notes on corticospinal tract (I recommend you to use your source as guyton and hall textbook of physiology , Ganong's review of medical physiology, GK Pal and Senbulingam)
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
I now have excellent content from Guyton & Hall and Ganong, plus detailed neuroanatomy from clinical textbooks. Let me compile the comprehensive notes.
Corticospinal Tract - Comprehensive Notes
Sources: Guyton & Hall Textbook of Medical Physiology; Ganong's Review of Medical Physiology, 26th Ed; Neuroanatomy through Clinical Cases, 3rd Ed; Localization in Clinical Neurology, 8th Ed
Note on GK Pal & Sembulingam: These textbooks are not in the available digital library. The notes below integrate Guyton & Hall and Ganong as your primary requested sources, supplemented by high-quality neuroanatomy references. The content closely corresponds to what GK Pal and Sembulingam cover on this topic.
1. Introduction / Definition
The corticospinal tract (CST), also called the pyramidal tract, is the principal descending motor pathway carrying voluntary motor commands from the cerebral cortex to the spinal cord. It is the most important output pathway from the motor cortex and the primary route for initiating skilled voluntary movement.
- Guyton & Hall: "The most important output pathway from the motor cortex is the corticospinal tract, also called the pyramidal tract."
- Ganong: "The corticospinal and corticobulbar system is the primary pathway for the initiation of skilled voluntary movement."
2. Origin (Cortical Sources)
The CST does not arise solely from the primary motor cortex. Its fibers come from multiple cortical areas:
| Source | % Contribution |
|---|---|
| Primary motor cortex (M1 - Brodmann's area 4, precentral gyrus) | ~30-31% |
| Premotor cortex + Supplementary motor area (area 6) | ~29-30% |
| Parietal lobe / somatosensory cortex (areas 3,1,2,5,7 - postcentral gyrus) | ~40% |
- Guyton & Hall: "The corticospinal tract originates about 30% from the primary motor cortex, 30% from the premotor and supplementary motor areas, and 40% from the somatosensory areas posterior to the central sulcus."
- Ganong: "About 31% of the corticospinal tract neurons are from M1. The premotor cortex and supplementary motor cortex account for 29% of the corticospinal tract neurons. The other 40% of corticospinal tract neurons originate in the parietal lobe."
Cell of origin: Pyramidal neurons in cortical layer V. About 3% are giant Betz cells (60 µm diameter), found exclusively in the primary motor cortex.
3. Fiber Composition
- Total fibers: over 1 million fibers per tract
- Large myelinated fibers (Betz cell fibers): ~34,000 per tract; mean diameter ~16 µm; conduction velocity ~70 m/sec (fastest signals from brain to cord)
- Small fibers (<4 µm): ~97% of total; conduct tonic background signals
- Guyton & Hall: "The most impressive fibers in the pyramidal tract are a population of large myelinated fibers with a mean diameter of about 16 micrometers... There are about 34,000 of these large Betz cell fibers in each corticospinal tract."
