testis and ovary tumour from robbin
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from Robbins Basic Pathology. Let me compile the complete, detailed answer:
Testis and Ovary Tumours - Robbins & Kumar Basic Pathology
TESTICULAR TUMOURS
(Robbins & Kumar Basic Pathology, Chapter 16 - pp. 655-658)
Classification
Testicular tumours fall into two broad categories:
| Category | Frequency | Behaviour |
|---|---|---|
| Germ cell tumours | ~95% | Almost all malignant |
| Sex cord-stromal tumours (Sertoli/Leydig cell) | Uncommon | Usually benign |
Germ cell tumours are divided into:
- Seminomas (~50% of all GCTs)
- Nonseminomatous tumours (embryonal carcinoma, yolk sac tumour, choriocarcinoma, teratoma, mixed)
Pathogenesis
- Incidence lowest in Africa and Asia; rising worldwide
- Family history: fathers and sons - 4x risk; brothers of affected males - 8-10x risk
- Cryptorchidism - associated with cancer in undescended testis AND contralateral descended testis; found in ~10% of testicular cancer cases
- Intersex syndromes (androgen insensitivity, gonadal dysgenesis) increase risk
- Chromosome 12p: extra copies (usually isochromosome i[12p]) found in virtually ALL germ cell tumours
- KIT oncogene mutations: found in up to 25% of tumours
- Most tumours in postpubertal males arise from a precursor - germ cell neoplasia in situ (GCNIS)
Individual Tumour Types
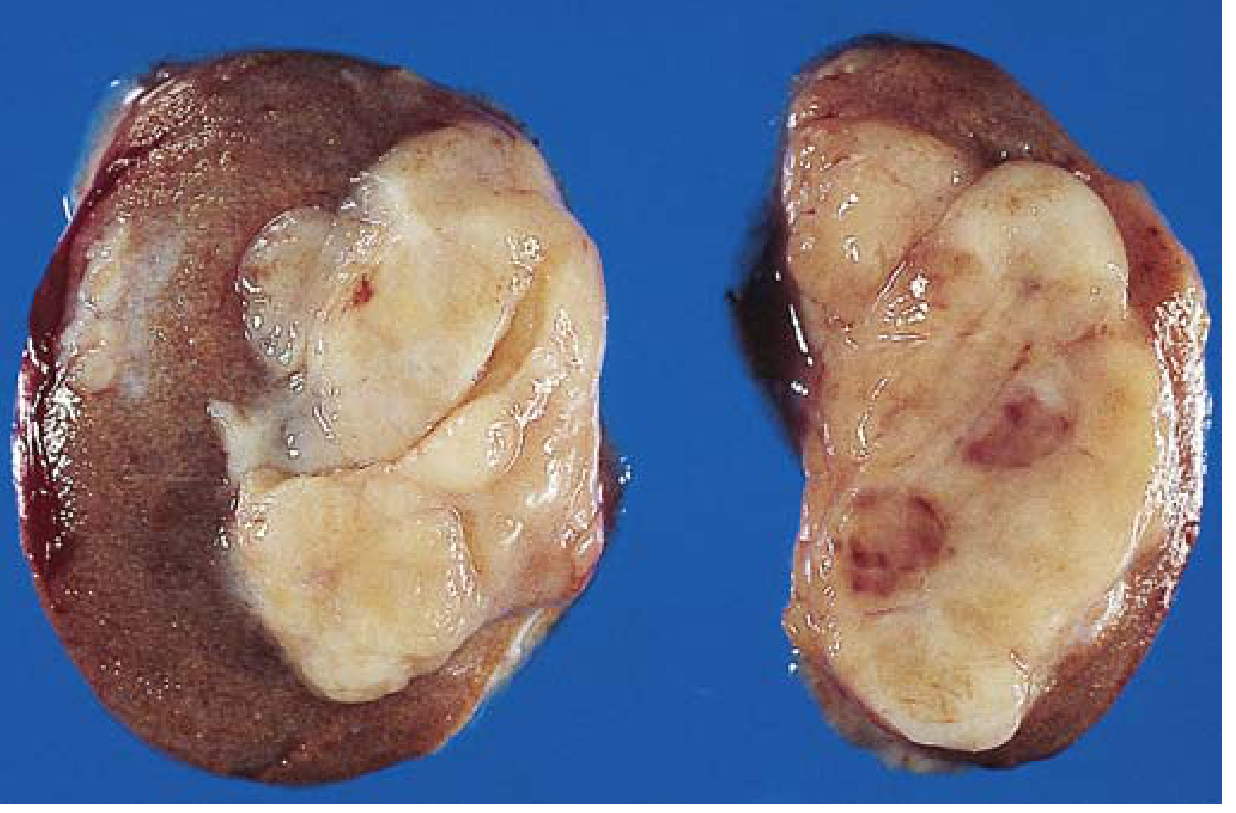
1. SEMINOMA (~50% of GCTs)
- Gross: soft, well-demarcated, gray-white homogeneous mass; foci of coagulative necrosis (no hemorrhage)
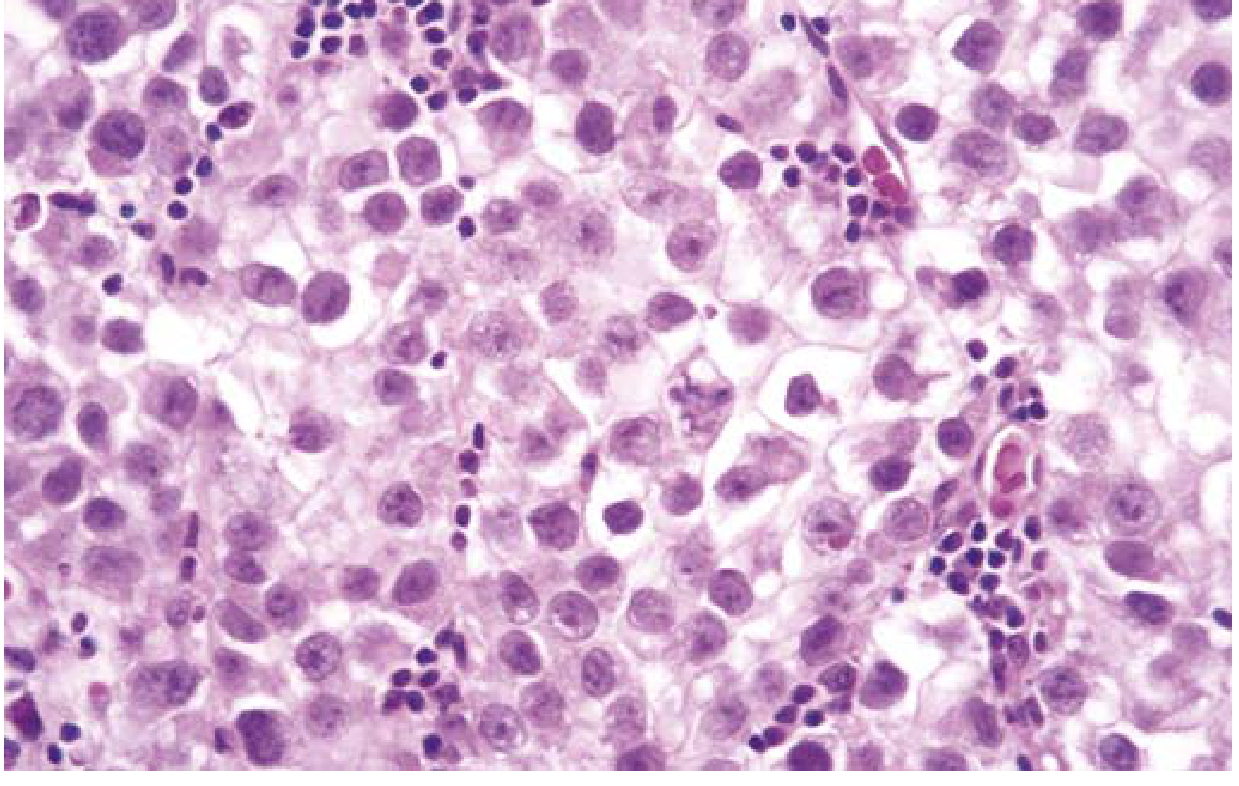
- Histo: large uniform cells with:
- Distinct cell borders
- Clear glycogen-rich cytoplasm
- Round nuclei with conspicuous nucleoli
- Small lobules with fibrous septa
- Lymphocytic infiltrate (characteristic)
- May have granulomatous reaction
- ~15% contain syncytiotrophoblasts → mildly elevated serum hCG (10-15% stage I; 30-50% disseminated)
