Explain me in detail about small intestine
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I have comprehensive content from multiple authoritative medical textbooks. Now I'll compile a thorough, well-structured answer.
The Small Intestine - A Detailed Overview
The small intestine is the longest part of the gastrointestinal tract, extending from the pyloric orifice of the stomach to the ileocecal fold. It is approximately 6-7 meters long in adults, with a progressively narrowing diameter from beginning to end. It consists of three segments: the duodenum, jejunum, and ileum.
1. Gross Anatomy
Duodenum
The duodenum is the first and shortest segment - about 20-25 cm long - and is the widest part. It is C-shaped, wraps around the head of the pancreas, and is retroperitoneal except for its very beginning (which is connected to the liver by the hepatoduodenal ligament).
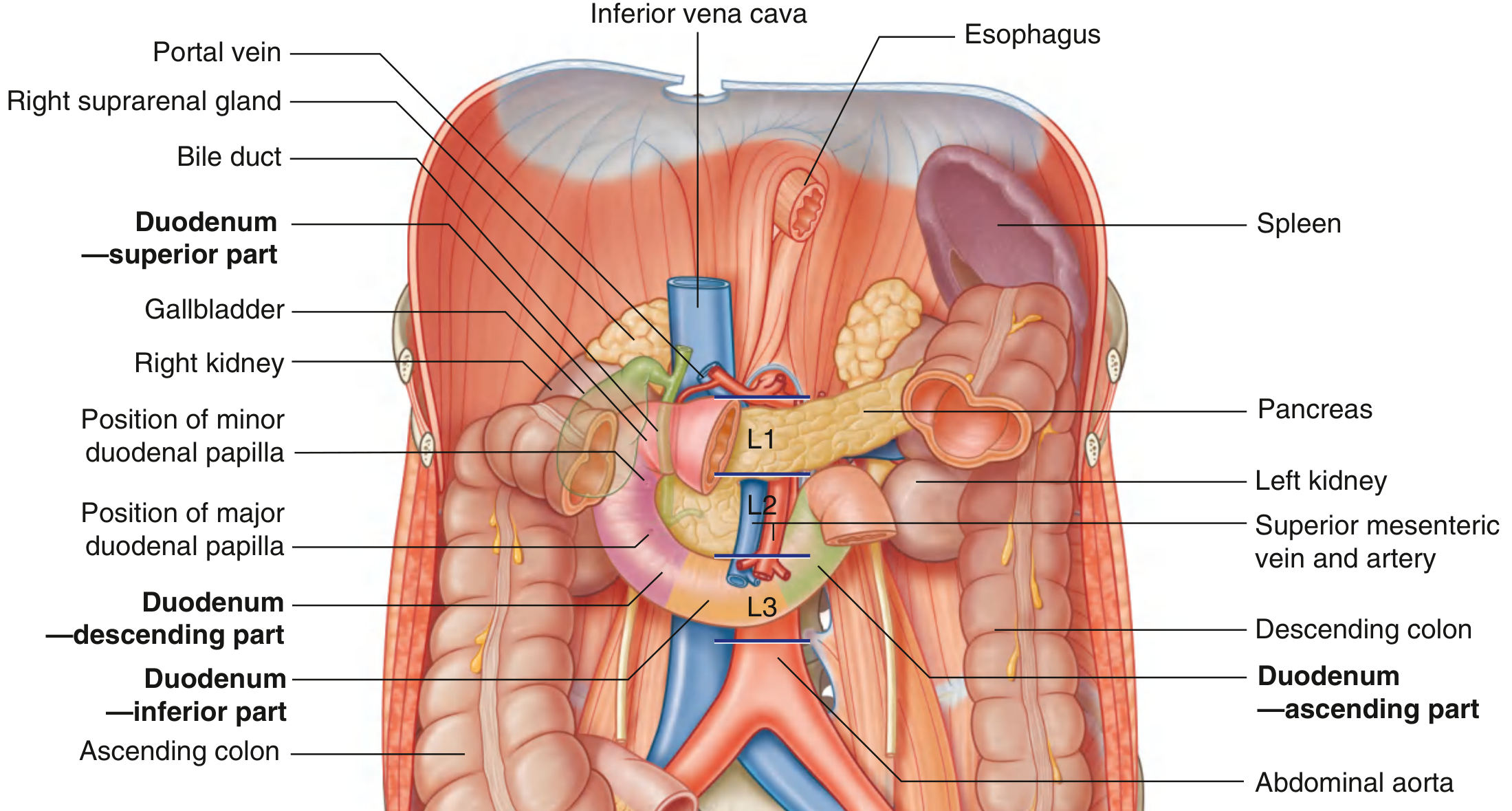
The duodenum is divided into four parts:
| Part | Location | Key Relationships |
|---|---|---|
| Superior (1st part) | Right of vertebra L1 | The "duodenal cap" - most duodenal ulcers occur here |
| Descending (2nd part) | Right of midline, L1-L3 | Contains the major duodenal papilla (bile + pancreatic duct opening) and minor duodenal papilla. Foregut/midgut junction is just below the major papilla. |
| Inferior/horizontal (3rd part) | Crosses midline | Crossed anteriorly by the superior mesenteric artery and vein |
| Ascending (4th part) | Left of aorta, ascends to L2 | Ends at the duodenojejunal flexure, held by the ligament of Treitz (suspensory muscle of duodenum) |
Blood supply to the duodenum: branches from the gastroduodenal artery (superior pancreaticoduodenal arteries) and the superior mesenteric artery (inferior pancreaticoduodenal arteries).
Jejunum
The jejunum represents the proximal two-fifths of the jejunoileal segment and lies mostly in the left upper quadrant. Key features:
- Larger diameter and thicker wall than the ileum
- Prominent plicae circulares (circular mucosal folds) - most developed here
- Less prominent arterial arcades and longer vasa recta (straight arteries) compared to the ileum
- More actively engaged in digestion and absorption
Blood supply: jejunal arteries from the superior mesenteric artery.
Ileum
The ileum makes up the distal three-fifths and lies mostly in the right lower quadrant, terminating at the ileocecal valve. Compared to the jejunum:
- Thinner walls
- Fewer and less prominent plicae circulares
- More arterial arcades and shorter vasa recta
- More mesenteric fat
The ileum opens into the large intestine at the ileocecal fold (two flaps projecting into the lumen of the cecum).