4. Course (From Cortex to Spinal Cord)
The tract follows a well-defined path through the neuraxis:
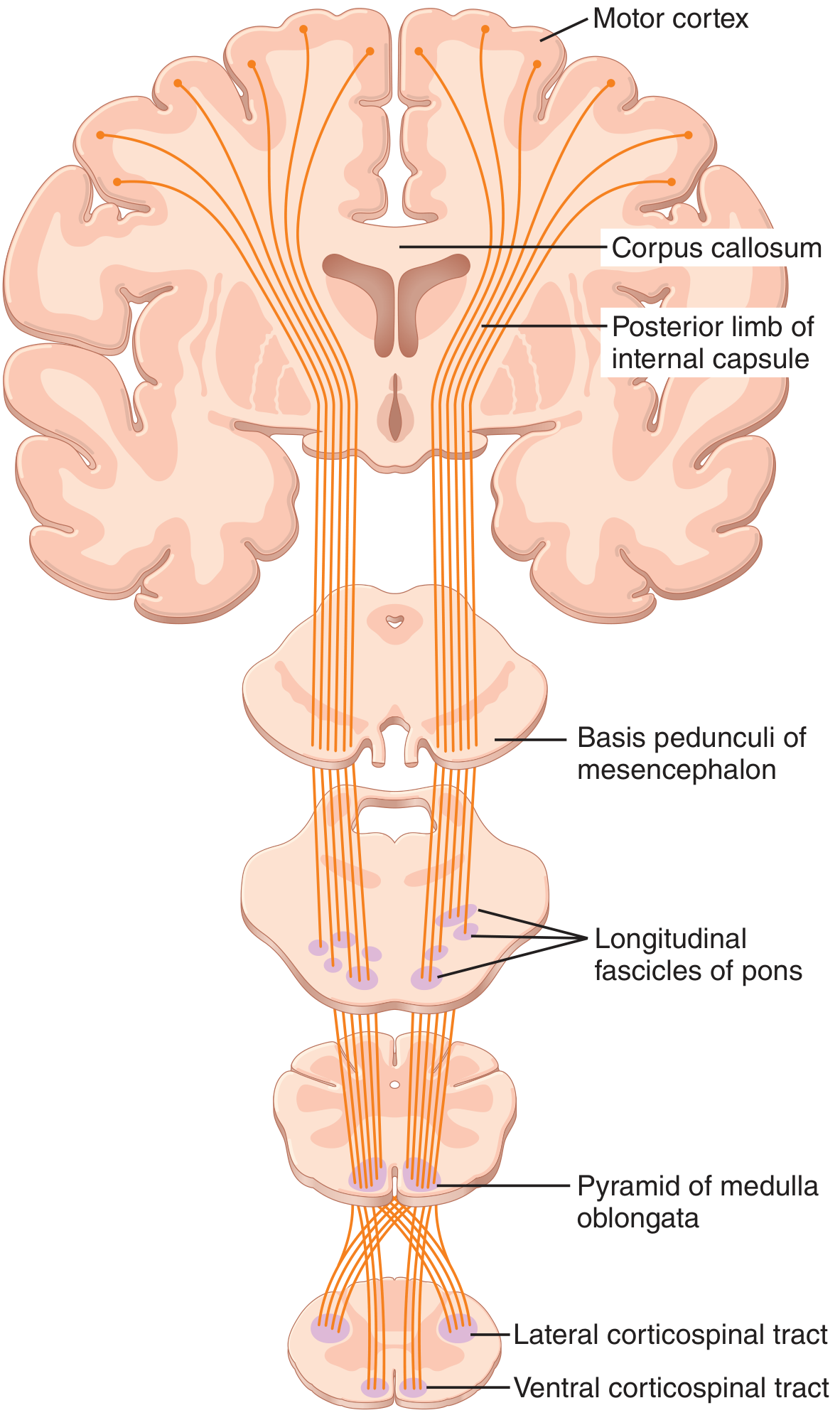
Step-by-step course:
1. Corona Radiata
Axons from the cortex enter the white matter as the corona radiata, a fanlike radiation descending toward the internal capsule.
2. Internal Capsule
Fibers condense and pass through the posterior limb of the internal capsule (between the caudate nucleus and putamen of the basal ganglia).
- Corticobulbar fibers travel in the genu of the internal capsule.
- Somatotopic arrangement in internal capsule: face fibers most anteriorly, followed by upper limb, then trunk, then lower limb fibers posteriorly.
3. Midbrain - Cerebral Peduncle (Crus Cerebri)
Fibers travel in the middle three-fifths of the crus cerebri / basis pedunculi of the midbrain.
4. Pons - Longitudinal Fascicles
In the pons, corticospinal fibers are scattered into small bundles (longitudinal fascicles) by the transverse pontocerebellar fibers.
5. Medulla - Pyramids
The fibers reunite at the level of the medulla to form the medullary pyramids on the ventral surface, giving the tract its alternative name "pyramidal tract."