- Histologically identical to dysgerminoma (ovary) and germinoma (CNS/extragonadal)
2. SPERMATOCYTIC TUMOUR (formerly Spermatocytic Seminoma)
- Rare (~1-2% of GCTs); affects older males (usually >65 years)
- Slow-growing; does NOT metastasize
- NOT associated with GCNIS; lacks i(12p); gains chromosome 9q
- Excellent prognosis with surgical resection
3. EMBRYONAL CARCINOMA (~2-3% pure; often mixed)
- Gross: ill-defined invasive mass with hemorrhage and necrosis; primary may be small even with systemic metastases
- Histo: large cells with basophilic cytoplasm, indistinct borders, large hyperchromatic nuclei, prominent nucleoli; solid sheets, primitive glands, or papillae

4. YOLK SAC TUMOUR (Endodermal Sinus Tumour)
- Most common testicular tumour in children < 3 years (excellent prognosis in this age group)
- In adults: rarely pure; usually mixed with embryonal carcinoma
- Histo: microcysts, lacelike/reticular patterns, glands, papillae
- Pathognomonic: Schiller-Duval bodies (primitive glomerulus-like structures)
- AFP (alpha-fetoprotein) positive (eosinophilic hyaline globules containing AFP and α1-antitrypsin)
5. CHORIOCARCINOMA
- Highly malignant; primary often small and nonpalpable despite extensive metastases
- Histo: cytotrophoblast-like cells capped by eosinophilic syncytiotrophoblasts
- Markedly elevated serum hCG
- Spreads haematogenously early (lungs, liver, brain)
6. TERATOMA
- Germ cells differentiate along multiple somatic lineages
- Gross: heterogeneous - solid, cartilaginous, cystic areas
- Histo: neural tissue, muscle, cartilage, squamous epithelium, thyroid-like tissue, bronchial epithelium, intestinal wall elements
- Prepubertal type: NOT associated with GCNIS or i(12p) → benign
- Postpubertal/adult type: considered malignant regardless of maturity of elements
- Teratoma with somatic-type malignancy: rare transformation into squamous cell carcinoma, adenocarcinoma, or sarcoma; resistant to standard GCT chemotherapy