2. Histology and Microscopic Structure
The wall of the small intestine has four layers - from innermost to outermost: mucosa, submucosa, muscularis propria, and serosa.

Surface Area Amplification (Three-Fold System)
The mucosa has three structural adaptations that massively increase its absorptive surface area - estimated at over 200 m² total:
- Plicae circulares (circular/spiral folds of mucosa + submucosa): increase surface area 3-fold; most developed in the jejunum
- Villi (finger-like projections of lamina propria covered by epithelium): increase surface area a further 10-fold; each villus contains a central lacteal (lymphatic capillary), capillaries, and smooth muscle fibers
- Microvilli (the "brush border" on each enterocyte): increase surface area another 20-fold; each enterocyte carries ~3,000 microvilli; each 1 mm² of mucosa has ~200 million microvilli
Cell Types of the Intestinal Epithelium
Between the villi are the crypts of Lieberkühn (intestinal glands) - short tubular pits where stem cells reside and new cells are generated. The epithelium contains:
| Cell Type | Location | Function |
|---|---|---|
| Enterocytes | Villi (mainly) | Absorption; brush border enzymes (peptidases, disaccharidases) |
| Goblet cells | Villi and crypts | Mucus secretion for lubrication and protection |
| Paneth cells | Base of crypts | Secrete antimicrobial peptides (defensins, lysozyme) |
| Enteroendocrine cells | Crypts and villi | Secrete gut hormones (CCK, secretin, GIP, GLP-1, motilin, PYY) |
| Stem cells | Base of crypts | Pluripotent; replace all epithelial cell types ~every 3-5 days |
| Cup cells and tuft cells | Villi/crypts (especially ileum) | Functions not fully defined |
Layers of the Wall
- Mucosa: epithelium + lamina propria (connective tissue with vessels, lacteals, immune cells) + muscularis mucosae
- Submucosa: loose connective tissue with blood vessels, lymphatics, and Meissner's (submucosal) nerve plexus. The duodenum also has Brunner's glands here - they secrete alkaline mucus to neutralize gastric acid
- Muscularis propria: inner circular layer + outer longitudinal layer; between them lies Auerbach's (myenteric) plexus - the main controller of gut motility
- Serosa: visceral peritoneum; the duodenum is mostly retroperitoneal (adventitia instead of serosa)
3. Motility
Segmentation
This is the primary mixing movement of the small intestine. Localized contractions of the circular muscle divide the chyme into segments, repeatedly mixing it with digestive juices and bringing it into contact with the mucosa. It does not produce net forward movement per se but facilitates absorption.