6. Pyramidal Decussation (Motor Decussation)
At the junction of medulla and spinal cord (lower end of medulla):
- ~75-90% (Guyton: most; Ganong: ~80%; Neuroanatomy: ~85%) of fibers cross the midline - this is the pyramidal decussation (also called decussation of the pyramids or Mistichelli crossing)
- These crossed fibers form the lateral corticospinal tract in the contralateral spinal cord
- ~10-25% (Ganong: ~20%) of fibers remain uncrossed and descend as the anterior (ventral) corticospinal tract
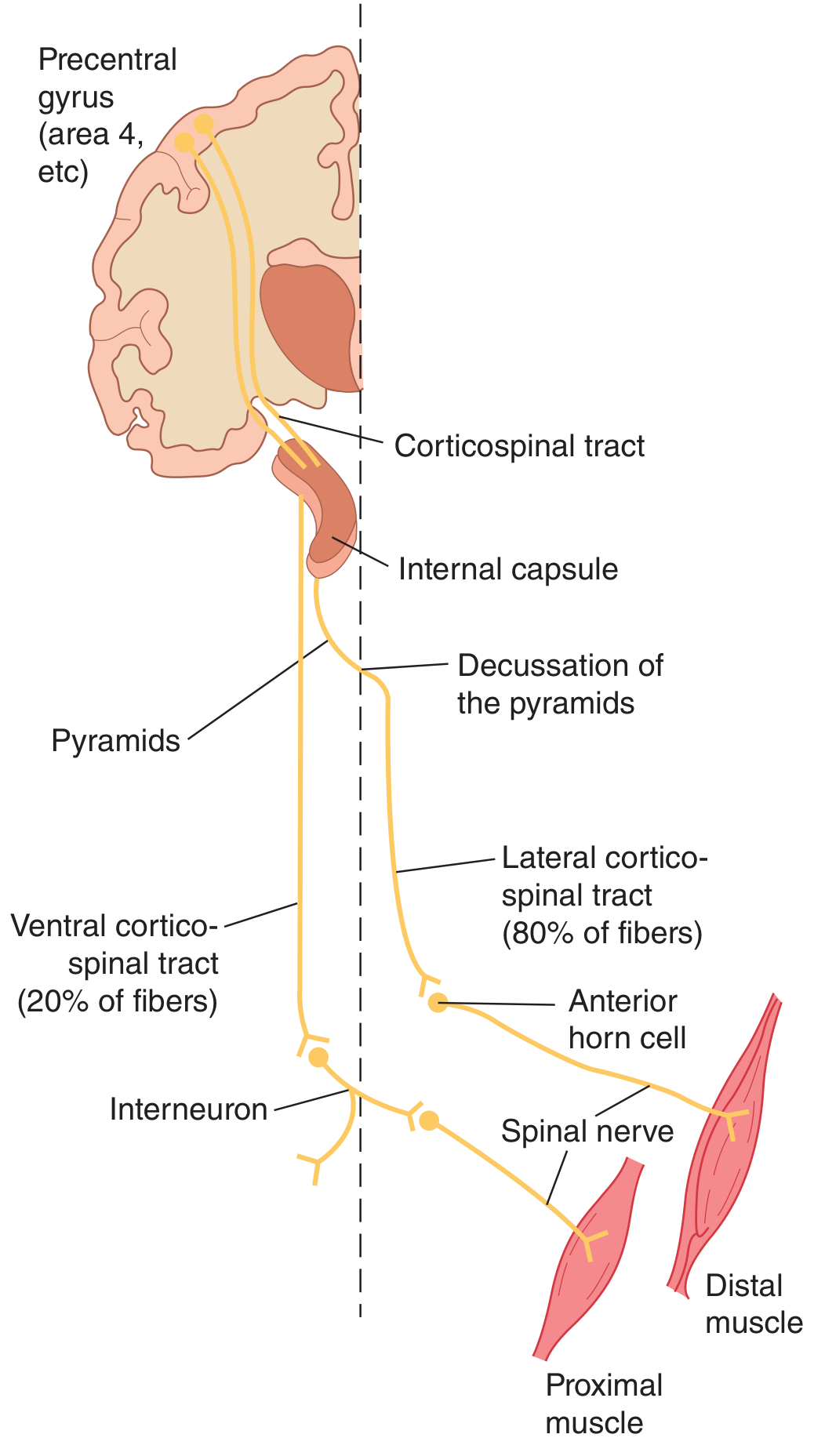
5. The Two Divisions in the Spinal Cord
A. Lateral Corticospinal Tract
- Formed by crossed fibers (~80-85%)
- Descends in the lateral funiculus (lateral white column) of the spinal cord
- Runs throughout the entire length of the spinal cord
- Terminates principally on interneurons in the intermediate gray zone, with some direct monosynaptic connections to anterior horn motor neurons (especially for skilled distal limb movements)
- Controls contralateral voluntary movement, especially fine, skilled movements of distal limbs (hands and fingers)
B. Anterior (Ventral) Corticospinal Tract
- Formed by uncrossed fibers (~15-20%)
- Descends in the anterior (ventral) funiculus of the spinal cord
- Most fibers eventually cross in the anterior white commissure at cervical or upper thoracic spinal levels before terminating
- Terminates on spinal interneurons and medial motor neuron groups
- Concerned with bilateral postural movements of the trunk and proximal muscles (supplementary motor cortex function)
- Ganong: "The ventral corticospinal tract and medial descending brainstem pathways are concerned with adjustments of proximal muscles and posture."
6. Termination in the Spinal Cord
- Mainly synapse on interneurons in the intermediate gray matter (Rexed laminae V-VIII)
- Some fibers synapse on sensory relay neurons in the dorsal horn (modulate sensory input)
- A very few fibers synapse directly on anterior horn motor neurons (alpha motor neurons) - particularly important for fine skilled movements of digits
- Guyton: "Finally terminating principally on the interneurons in the intermediate regions of the cord gray matter. A few terminate on sensory relay neurons in the dorsal horn, and a very few terminate directly on the anterior motor neurons."
7. Somatotopic Organization
