Hii
Hey! How can I help you today?
Teach me tof
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Here is a complete, well-organized lesson on Tetralogy of Fallot (TOF):
Tetralogy of Fallot (TOF)
What is TOF?
TOF is the most common cyanotic congenital heart disease beyond infancy. It accounts for about 5% of all congenital cardiac malformations. The name comes from the French physician Étienne-Louis Arthur Fallot, who described the four defects in 1888.
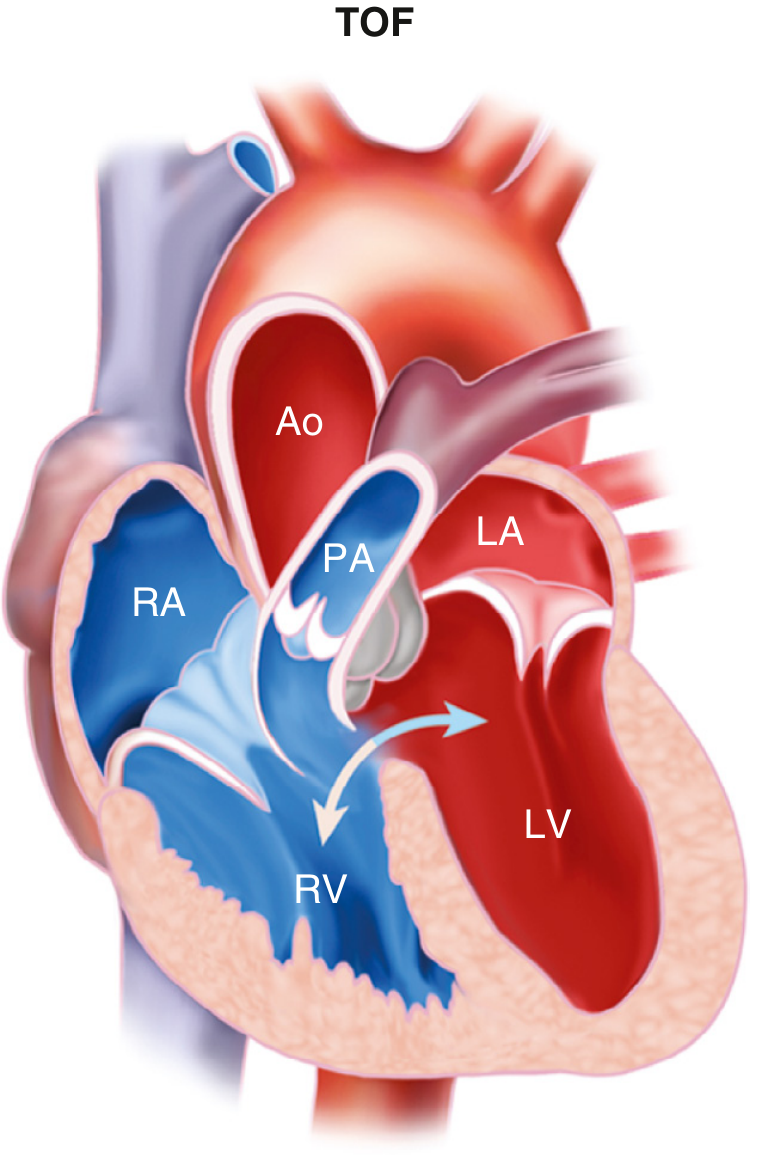
The 4 Defects (The "Tetralogy")
All four defects arise from a single embryological cause: anterosuperior displacement of the infundibular septum (the part of the ventricular wall that separates the outflow tracts).
| # | Defect | Description |
|---|---|---|
| 1 | VSD (Ventricular Septal Defect) | Large, unrestrictive hole in the interventricular septum |
| 2 | RVOTO (Right Ventricular Outflow Tract Obstruction) | Narrowing below/at/above the pulmonary valve (subpulmonic stenosis most common) |
| 3 | Overriding Aorta | The aorta straddles the VSD, receiving blood from BOTH ventricles |
| 4 | RVH (Right Ventricular Hypertrophy) | Secondary to the high pressure from the RVOTO |
Mnemonic: "PROVE" - Pulmonary stenosis, Right ventricular hypertrophy, Overriding aorta, VSD (some use "HOPS": Hypertrophy, Overriding aorta, Pulmonary stenosis, Septal defect)
Here is a diagram showing the anatomy:
Pathophysiology
The key problem is decreased pulmonary blood flow and right-to-left shunting of deoxygenated blood.