Clinical Features of Testicular GCTs
- Presentation: painless testicular mass (nontranslucent - unlike hydrocele)
- Standard management: radical orchiectomy (biopsy avoided due to tumor spillage risk)
- Tumour markers:
- AFP: yolk sac tumour; elevated in nonseminomatous GCTs
- hCG: choriocarcinoma, seminoma (low elevation)
- LDH: correlates with tumour bulk
Staging and Prognosis:
- Seminomas: radiosensitive; excellent prognosis even with metastases
- Nonseminomatous GCTs: treated with BEP chemotherapy; cure rates >90% even with metastatic disease
- Key staging: limited to testis → retroperitoneal lymph nodes → hematogenous spread (lung, liver, brain)
OVARIAN TUMOURS
(Robbins & Kumar Basic Pathology, Chapter 17 - pp. 695-700)
Overview
Ovarian cancer is the second most common gynecologic malignancy (after endometrial carcinoma) but the leading cause of gynecologic cancer death in the US.
Three cell types give rise to ovarian tumours:
| Origin | Tumour Type | % of All Ovarian Tumours | % Malignant |
|---|---|---|---|
| Surface/fallopian tube epithelium | Epithelial tumours | ~70% | ~90% of all malignancies |
| Germ cells | Germ cell tumours | 20-30% | <10% of malignancies |
| Sex cord-stromal cells | Sex cord-stromal tumours | Uncommon | <10% of malignancies |
Frequency of Major Ovarian Tumours:
| Type | % Malignant Ovarian Tumours | % Bilateral |
|---|---|---|
| Serous - benign (60%) | 47% total | 25% |
| Serous - borderline (15%) | 30% | |
| Serous - malignant (25%) | 65% | |
| Mucinous - benign (80%) | 3% total | 5% |
| Mucinous - borderline (10%) | 10% | |
| Mucinous - malignant (10%) | <5% | |
| Endometrioid carcinoma | 20% | 20% |
| Undifferentiated carcinoma | 10% | - |
| Granulosa cell tumour | 5% | 5% |
| Teratoma - benign (96%) | 1% | 15% |
| Metastatic | 5% | >50% |
A. SURFACE EPITHELIAL TUMOURS
Most arise from müllerian epithelium. About 80% are benign and occur in women aged 20-45.