The CST maintains somatotopic organization throughout its course:
- The homunculus representation on the motor cortex is preserved
- In the internal capsule: face > arm > trunk > leg (anterior to posterior)
- In the spinal cord lateral corticospinal tract: cervical segments (serving arms) are most medial; sacral segments (serving legs) are most lateral
8. Function
- Skilled voluntary movement - the primary function; especially fine, fractionated movements of the distal limbs (fingers)
- Speed and agility of movement - Betz cells provide the fastest conduction velocity to the cord
- Direct muscle activation - monosynaptic connections allow precise control
- Modulation of sensory input - fibers to dorsal horn modulate ascending sensory signals during movement
- Lateral CST + rubrospinal tract: Together control distal limb muscles and skilled movements
- Ventral CST + medial brainstem tracts: Together control axial and proximal muscles and posture
9. Upper Motor Neuron (UMN) vs. Lower Motor Neuron (LMN)
Understanding this distinction is critical for clinical application of CST knowledge.
Upper Motor Neurons (UMN)
- Cortical and brainstem neurons (including CST neurons) that innervate spinal motor neurons
- Cell bodies in motor cortex, axons travel in the CST
Lower Motor Neurons (LMN)
- Spinal and cranial nerve motor neurons whose axons directly innervate skeletal muscle
- The "final common pathway"
Clinical Features of UMN (CST) Lesion:
| Feature | UMN Lesion |
|---|---|
| Weakness/Paralysis | Contralateral (above decussation), Ipsilateral (below decussation) |
| Tone | Increased (spasticity, hypertonia) |
| Reflexes | Hyperreflexia |
| Clonus | Present |
| Babinski sign | Positive (extensor plantar response) |
| Muscle wasting | Absent (or disuse atrophy only) |
| Fasciculations | Absent |
| Distribution | Hemisplegia / monoplegia (patterns) |
Clinical Features of LMN Lesion:
| Feature | LMN Lesion |
|---|---|
| Weakness | Flaccid paralysis |
| Tone | Decreased (hypotonia) |
| Reflexes | Hypo- or areflexia |
| Fasciculations | Present |
| Muscle wasting | Marked (neurogenic atrophy) |
| Babinski sign | Negative |
Ganong: "Damage to [UMN] initially causes muscles to become weak and flaccid but eventually leads to spasticity, hypertonia, hyperactive stretch reflexes, and abnormal plantar extensor reflex (positive Babinski sign)."
