Anatomy of ij catheterization for hemodialysis
Reading File
Finding Sources
Finding Sources
Searching the Web
internal jugular vein anatomy hemodialysis catheter placement landmarks
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive information. Let me compile the full answer.
Anatomy of Internal Jugular (IJ) Catheterization for Hemodialysis
Why the IJ Vein is Preferred
The right internal jugular (IJ) vein is the first-choice site for hemodialysis catheter placement, favored by KDOQI and KDIGO guidelines. The right IJ provides a nearly straight path from the neck into the superior vena cava (SVC) and then to the right atrium, minimizing catheter tip malposition and dysfunction. The left IJ is a secondary option - it requires a longer catheter (the tip must cross the midline), and outcomes (dysfunction, infection) are generally inferior when tip depth is inadequate.
The preference hierarchy is: Right IJ > Femoral veins > Left IJ > Subclavian (last resort).
Subclavian access is actively avoided in dialysis patients because subclavian cannulation causes central vein stenosis at a higher rate than IJ catheters, which can permanently destroy the ipsilateral arm's options for future AV fistula/graft creation.
- Brenner and Rector's The Kidney, p. 2820
- Comprehensive Clinical Nephrology, 7th Ed., p. 1027
Relevant Anatomy
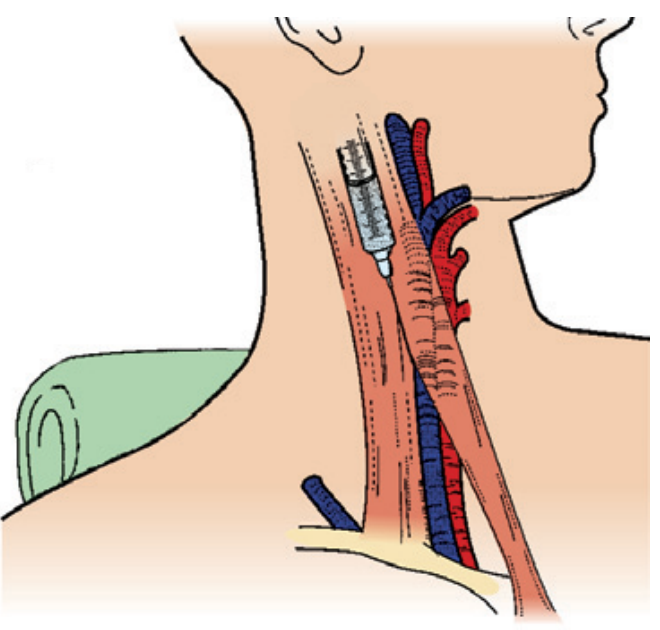
Figure: Needle approach to the IJ vein - note the IJ vein (blue) running lateral to the carotid artery (red), within the groove formed by the sternal and clavicular heads of the SCM muscle.
Key anatomical relationships:
- The IJ vein emerges at the apex of the triangle formed by the two heads (sternal and clavicular) of the sternocleidomastoid (SCM) muscle as they diverge inferiorly
- The IJ runs along the anterior border of the clavicular head of the SCM, just lateral to the common carotid artery
- The IJ, carotid artery, and vagus nerve are all enclosed in the carotid sheath
- At its lower end, the IJ joins the subclavian vein behind the sternoclavicular joint to form the brachiocephalic (innominate) vein
- The brachiocephalic veins converge to form the SVC, which drains into the right atrium
- The right IJ follows an almost straight, vertical course into the SVC - this is why it is anatomically preferred over the left
Structures at risk during IJ cannulation:
| Structure | Location | Risk |
|---|---|---|
| Common carotid artery | Medial to IJ | Arterial puncture (most common complication) |
| Vagus nerve | Posterior in carotid sheath | Rare nerve injury |
| Recurrent laryngeal nerve | Deep/medial | Hoarseness |
| Phrenic nerve | Anterior to anterior scalene | Paralysis of ipsilateral hemidiaphragm |
| Brachial plexus | Posterior triangle | Neurological deficit |
| Thoracic duct (left only) | At left IJ-subclavian junction | Chylothorax |
| Apex of pleura | At base of neck | Pneumothorax (less common than subclavian) |
- Pfenninger and Fowler's Procedures for Primary Care, 3rd Ed.
Procedural Anatomy (Central Approach)
Patient positioning: Trendelenburg (15-30 degrees head-down) to distend the IJ vein, reduce air embolism risk, and bring the vein closer to the surface. Head is turned slightly to the contralateral side.