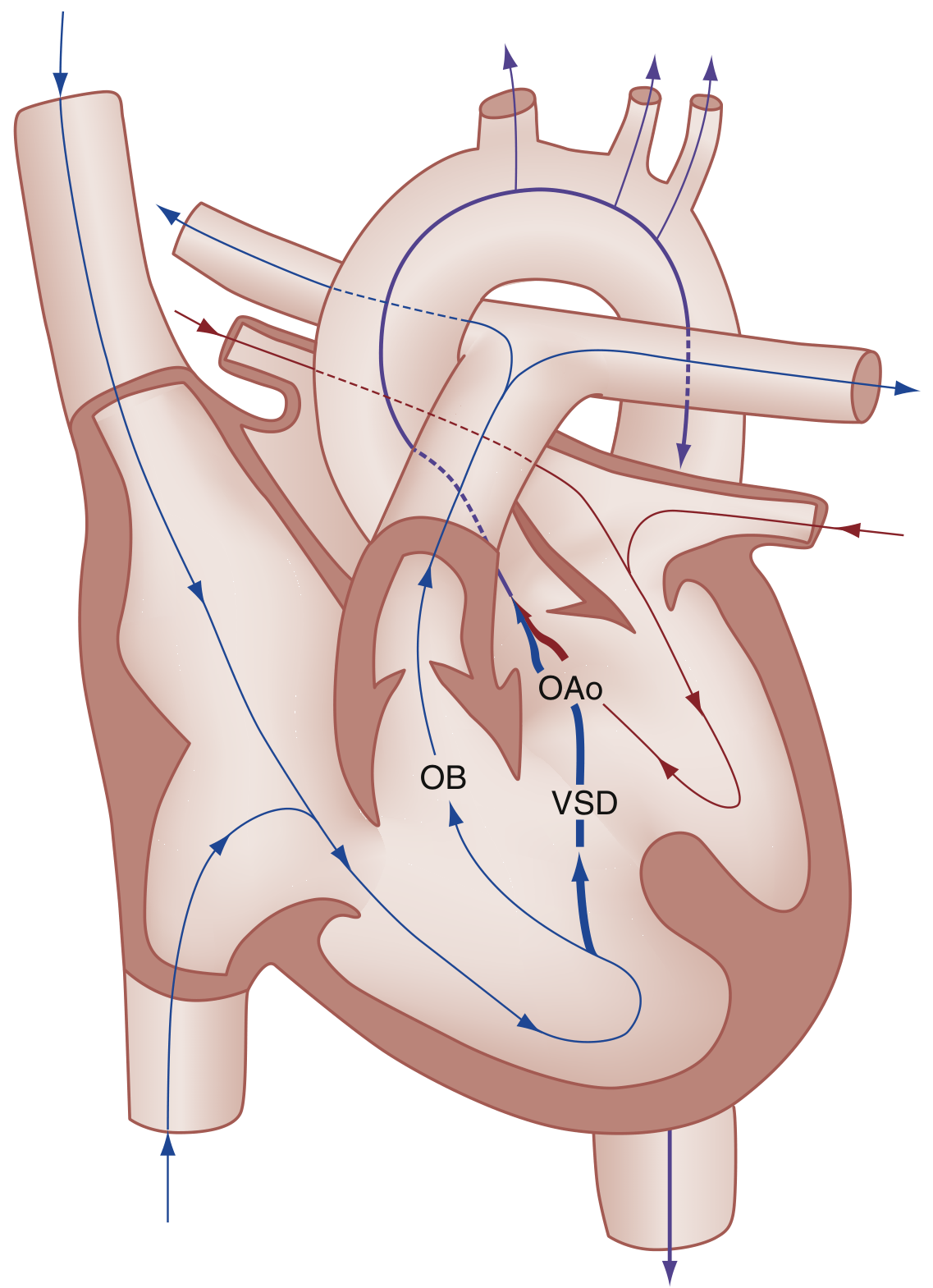
- Deoxygenated blood in the RV cannot easily get to the lungs (blocked by RVOTO)
- Blood is instead shunted right-to-left across the VSD into the left ventricle and the overriding aorta
- Up to 75% of venous blood can bypass the lungs entirely
- Result: systemic hypoxemia and cyanosis
Clinical Features
Degree of cyanosis depends on the severity of RVOTO:
- Mild RVOTO = "Pink TOF" (acyanotic) - may not present until age 1-3 years
- Severe RVOTO = Profound cyanosis within first days of life; may need PGE1 infusion to keep the PDA open
Signs and symptoms:
- Cyanosis (bluish skin, lips)
- Systolic ejection murmur at the left sternal border (from RVOTO, NOT the VSD)
- Chronic hypoxemia leads to compensatory polycythemia
- Clubbing of fingers and toes
- Squatting in older children (increases SVR, reduces R-to-L shunt)
Investigations
Chest X-ray
- "Boot-shaped heart" (coeur en sabot): due to RVH causing upward tilting of the cardiac apex + concave main pulmonary artery segment
- Decreased pulmonary vascular markings (less blood reaching lungs)
- Right-sided aortic arch in 25% of cases
ECG
- Right axis deviation
- Right ventricular hypertrophy (tall R in V1, deep S in V6)
Echocardiography (Echo)
- Confirms all four defects
- Shows overriding aorta, VSD, RVOTO severity
- CW Doppler across pulmonic valve: high velocity consistent with severe stenosis
The "Tet Spell" (Hypercyanotic/Hypoxic Spell)
This is a medical emergency that occurs most commonly in infants aged 2-4 months.
