Make acute abdomen answer for md radiology exam for 10 marks should include images
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Finding Sources
Reading File
Loading Image
Loading Image
I now have extensive content and images. Let me compile the comprehensive MD Radiology exam answer.
ACUTE ABDOMEN - RADIOLOGY APPROACH
MD Radiology Examination Answer (10 Marks)
DEFINITION
Acute abdomen refers to a clinical syndrome of acute, severe abdominal pain requiring urgent diagnostic evaluation and, often, immediate surgical or medical intervention. From a radiological perspective, the role of imaging is to rapidly identify life-threatening pathology, guide triage, and direct management.
IMAGING MODALITIES IN ACUTE ABDOMEN
1. Plain Radiograph (AXR + Erect CXR)
The plain abdominal radiograph (AXR) was historically the principal imaging investigation. In current practice, it has been largely replaced by ultrasound (US) and CT following senior clinical assessment. The AXR retains validity in two main situations:
- Detection of visceral perforation (pneumoperitoneum)
- Assessment of bowel dilatation (obstruction)
Plain AXR is not recommended for diagnosing appendicitis, cholecystitis, diverticulitis, or pancreatitis.
Standard radiographs: Supine AXR + Erect chest radiograph (CXR). The patient should ideally remain erect for 10 minutes before CXR to allow free gas to rise.
KEY RADIOLOGICAL FINDINGS
A. PNEUMOPERITONEUM (Free Peritoneal Gas)
Erect CXR - most sensitive plain film view:
- Free gas appears as a crescentic lucency under the diaphragm (usually the right hemidiaphragm)
- As little as 1 mL of free gas can be detected
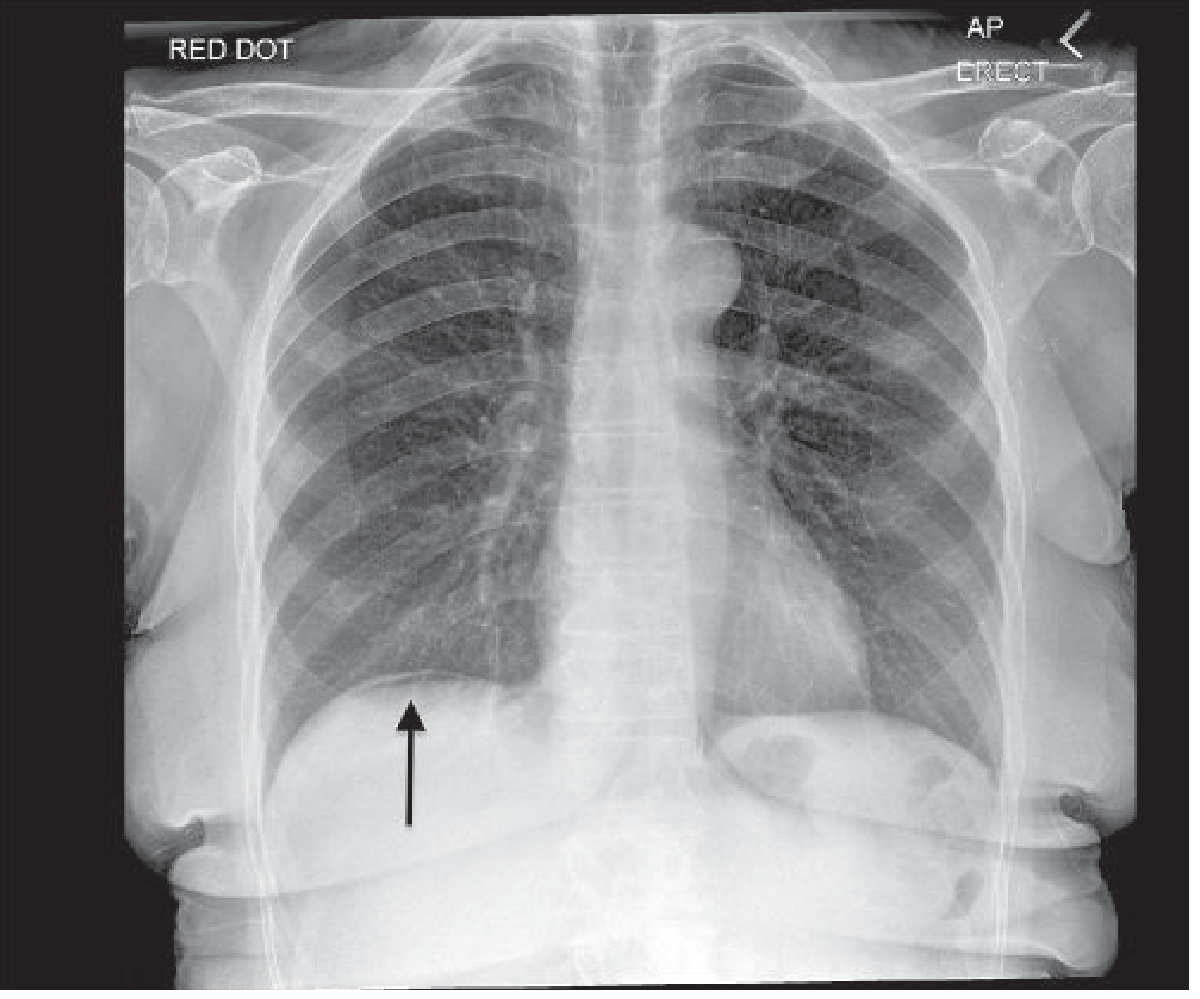
Fig. 1: Pneumoperitoneum on erect CXR - free gas seen between liver and right hemidiaphragm (arrow). (Grainger & Allison's Diagnostic Radiology)
Supine AXR signs of pneumoperitoneum:
