laq shoulder joint vishram singh
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive information from multiple anatomy atlases to write a complete LAQ answer on the Shoulder Joint as per Vishram Singh's style. Let me compose the full answer:
Shoulder Joint (Glenohumeral Joint) - LAQ
Definition and Type
The shoulder joint (glenohumeral joint) is a multiaxial ball-and-socket synovial joint - the most mobile joint in the human body. It is formed between the head of humerus and the glenoid cavity of the scapula.
Articular Surfaces
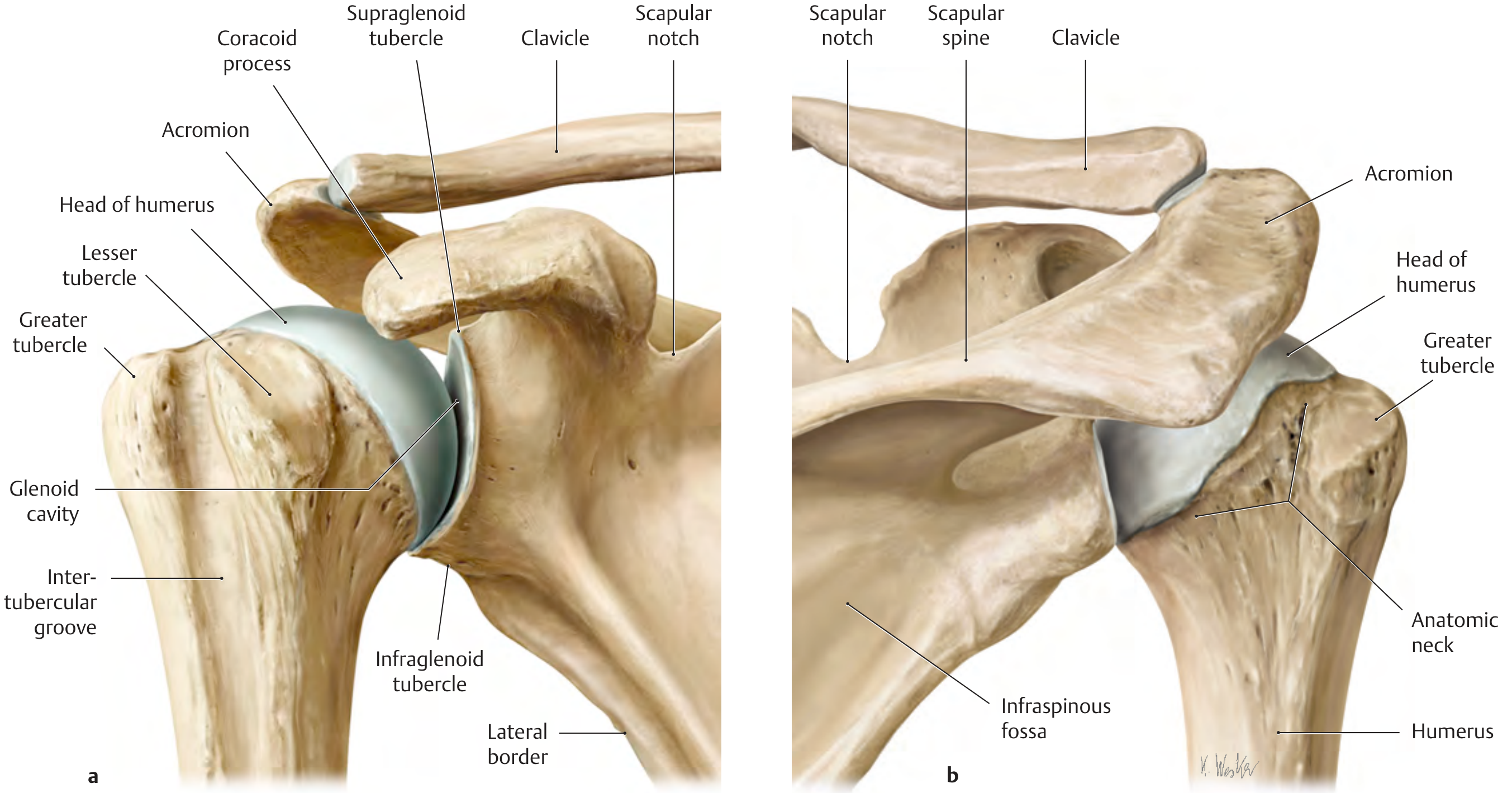
| Structure | Description |
|---|---|
| Head of humerus | Large, rounded; covered by hyaline cartilage; faces medially, upward, and backward |
| Glenoid cavity | Shallow, pear-shaped fossa on the superolateral angle of scapula; 3-4 times smaller than humeral head |
| Glenoid labrum | Fibrocartilaginous rim (~5 mm wide) that deepens the glenoid cavity slightly; attached to its margins |
The articular surface of the glenoid is tilted slightly upward (retroverted ~7°), which helps hold the humeral head. The supraglenoid tubercle gives origin to the long head of biceps brachii; the infraglenoid tubercle gives origin to the long head of triceps brachii.