Two molecular types of carcinoma:
- Type I carcinoma: low-grade, arises from borderline tumours or endometriosis; includes low-grade serous, endometrioid, mucinous; has KRAS/BRAF/ERBB2 mutations; wild-type TP53
- Type II carcinoma: high-grade serous; arises from serous tubal intraepithelial carcinoma (STIC); TP53 mutations in >95%
Risk factors for epithelial carcinomas:
- Increasing age
- Early menarche/late menopause
- Nulliparity
- Family history
- BRCA1 or BRCA2 mutations (found in 5-10% familial cases; 20-60% lifetime risk of ovarian cancer)
- Oral contraceptive use is protective (suppresses ovulation)
1. SEROUS TUMOURS (most common)
Most common ovarian epithelial tumour; 70% benign or borderline, 30% malignant.
- Gross: large spherical/ovoid cystic structures (up to 30-40 cm); multiloculated with septa; filled with clear serous fluid; papillary projections into cystic cavities (more prominent in malignant)
- Histo benign: single layer columnar epithelium lining cysts
- Histo malignant (high-grade): complex papillary and solid architecture; psammoma bodies (laminated calcifications) characteristic
- 25% of benign tumours bilateral; 65% of malignant bilateral
2. MUCINOUS TUMOURS
- Gross: multiloculated cysts filled with gelatinous/mucinous material
- Histo: glands and cysts lined by mucin-secreting columnar cells resembling endocervical or intestinal epithelium
- Usually unilateral; less commonly malignant than serous
- Rupture → pseudomyxoma peritonei (gelatinous implants on peritoneum)
3. ENDOMETRIOID CARCINOMA
- Accounts for ~20% of ovarian carcinomas
- Resemble uterine endometrial glands histologically
- 20% bilateral; 15-30% coexist with endometrial carcinoma (synchronous primary)
- Associated with endometriosis
B. GERM CELL TUMOURS OF OVARY
1. MATURE CYSTIC TERATOMA (Dermoid Cyst)
- Most common ovarian germ cell tumour; 96% benign
- Tissues from all three germ layers: skin, hair, teeth, sebaceous material
- Bilateral in 15%
- Malignant transformation rare (<2%): most commonly squamous cell carcinoma
2. DYSGERMINOMA
- Ovarian counterpart of testicular seminoma
- Most common malignant germ cell tumour of ovary
- Occurs in young women/girls
- Radiosensitive; good prognosis
- Bilateral in ~15%
3. ENDODERMAL SINUS TUMOUR (Yolk Sac Tumour)
- Elevated AFP
- Schiller-Duval bodies
- Highly malignant; seen in young females
4. CHORIOCARCINOMA (ovarian)
- Extremely rare primary; very malignant
- Elevated hCG
C. SEX CORD-STROMAL TUMOURS (Ovary)
1. GRANULOSA CELL TUMOUR
- Most important clinically (~5% of malignant ovarian tumours)
- Functionally active: secretes estrogen → endometrial hyperplasia/carcinoma (in adults); precocious puberty (in children)
- Call-Exner bodies (characteristic): small follicles filled with eosinophilic secretion
- Low malignant potential but late recurrences possible
- Inhibin is a useful tumour marker
2. THECOMA-FIBROMA GROUP
- Thecoma: estrogen-secreting; post-menopausal women
- Fibroma: associated with Meigs syndrome (ovarian fibroma + ascites + right-sided pleural effusion)
3. SERTOLI-LEYDIG CELL TUMOUR (Androblastoma)
- Secretes androgens → virilization
- Rare; most are benign or low-grade malignant
Key Tumour Markers Summary
| Marker | Associated Tumour |
|---|---|
| AFP | Yolk sac tumour (testis & ovary), Embryonal carcinoma |
| hCG | Choriocarcinoma, Seminoma (low), Embryonal carcinoma |
| LDH | Dysgerminoma, Seminoma |
| Inhibin | Granulosa cell tumour |
| CA-125 | Serous ovarian carcinoma |
Testicular vs. Ovarian Germ Cell Tumour Counterparts
| Testis | Ovary | Notes |
|---|---|---|
| Seminoma | Dysgerminoma | Histologically identical; both radiosensitive |
| Yolk sac tumour | Endodermal sinus tumour | AFP positive; Schiller-Duval bodies |
| Embryonal carcinoma | Embryonal carcinoma | Rare in ovary |
| Choriocarcinoma | Choriocarcinoma | hCG positive; both highly aggressive |
| Teratoma | Mature cystic teratoma (dermoid) | Prepubertal testis = benign; ovary = usually benign |
Sources: Robbins & Kumar Basic Pathology (9780323790185), Chapter 16 (pp. 655-658) and Chapter 17 (pp. 695-700)
This is a shared conversation. Sign in to Orris to start your own chat.