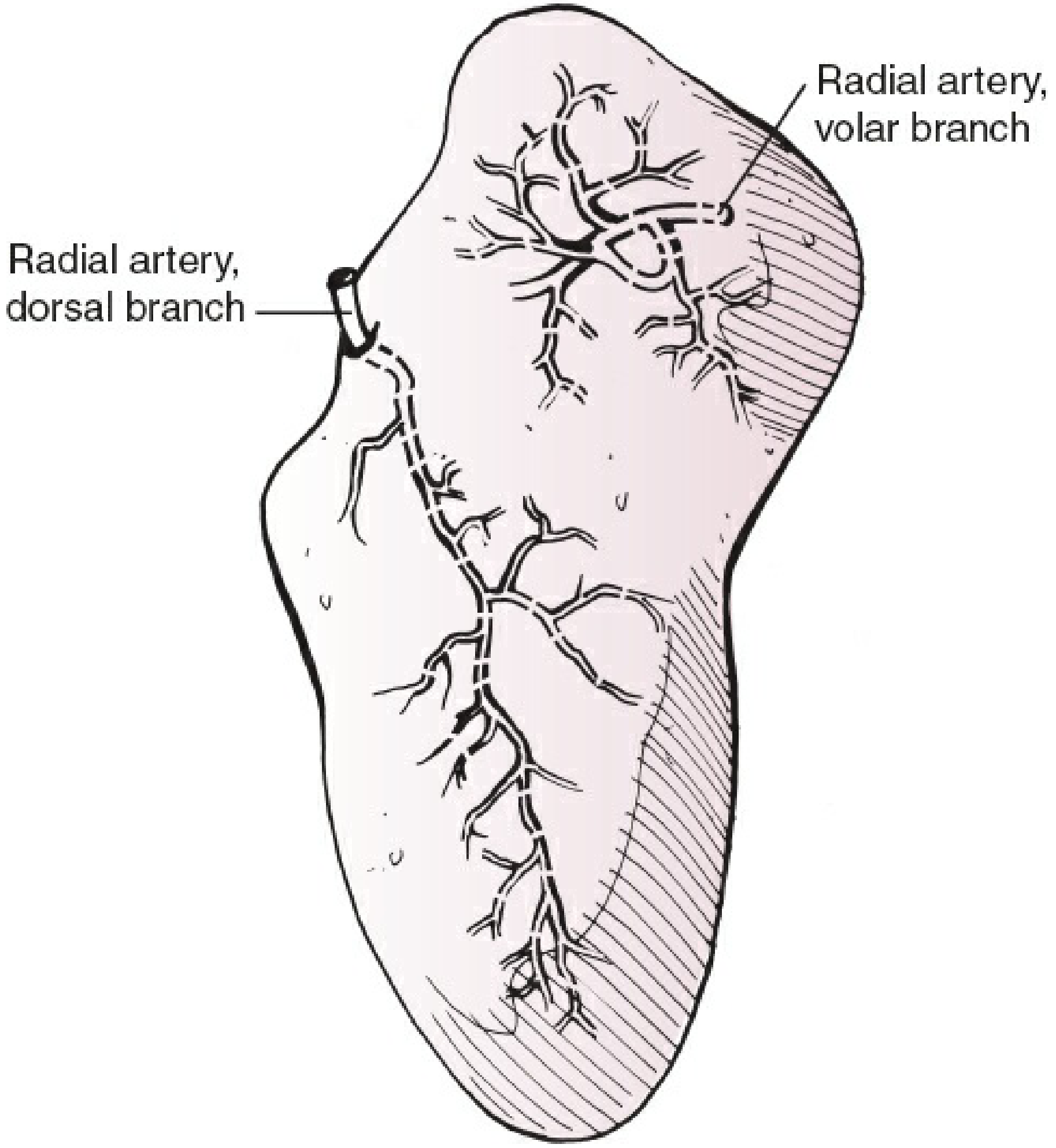
Figure 44-17: The two vascular pedicles of the scaphoid (Rockwood & Green's, 10th ed.)
1. Dorsal branch of the radial artery (dominant supply)
- Enters via small foramina along the dorsal ridge just distal to the waist
- Flows retrograde (distally to proximally)
- Supplies 70-80% of the scaphoid, including the entire proximal pole
- This is the main reason why proximal fractures risk AVN
2. Volar (palmar) branch of the radial artery
- Enters via the scaphoid tubercle
- Supplies the remaining 20-30% - the distal portion only
Clinical consequence of this pattern:
- Only 67% of scaphoids have arterial foramina throughout all three regions
- 20% have foramina mainly at the waist with virtually none in the proximal third
- Proximal third fractures may have no residual blood supply to the proximal fragment
- Risk of avascular necrosis (AVN) of the proximal pole: up to 35% for proximal pole fractures
- Waist: the waist itself has minimal or no perforating vasculature - fractures here disrupt the retrograde flow
Ligamentous Attachments
The scaphoid has no tendon attachments. Its ligamentous attachments are mostly on the nonarticular dorsoradial surface:
- Scapholunate interosseous ligament (SLIL): connects scaphoid to lunate; key stabilizer; rupture causes scapholunate dissociation
- Radioscaphocapitate (RSC) ligament: does NOT attach to the bone itself - it crosses the waist, acting as a volar sling or fulcrum around which the scaphoid rotates
- Short intrinsic ligaments: connect to adjacent carpal bones, especially the lunate
- Dorsal intercarpal ligament: attaches on the dorsal ridge
The RSC ligament's sling-like relationship to the waist is important - it is why hyperextension of the wrist generates a bending moment at the waist, causing the classic waist fracture.
Biomechanical Role
The scaphoid acts as a "bridge" or intercalated segment linking and synchronizing motion between the proximal and distal carpal rows:
- It rotates proximally and glides distally with wrist motion
- It participates in nearly all carpal movements, especially volar flexion
- Because it connects to so many bones (5 articulations), any disruption - fracture, nonunion, or ligament tear - causes progressive carpal collapse and wrist arthritis (SNAC wrist: Scaphoid Nonunion Advanced Collapse)
Why the Scaphoid Fractures So Easily
The combination of:
- Bridging position spanning both carpal rows
- 45-degree oblique orientation
- Large proportion of articular surface
- Retrograde blood supply
...makes the scaphoid the most commonly fractured carpal bone (~60-70% of all carpal fractures), typically from a fall on an outstretched hand (FOOSH) with wrist hyperextension, where the RSC sling concentrates tensile forces at the waist.
Sources: Rockwood & Green's Fractures in Adults, 10th ed. (2025), pp. 1882-1884; Campbell's Operative Orthopaedics, 15th ed. (2026), p. 4192; Imaging Anatomy: Bones, Joints, Vessels & Nerves, pp. 550-551; Miller's Review of Orthopaedics, 9th ed., p. 733
This is a shared conversation. Sign in to Orris to start your own chat.