Fibrous Capsule
The capsule is loose and redundant, attached:
- Medially - to the margin of the glenoid labrum (and a short distance beyond it on the glenoid neck)
- Laterally - to the anatomical neck of humerus (except inferiorly, where it extends ~1 cm below onto the surgical neck)
Key features:
- Posteriorly: thin and not reinforced by ligaments
- Anteriorly: reinforced by three glenohumeral ligaments
- Inferiorly: sags down as the axillary recess when the arm is at rest - this provides a reserve of capsule needed during abduction
- The capsule is perforated in two places:
- Anteriorly - to allow communication with the subscapular bursa
- Superiorly - for passage of the tendon of long head of biceps brachii
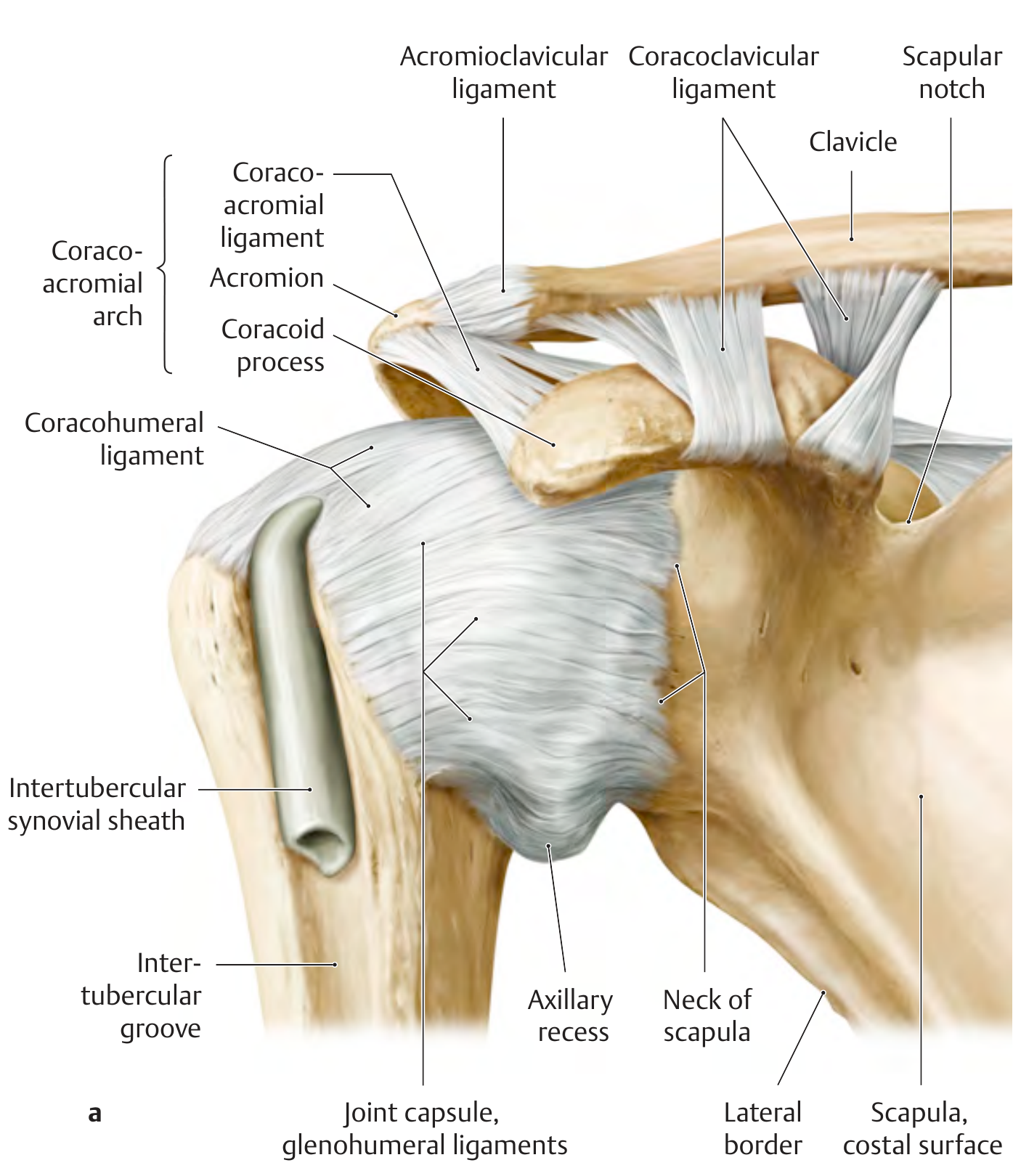
Ligaments
1. Glenohumeral Ligaments (3 bands - thickenings of anterior capsule)
| Ligament | Origin | Insertion | Function |
|---|---|---|---|
| Superior glenohumeral | Upper margin of glenoid | Lesser tubercle / intertubercular groove | Limits inferior translation; forms biceps pulley with coracohumeral lig. |
| Middle glenohumeral | Upper margin of glenoid | Anatomical neck of humerus | Limits external rotation |
| Inferior glenohumeral | Inferior glenoid margin | Middle of anatomical neck | Most important - forms a hammock during abduction; prevents anterior-inferior dislocation |