| Sign | Description |
|---|---|
| Rigler's Sign (double wall sign) | Gas visible on both sides of the bowel wall - inner (luminal) and outer (peritoneal) |
| Falciform ligament sign | Falciform ligament outlined by gas on both sides |
| Inverted V sign | Medial umbilical ligaments outlined by gas |
| Morrison's pouch gas | Gas in the hepatorenal fossa (right upper quadrant) |
| Triangular air | Triangular gas pockets between bowel loops |
CT is the most sensitive investigation for free peritoneal gas. Images must be reviewed on lung window settings (W:1500, L:-600) to detect small volumes.
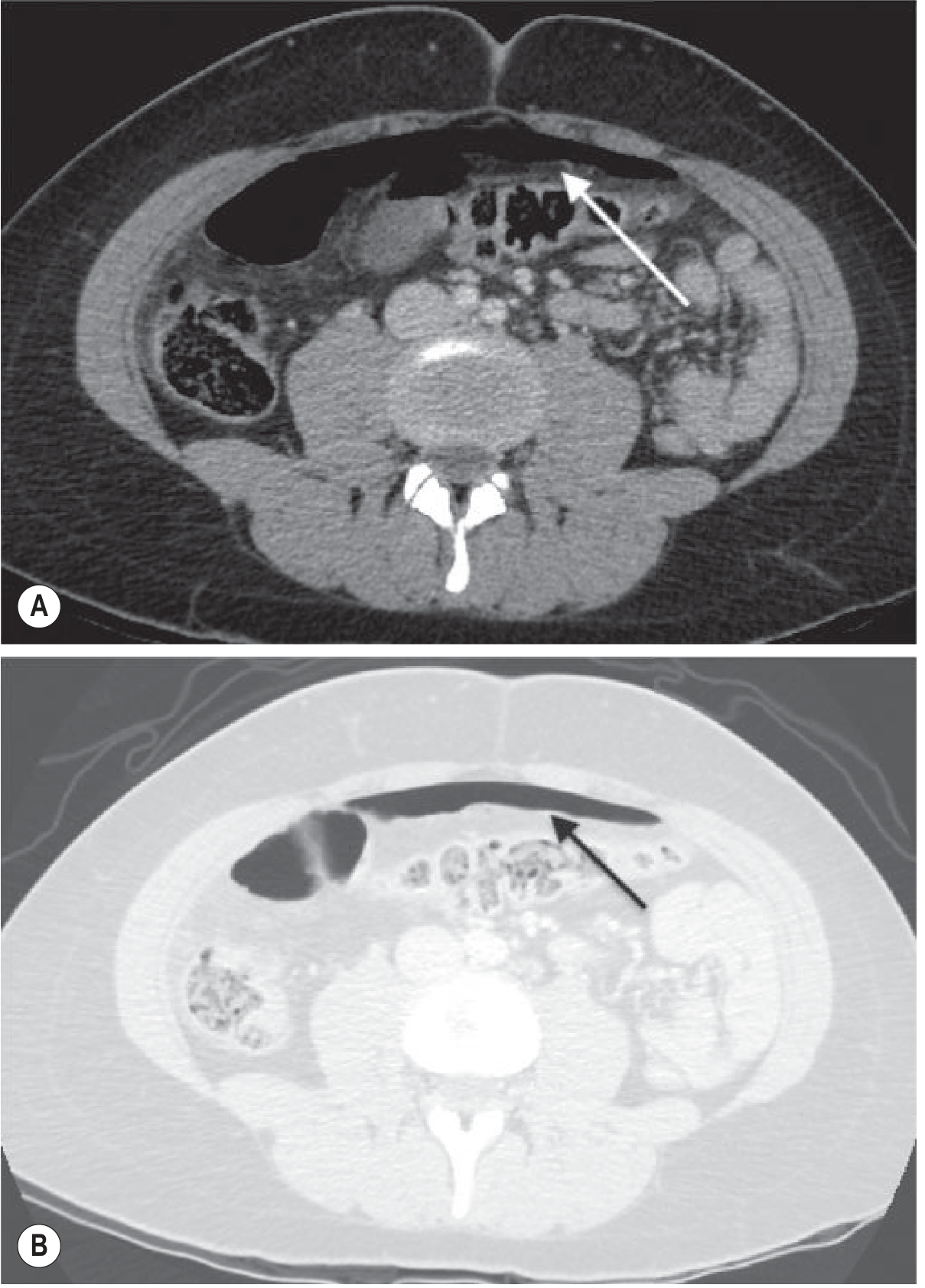
Fig. 2: CT abdomen - free peritoneal gas due to perforated viscus. (A) Soft tissue windows - gas difficult to see. (B) Lung windows (W:1500, L:-600) - free gas anterior to abdominal wall clearly visible. (Grainger & Allison's)
Causes of pneumoperitoneum WITHOUT peritonitis (Table 18.4):