Peristalsis
Peristaltic waves propel chyme toward the ileocecal valve. In the small intestine, peristalsis is normally weak, traveling at 0.5-2.0 cm/sec and dying out after only 3-5 cm. Net movement of chyme averages just 1 cm/min, so transit from the pylorus to the ileocecal valve takes 3-5 hours.
Peristalsis is stimulated by:
- Chyme entering the duodenum (wall stretch)
- Gastroenteric reflex (initiated by gastric distension)
- Hormones: gastrin, CCK, insulin, motilin, serotonin (pro-motility)
- Inhibited by: secretin, glucagon, GLP-1
A "peristaltic rush" occurs during intense mucosal irritation (e.g., infectious diarrhea) - powerful waves sweep contents from the small intestine into the colon within minutes.
Migrating Motor Complex (MMC)
During fasting periods, a cyclical migrating complex of electrical activity sweeps from the stomach through the small intestine approximately every 90 minutes. Its role is to clear residue and bacteria from the small intestine.
Villus Contraction
The muscularis mucosae sends fibers into villi, causing them to rhythmically shorten and elongate. This churns the lacteals (enhancing lymph flow) and increases mucosal surface exposure.
4. Digestion and Absorption
The small intestine absorbs approximately 6.5 L/day of the ~8.5 L fluid load presented to it daily. This is where the final absorption of virtually all nutrients occurs.
Carbohydrates
- Pancreatic amylase breaks down starch to oligosaccharides in the lumen
- Brush border enzymes (maltase, sucrase, lactase) complete hydrolysis to monosaccharides (glucose, galactose, fructose)
- Glucose and galactose are absorbed by Na+-dependent cotransport (SGLT1); fructose by facilitated diffusion (GLUT5)
Proteins
- Pancreatic proteases (trypsin, chymotrypsin, elastase, carboxypeptidases) reduce proteins to small peptides
- Brush border peptidases complete hydrolysis to amino acids and dipeptides
- Amino acids are absorbed by Na+-dependent cotransporters
- The jejunum is the principal site for protein digestion and absorption
Lipids
Lipid digestion in the small intestine proceeds in three steps:
- Emulsification: bile salts emulsify fat globules, creating a large surface area
- Enzymatic hydrolysis: pancreatic lipase (aided by colipase), cholesterol ester hydrolase, and phospholipase A2 break down triglycerides, cholesterol esters, and phospholipids respectively
- Micellar solubilization and absorption: products (monoglycerides, fatty acids, cholesterol) form mixed micelles with bile salts, which diffuse to the brush border, where lipids enter enterocytes by passive diffusion
- Inside enterocytes, lipids are re-esterified and packaged into chylomicrons, which enter the lacteals and travel via the lymphatic system (thoracic duct) to the bloodstream
The small intestine is the main site of synthesis of HDL, LDL, and VLDL.
Site-Specific Absorption Summary
| Segment | Primary Absorptive Roles |
|---|---|
| Duodenum | Iron, calcium, folate, fat-soluble vitamins (proximal), most minerals |
| Jejunum | Glucose, amino acids, fatty acids, most vitamins, water, electrolytes (Na+, K+, Cl-), folate |
| Ileum (general) | Continuation of jejunal functions; compensates for jejunal loss |
| Terminal ileum (specific) | Bile salts (active reabsorption via specific transporters), Vitamin B12 (intrinsic factor complex). The jejunum cannot compensate for loss of the terminal ileum. |
Electrolyte Transport
- Jejunum: Na+ absorption via Na+-monosaccharide cotransporters, Na+-amino acid cotransporters, and Na+-H+ exchange. Net result: absorption of NaHCO3. Tight junctions are "leaky" - allowing significant paracellular movement.