The inferior glenohumeral ligament has 3 parts: anterior band, posterior band, and the axillary recess between them.
2. Coracohumeral Ligament
- Arises from the base of the coracoid process
- Passes to the greater and lesser tubercles as two bands
- Bridges the gap (rotator interval) between supraspinatus and subscapularis
- Stabilizes the tendon of long head of biceps as it passes into the intertubercular groove
3. Transverse Humeral Ligament
- A band crossing the intertubercular groove, holding the biceps tendon in place
4. Coracoacromial Ligament (extracapsular)
- Connects the coracoid process to the acromion
- Together with acromion and coracoid, forms the coracoacromial arch - a protective roof over the shoulder
- Limits upward movement of the humeral head
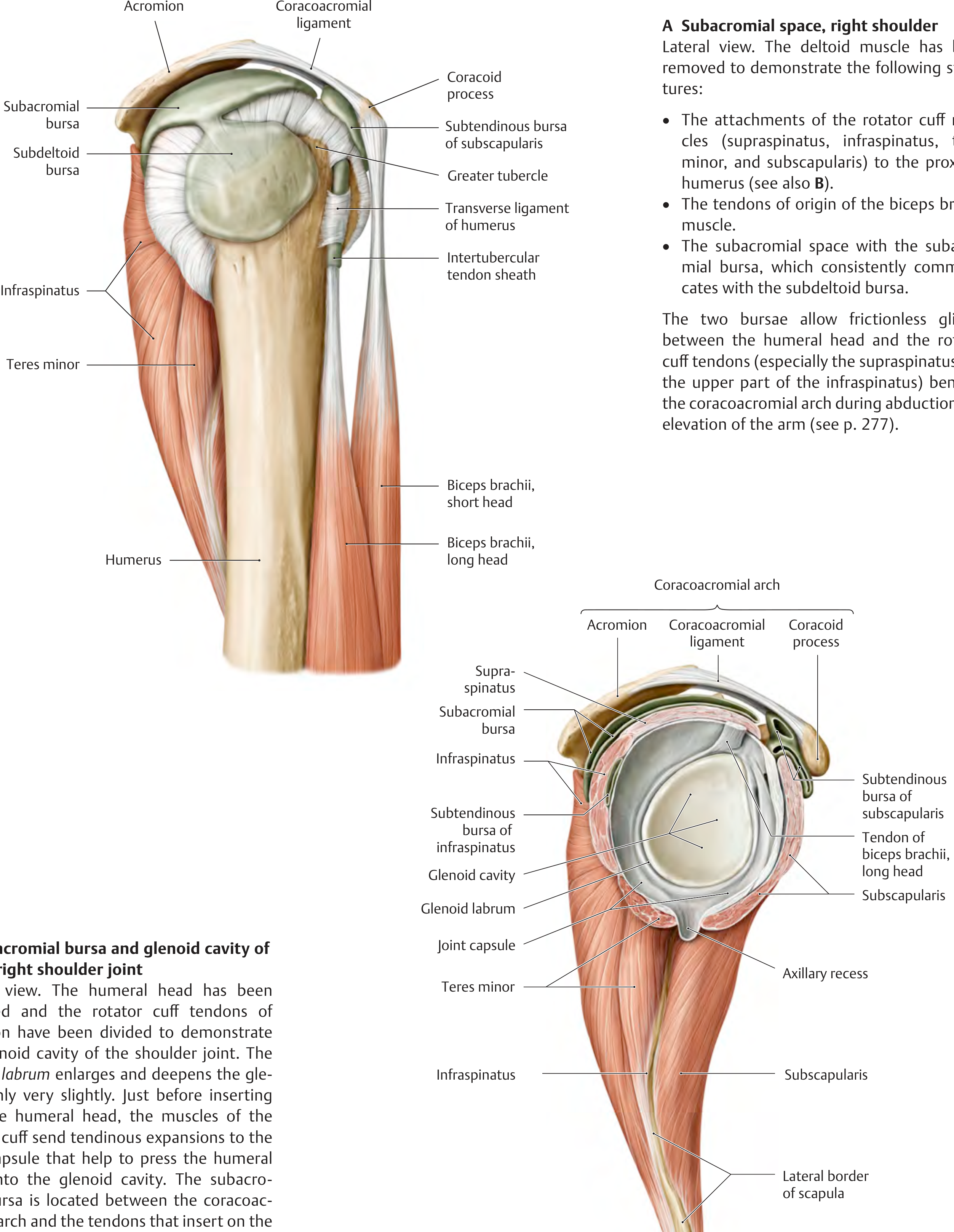
Bursae
| Bursa | Location | Communication |
|---|---|---|
| Subacromial bursa | Between coracoacromial arch and rotator cuff (supraspinatus) | Communicates with subdeltoid bursa |
| Subdeltoid bursa | Between deltoid and rotator cuff | Communicates with subacromial bursa |
| Subtendinous bursa of subscapularis | Between subscapularis tendon and scapula | Communicates with joint cavity (through anterior perforation) |