- Postoperative (up to 7 days)
- Peritoneal dialysis
- Silent perforation of viscus (elderly, steroids, unconscious)
- Pneumatosis intestinalis (cyst rupture)
- Tracking from pneumomediastinum
- Vaginal-tubal entry of air
Differential for subdiaphragmatic gas-mimics: Chilaiditi syndrome (colon interposed under diaphragm), subphrenic abscess (see below).
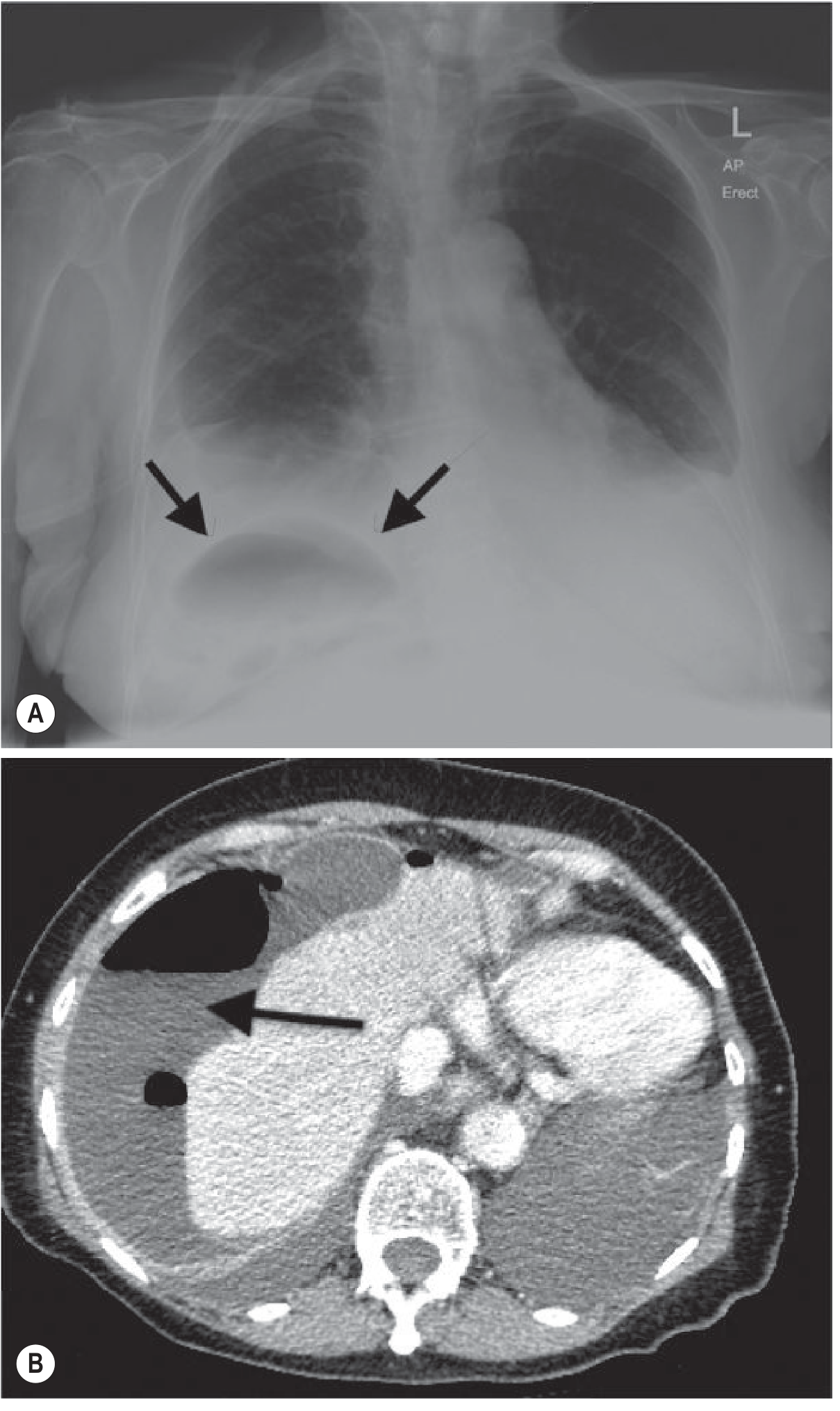
Fig. 3: Subphrenic abscess - erect CXR shows air-fluid level under right hemidiaphragm (A); CT confirms collection (B). (Grainger & Allison's)
B. BOWEL OBSTRUCTION
Small Bowel Obstruction (SBO):
- Distended small bowel loops (>3 cm), central position, multiple loops
- Valvulae conniventes (plicae circulares) are thin, frequent, span the full width of the bowel
- String of beads sign - gas bubbles trapped between valvulae conniventes in fluid-filled dilated loops (virtually diagnostic of SBO)