Insertion site: Just at, or slightly caudal to, the apex of the SCM triangle - the V-shaped groove formed between the sternal and clavicular heads of the SCM muscle. This is typically at or just above the level of the thyroid cartilage.
Needle angle and direction:
- Insert at a 30-degree angle to the skin
- Aim toward the ipsilateral nipple (or the ipsilateral anterior superior iliac spine in larger patients)
- Return of dark, non-pulsatile blood confirms venous entry
Three classic approaches:
| Approach | Entry Point | Direction |
|---|---|---|
| Central (most common) | Apex of SCM triangle | Toward ipsilateral nipple, 30° to skin |
| Anterior | Medial to SCM (at midpoint) | Lateral, toward IJ at 45° |
| Posterior | Behind SCM (posterior border) | Anteroinferior under SCM |
The central approach is most commonly used for hemodialysis catheters because ultrasound easily targets the vein at this location.
- Pfenninger and Fowler's Procedures for Primary Care, 3rd Ed., p. 1525-1542
Catheter Course and Tip Placement

Figure: Ultrasound-guided access to the right IJ vein for tunneled hemodialysis catheter placement.
For hemodialysis catheters, the tip must sit in a large, high-flow vessel to sustain blood flow rates of 300-400 mL/min without recirculation:
- Optimal tip position: Atriocaval junction (junction of SVC and right atrium), or within the mid-to-lower right atrium
- If the tip is too high (in the SVC proper), blood flow rates are suboptimal and dysfunction is more common
Catheter path for tunneled IJ catheters:
- Vein entry at IJ (at the neck, above the clavicle)
- A subcutaneous tunnel is created running lateral and inferior, under the clavicle, approximately 5-7 cm from the initial needle entry site
- The tunnel exit (skin exit site) is typically in the infraclavicular region, roughly 1-2 cm below the clavicle, midway between the sternal and humeral heads of the clavicle
- A Dacron cuff sits in the tunnel ~2 cm from the exit site - this anchors the catheter and creates a mechanical barrier against infection
- Brenner and Rector's The Kidney, p. 2910
Catheter Length by Access Site
Using the Peres formula (from Comprehensive Clinical Nephrology, 7th Ed., p. 1027):
| Access Site | Formula | Accuracy |
|---|---|---|
| Right internal jugular | Height (cm) / 10 | 90% |
| Left internal jugular | Height (cm) / 10 + 4 cm | 94% |
| Right subclavian | Height (cm) / 10 - 2 cm | 96% |
| Left subclavian | Height (cm) / 10 + 2 cm | 97% |
Standard catheter sizes: 14.5-16 French, lengths of 24 cm (right IJ), 28 cm (left IJ), and 36-42 cm (femoral).
Ultrasound Guidance
Real-time ultrasound is strongly recommended (Grade 1A recommendation per SCCM guidelines) for IJ cannulation. Ultrasound:
- Confirms vein compressibility (differentiating it from the non-compressible carotid artery)
- Identifies anatomical variants (IJ sitting medial to carotid in ~5% of patients)
- Reduces arterial puncture and first-pass failure
- Particularly important in patients with obesity, short necks, prior neck surgery, or prior IJ catheters
Ultrasound views:
-
Short-axis (transverse): See the IJ as a round, compressible, non-pulsatile vessel lateral to the pulsatile carotid; needle appears as a bright dot
-
Long-axis: Shows the needle tip coursing into the vein in real time - reduces "posterior wall" puncture
-
Miller's Anesthesia, 10e; Fischer's Mastery of Surgery, 8e
Complications Specific to IJ Access for HD
| Complication | Notes |
|---|---|
| Arterial puncture (carotid) | Most common; managed with direct compression |
| Pneumothorax | Less common than subclavian; risk is low with IJ approach |
| IJ thrombosis | ~25% of tunneled catheters (usually asymptomatic) |
| Catheter dysfunction | Due to fibrin sheath, intraluminal clot, or tip malposition |
| Exit site / tunnel infection | Risk reduced by Dacron cuff in tunneled catheters |
| Catheter-related bacteremia | Major long-term morbidity; lower with tunneled vs. non-tunneled |
| Central vein stenosis | Less common with IJ than subclavian access |
| Air embolism | Prevented by Trendelenburg positioning during insertion |
The right IJ has a lower dysfunction rate than the left IJ, largely due to its straighter course into the SVC without requiring the catheter to traverse a more tortuous angle.
- Brenner and Rector's The Kidney; Comprehensive Clinical Nephrology, 7th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.