| Subtendinous bursa of infraspinatus | Behind infraspinatus tendon | May communicate with joint cavity |
| Subcoracoid bursa | Beneath coracoid process | Communicates with joint cavity |
The subacromial and subdeltoid bursae together form a large continuous unit called the subacromial-subdeltoid bursa, allowing frictionless gliding of the rotator cuff tendons under the coracoacromial arch during abduction.
Rotator Cuff (SITS Muscles)
The rotator cuff is the primary stabilizer of the glenohumeral joint, pressing the humeral head into the glenoid cavity:
| Muscle | Origin | Insertion | Nerve | Action at Shoulder |
|---|---|---|---|---|
| Supraspinatus | Supraspinous fossa | Greater tubercle (upper facet) | Suprascapular (C5,6) | Initiates abduction (first 15°) |
| Infraspinatus | Infraspinous fossa | Greater tubercle (middle facet) | Suprascapular (C5,6) | Lateral rotation |
| Teres minor | Lateral border of scapula | Greater tubercle (lower facet) | Axillary (C5,6) | Lateral rotation |
| Subscapularis | Subscapular fossa | Lesser tubercle | Lower subscapular (C5,6,7) | Medial rotation |
The tendons blend with the joint capsule, sending expansions into it - this is why the rotator cuff both moves and stabilizes the joint.