Why initial flaccidity with UMN lesions? - Acute destruction of CST causes "spinal shock" with loss of facilitation to LMNs, causing transient flaccidity before spasticity develops as reorganization occurs.
The Babinski Sign - dorsiflexion of the great toe with fanning of other toes when lateral sole is scratched. Normal in infants (immature CST), pathological in adults. Localizing value but physiologic significance is unclear.
10. Lesion Localization - Where Does the Deficit Appear?
| Lesion Site | Deficit |
|---|---|
| Motor cortex (one side) | Contralateral face, arm, leg weakness |
| Internal capsule (posterior limb) | Contralateral hemiplegia (face, arm, leg all affected - dense) |
| Cerebral peduncle | Contralateral hemiplegia |
| Pons | Contralateral hemiplegia + ipsilateral CN VI/VII signs |
| Medulla (above pyramidal decussation) | Contralateral hemiplegia |
| Medulla (below / at pyramidal decussation) | Ipsilateral hemiplegia |
| Spinal cord (lateral CST, one side) | Ipsilateral weakness below lesion (Brown-Sequard pattern) |
- Neuroanatomy (Clinical Cases): "Lesions of the corticospinal tract occurring above the pyramidal decussation produce contralateral weakness, whereas lesions below the pyramidal decussation produce ipsilateral weakness."
11. Corticobulbar Tract (Related Pathway)
The corticobulbar tract travels alongside the CST but terminates in brainstem cranial nerve nuclei (CN V, VII, IX, X, XI, XII) rather than the spinal cord.
- Fibers travel in the genu of the internal capsule (vs. posterior limb for corticospinal)
- Descend in the medial part of the cerebral peduncle
- Most cranial nerve nuclei receive bilateral corticobulbar input (except lower face - CN VII, and tongue - CN XII, which have predominantly contralateral supply)
- Therefore, a unilateral UMN lesion typically spares forehead muscles (bilateral supply) but causes contralateral lower facial weakness and contralateral tongue deviation
12. Quick Summary Table
| Feature | Details |
|---|---|
| Other name | Pyramidal tract |
| Origin | Layer V pyramidal cells; area 4 (31%), area 6 (29%), parietal (40%) |
| Total fibers | >1 million per side |
| Betz cells | ~34,000; 16 µm diameter; 70 m/sec conduction |
| Course | Corona radiata → Post. limb internal capsule → Crus cerebri → Pons (scattered) → Medullary pyramid → Decussation |
| Decussation | Pyramidal decussation at caudal medulla |
| Crossed (lateral CST) | 80-85% |
| Uncrossed (anterior CST) | 15-20% |
| Lateral CST location | Lateral funiculus of spinal cord |
| Anterior CST location | Anterior funiculus of spinal cord |
| Termination | Interneurons (mainly), motor neurons (some), dorsal horn (few) |
| Function | Voluntary skilled movement (distal > proximal) |
| UMN lesion | Spasticity, hyperreflexia, Babinski+, contralateral weakness |
Sources:
- Guyton and Hall Textbook of Medical Physiology, p. 689
- Ganong's Review of Medical Physiology, 26th Ed, p. 246
- Neuroanatomy through Clinical Cases, 3rd Ed, Ch. 6
- Localization in Clinical Neurology, 8th Ed
This is a shared conversation. Sign in to Orris to start your own chat.