- Ileum: Na+ absorption by Na+-H+ exchange plus Cl--HCO3- exchange. Net result: absorption of NaCl.
- Crypts of Lieberkühn produce ~1,800 mL/day of near-pure extracellular fluid (pH 7.5-8.0), which is then immediately reabsorbed by the villi - this fluid vehicle facilitates absorption of luminal nutrients.
5. Endocrine and Immune Functions
Gut Hormones
The small intestine is an active endocrine organ, secreting:
| Hormone | Source | Stimulus | Effect |
|---|---|---|---|
| Secretin | S cells (duodenum) | Acidic chyme | Stimulates pancreatic bicarbonate secretion; inhibits gastric motility |
| CCK (cholecystokinin) | I cells (duodenum/jejunum) | Fats and proteins | Stimulates gallbladder contraction, pancreatic enzyme secretion |
| GIP (gastric inhibitory peptide) | K cells | Glucose and fat | Inhibits gastric acid; stimulates insulin release |
| GLP-1 and GLP-2 | L cells (ileum) | Nutrients | GLP-1: incretin effect (insulin release, appetite suppression); GLP-2: intestinal growth and repair |
| Motilin | M cells | Fasting state | Initiates migrating motor complex |
| PYY (peptide YY) | L cells (ileum) | Nutrients | Slows gastric emptying ("ileal brake") |
Immune Function (GALT)
The small intestine contains a large proportion of the body's immune tissue:
- Peyer's patches - organized lymphoid follicles in the ileal submucosa; key sites of immune surveillance
- M cells - specialized epithelial cells overlying Peyer's patches that sample luminal antigens
- Intraepithelial lymphocytes and lamina propria plasma cells (IgA-secreting)
- Secretory IgA is the dominant antibody in the intestinal lumen
6. Blood Supply, Venous and Lymphatic Drainage
- Duodenum: dual supply from gastroduodenal (celiac artery branch) and superior mesenteric artery via pancreaticoduodenal arcades
- Jejunum and ileum: entirely from the superior mesenteric artery (SMA) via jejunal and ileal branches forming arterial arcades; ileum has more arcades with shorter vasa recta than the jejunum
- Venous drainage: superior mesenteric vein → portal vein → liver (all absorbed nutrients except lipids pass through the liver first)
- Lymphatics: lacteals in each villus drain into mesenteric lymphatics → cisterna chyli → thoracic duct (carries chylomicrons/absorbed lipids)
- Nerve supply: sympathetic (T9-T11 via superior mesenteric plexus) and parasympathetic (vagus nerve); intrinsic enteric nervous system (Meissner's and Auerbach's plexuses)
7. Clinically Important Points
| Condition | Relevance |
|---|---|
| Duodenal ulcer | Most occur in the duodenal cap (1st part); associated with H. pylori and excess acid |
| Celiac disease | Immune reaction to gluten damages enterocytes and destroys villi; leads to malabsorption |
| Short bowel syndrome | Resection of large segments (especially terminal ileum) causes malabsorption of bile salts, vitamin B12, fat-soluble vitamins, and severe diarrhea |
| Carcinoid/NETs | Most common in the last 2 feet of the terminal ileum; 35% associated with metastases at diagnosis; average size at diagnosis ~3.5 cm |
| Crohn's disease | The only inflammatory bowel disease affecting the small intestine; terminal ileum most commonly involved |
| Bacterial overgrowth | Impaired peristalsis leads to excess bacteria in the small intestine |
Sources:
- Gray's Anatomy for Students - Anatomy of the small intestine
- Guyton and Hall Textbook of Medical Physiology - Motility, secretion, digestion
- Costanzo Physiology, 7th Edition - Electrolyte transport and absorption
- Bailey and Love's Short Practice of Surgery, 28th Edition - Physiology and clinical relevance
- Junqueira's Basic Histology, 17th Edition - Histology and cell types
- Sabiston Textbook of Surgery - Neuroendocrine tumors
This is a shared conversation. Sign in to Orris to start your own chat.