Movements and Muscles
| Movement | Range | Main Muscles |
|---|---|---|
| Flexion | 0-90° (glenohumeral) | Anterior deltoid, pectoralis major (clavicular head), coracobrachialis, biceps brachii |
| Extension | 0-45° | Posterior deltoid, teres major, latissimus dorsi, long head of triceps |
| Abduction | 0-90° (glenohumeral) | Supraspinatus (0-15°), then deltoid (15-90°) |
| Adduction | - | Pectoralis major, latissimus dorsi, teres major, coracobrachialis |
| Medial rotation | - | Subscapularis, teres major, latissimus dorsi, pectoralis major, anterior deltoid |
| Lateral rotation | - | Infraspinatus, teres minor, posterior deltoid |
| Circumduction | - | Combination of all |
Note on abduction: Full abduction to 180° requires 90° at glenohumeral joint + 60° at scapulothoracic joint + 30° at clavicular joints. The scapula must rotate upward for full elevation.
Nerve Supply
- Anterior aspect: Axillary nerve, musculocutaneous nerve
- Posterior aspect: Axillary nerve, suprascapular nerve
- Inferior aspect: Subscapular nerves
The joint is supplied by C5 and C6 nerve roots (Hilton's law: same nerves that supply muscles acting on a joint also supply the joint itself).
Blood Supply
- Anterior circumflex humeral artery (branch of axillary artery) - mainly supplies humeral head
- Posterior circumflex humeral artery (branch of axillary artery)
- Suprascapular artery
- Thoracoacromial artery
Relations
| Direction | Structures |
|---|---|
| Anterior | Subscapularis muscle, coracobrachialis, biceps brachii short head |
| Posterior | Infraspinatus, teres minor |
| Superior | Supraspinatus, coracoacromial arch |
| Inferior | Axillary nerve and posterior circumflex humeral artery (in quadrilateral space); long head of triceps |
The axillary nerve is intimately related to the inferior capsule and is at risk in:
- Inferior dislocations
- Surgical neck fractures
- Deep intramuscular injections in the deltoid (should be given in the upper outer quadrant)
Applied Anatomy / Clinical Points
1. Dislocation (Most Common of All Joints - 45% of all dislocations)
- Anteroinferior dislocation is by far the most common (95%)
- Mechanism: forcible external rotation + abduction of the raised arm
- The humeral head slips below the weak inferior capsule and comes to rest below the coracoid process (subcoracoid dislocation)
- The head presses against the anteroinferior glenoid rim causing:
- Bankart lesion - avulsion of the glenoid labrum + rim fragment
- Hill-Sachs lesion - compression fracture of posterosuperior humeral head
- Complications:
- Axillary nerve injury - test sensation over "regimental badge area" (lateral deltoid)
- Axillary artery injury (especially in elderly)
- Rotator cuff tear (especially in patients >40 years)
Posterior dislocation is rare and classically occurs in epileptic fits and electric shock (due to strong internal rotator pull)
2. Rotator Cuff Tears
- Supraspinatus is most commonly torn (at its "critical zone" - ~1 cm from its insertion, a relatively avascular area)
- Painful arc: 60°-120° of abduction
- Full-thickness tears: complete loss of active abduction
3. Bankart Repair
- Arthroscopic reattachment of torn labrum + anterior capsule tightening
4. Frozen Shoulder (Adhesive Capsulitis)
- The axillary recess becomes fibrosed and adherent
- Results in severe restriction of all shoulder movements, especially external rotation
5. Subacromial Impingement
- Inflammation/compression of supraspinatus tendon between greater tubercle and coracoacromial arch
- Painful on abduction between 60°-120° (painful arc sign)
6. Injection Site
- Shoulder joint can be injected anteriorly (below coracoid process, between coracoid and head of humerus) or posteriorly (2 cm below and medial to posterior corner of acromion)
Why the Shoulder is Most Mobile But Least Stable
The glenohumeral joint sacrifices stability for mobility because:
- Glenoid cavity is shallow (only slightly deepened by labrum)
- Articular surfaces are markedly incongruent - glenoid is 3-4x smaller than humeral head
- Capsule is loose and redundant
- Ligaments are weak and few
- Stability depends primarily on the rotator cuff muscles rather than bony architecture
This is the evolutionary trade-off as the upper limb changed from a weight-bearing organ (as in quadrupeds) to a manipulative organ - mobility was gained at the cost of stability.
Sources: THIEME Atlas of Anatomy - General Anatomy and Musculoskeletal System; Gray's Anatomy for Students
This is a shared conversation. Sign in to Orris to start your own chat.