- AXR sensitivity for SBO: ~66% (fluid-filled loops invisible on plain film)
- CT is superior - shows transition point, fluid-filled loops, and causative lesion
Large Bowel Obstruction (LBO):
- Dilated colon (>6 cm; caecum >9 cm is high risk for perforation)
- Peripheral/framing distribution
- Haustral folds are broad, widely spaced, and do NOT span the full width
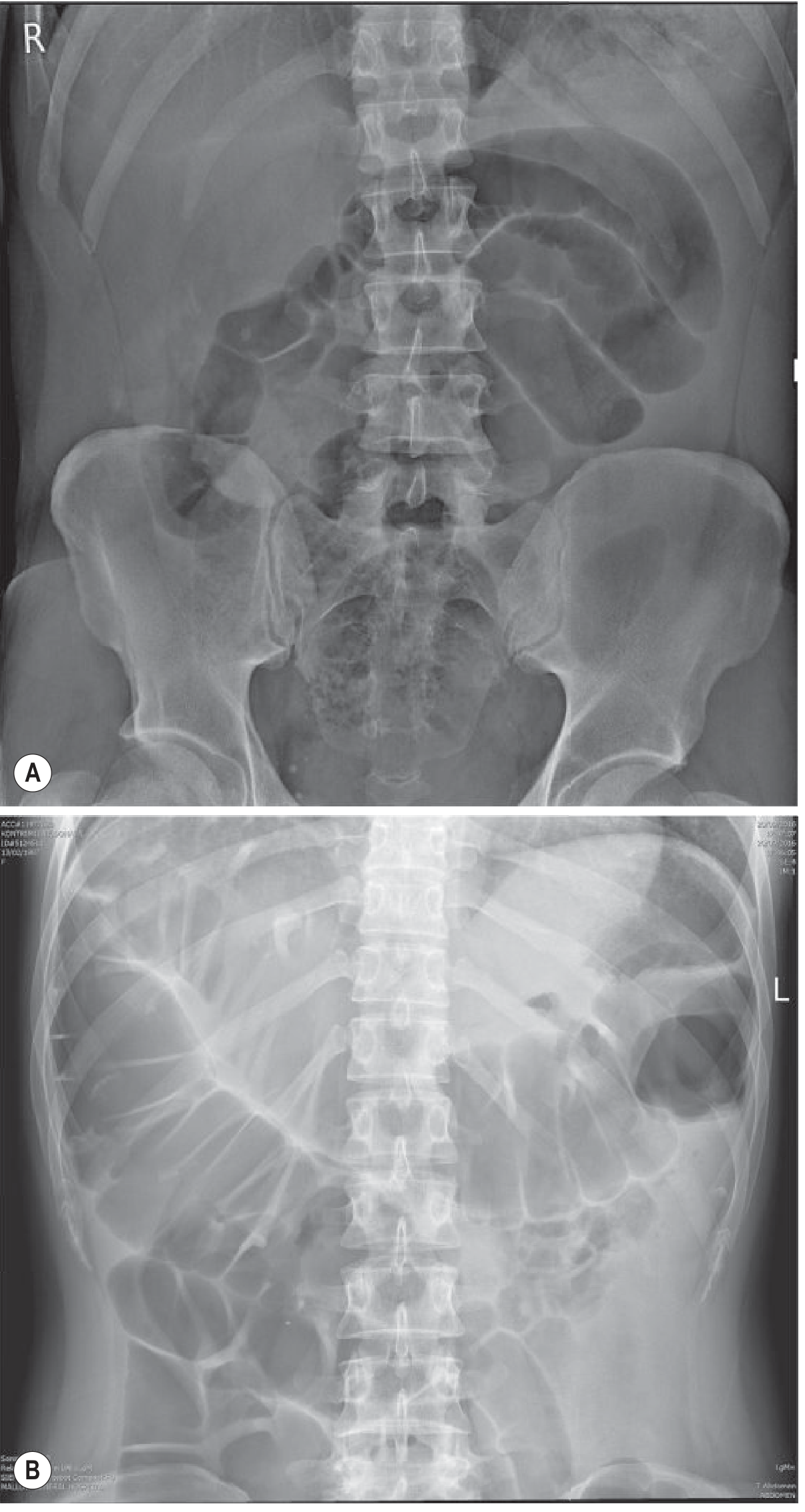
Fig. 4: Bowel obstruction. (A) Small bowel obstruction - central distended loops with valvulae conniventes. (B) Large bowel obstruction - peripheral dilated loops with haustral markings. (Grainger & Allison's)
Gallstone Ileus (special case):
Rigler's triad on AXR:
- SBO
- Pneumobilia (gas in biliary tree - branching, central pattern)
- Ectopic gallstone (usually RIF/pelvic loops) CT is definitive.
C. GAS IN THE BOWEL WALL (Pneumatosis Intestinalis)
Linear gas streaks in the bowel wall indicate bowel ischaemia or infarction until proven otherwise.