Trigger: Anything that suddenly drops systemic vascular resistance (SVR) - crying, defecation, feeding, tachycardia, hypovolemia
Vicious cycle:
Drop in SVR → More R-to-L shunting across VSD → Hypoxemia + hypercapnia + acidosis → Hyperpnea → Increased venous return to RV → More shunting... (cycle worsens)
Clinical signs: Hyperpnea, prolonged crying, worsening cyanosis, limpness. Severe spells can cause seizures, stroke, or death. Notably, the murmur decreases during a tet spell (less blood going through the RVOT).
Management of Tet Spell
| Priority | Intervention | Mechanism |
|---|---|---|
| 1st | Knee-to-chest position (infants) / Squatting (children) | Increases SVR, reduces R-to-L shunt |
| 2nd | Supplemental O2 | Limited benefit alone |
| 3rd | Morphine 0.1-0.2 mg/kg IV/IM | Calms child, reduces catecholamine surge, lowers respiratory rate |
| Alt. opioid | Fentanyl 1 µg/kg IV/IM or 1.5-2 µg/kg intranasal | No histamine release risk |
| Sedation | Midazolam 0.2-0.3 mg/kg intranasal | |
| Acidosis | Sodium bicarbonate 1 mEq/kg IV if pH <7.4 | Breaks hypoxemia-acidosis cycle |
| Refractory | Ketamine 1-2 mg/kg IV or 3-5 mg/kg IM | Analgesia + increases SVR |
| Refractory | Phenylephrine 0.01-0.02 mg/kg IV | Alpha-agonist, raises SVR |
| Refractory | Propranolol 0.1-0.2 mg/kg IV | May reduce infundibular spasm |
| Refractory | IV fluid bolus | Increases preload/pulmonary flow |
Treatment / Surgery
Palliative (temporary)
- Modified Blalock-Taussig (BT) shunt: anastomosis between the subclavian artery and ipsilateral pulmonary artery - increases pulmonary blood flow
Definitive Surgical Repair
- Close the VSD (patch)
- Relieve the RVOTO (resect infundibular tissue, possibly patch the RVOT/pulmonary valve annulus)
- Mortality: 5-10% for corrective surgery (when done early)
Long-term Issues After Repair
- The major late complication is pulmonary regurgitation (from disrupting the pulmonary valve during repair)
- Leads to progressive RV dilation and dysfunction
- May eventually require pulmonary valve replacement
- Serial echo monitoring (and cardiac MRI for RV volumes) is essential
Associated Defects
- Right-sided aortic arch (25%)
- ASD (atrial septal defect)
- Anomalous origin of the left coronary artery
- Patent ductus arteriosus (PDA)
Key High-Yield Points
| Fact | Detail |
|---|---|
| Most common cyanotic CHD beyond infancy | TOF |
| Embryologic cause | Anterosuperior displacement of infundibular septum |
| CXR appearance | Boot-shaped heart + decreased pulmonary markings |
| Murmur character | Ejection systolic murmur at left sternal border (from RVOTO) |
| Tet spell position | Knee-to-chest (infants), squatting (older children) |
| Palliative surgery | Modified Blalock-Taussig shunt |
| Long-term post-repair complication | Pulmonary regurgitation |
| Untreated prognosis | Average life expectancy only 3-4 years without surgery |
Sources: Rosen's Emergency Medicine, Robbins & Kumar Basic Pathology, Guyton & Hall Medical Physiology, Textbook of Clinical Echocardiography (Braunwald's Heart Disease)
Would you like me to go deeper into any particular aspect - such as embryology, surgical techniques, echocardiographic findings, or post-repair complications?
This is a shared conversation. Sign in to Orris to start your own chat.