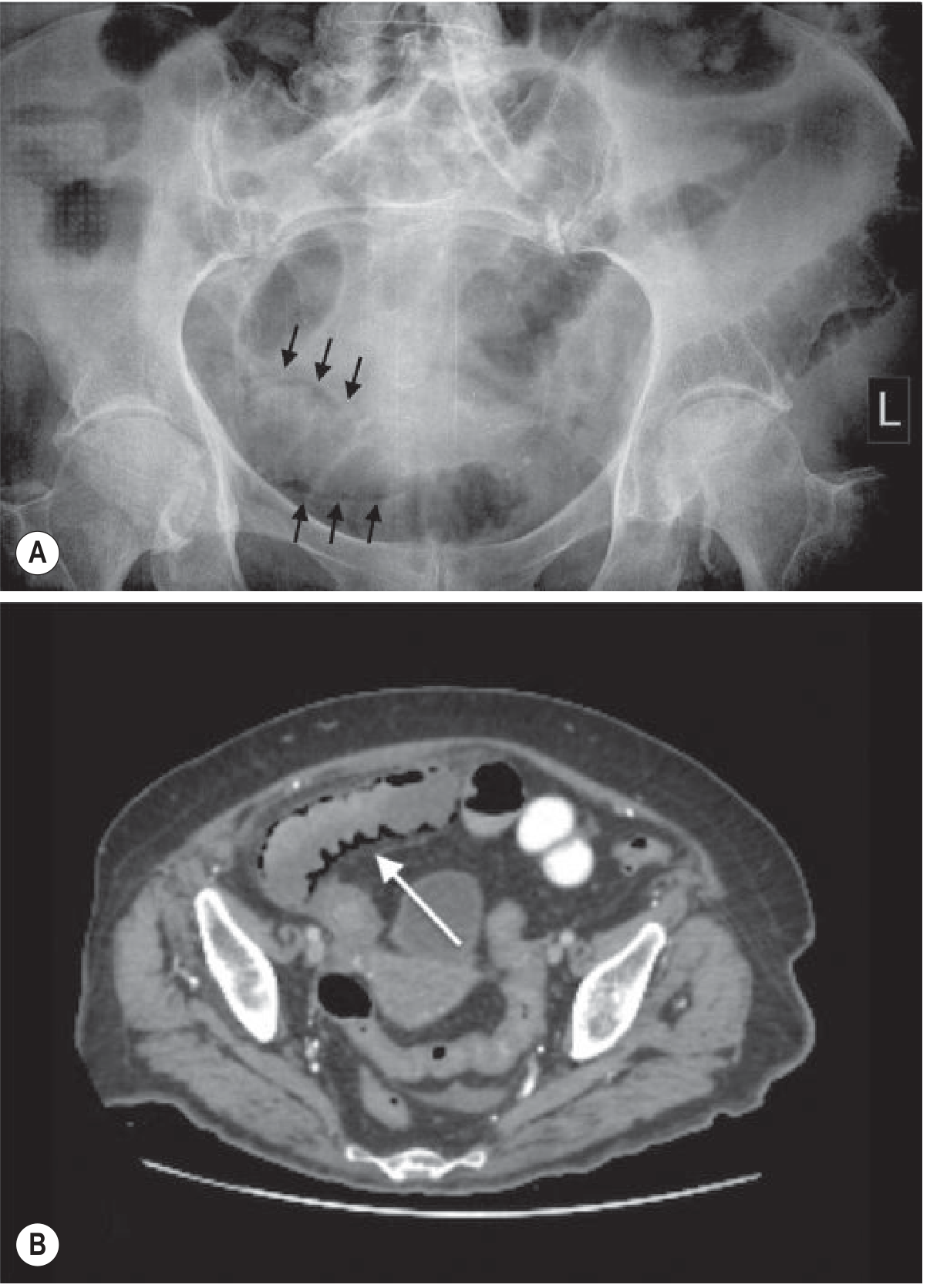
Fig. 5: Pneumatosis intestinalis in bowel ischaemia. AXR (A) shows subtle intramural gas; CT (B) confirms pneumatosis and bowel wall hypoenhancement. (Grainger & Allison's)
Portal venous gas (peripheral in liver) vs Pneumobilia (central in liver) - important distinction.
D. ACUTE INFLAMMATORY CONDITIONS
Acute Appendicitis
Ultrasound (graded compression US):
- Technique: Graduated compression probe over RIF to displace bowel
- US signs (Table 18.6):
- Blind-ending tubular non-compressible structure
- Diameter ≥7 mm
- No peristalsis
- Appendicolith (hyperechoic with acoustic shadow)
- Surrounding hyperechoic fat (periappendiceal inflammation)
- Pericaecal fluid/abscess
- Sensitivity: 78-98%; Specificity: 85-98%
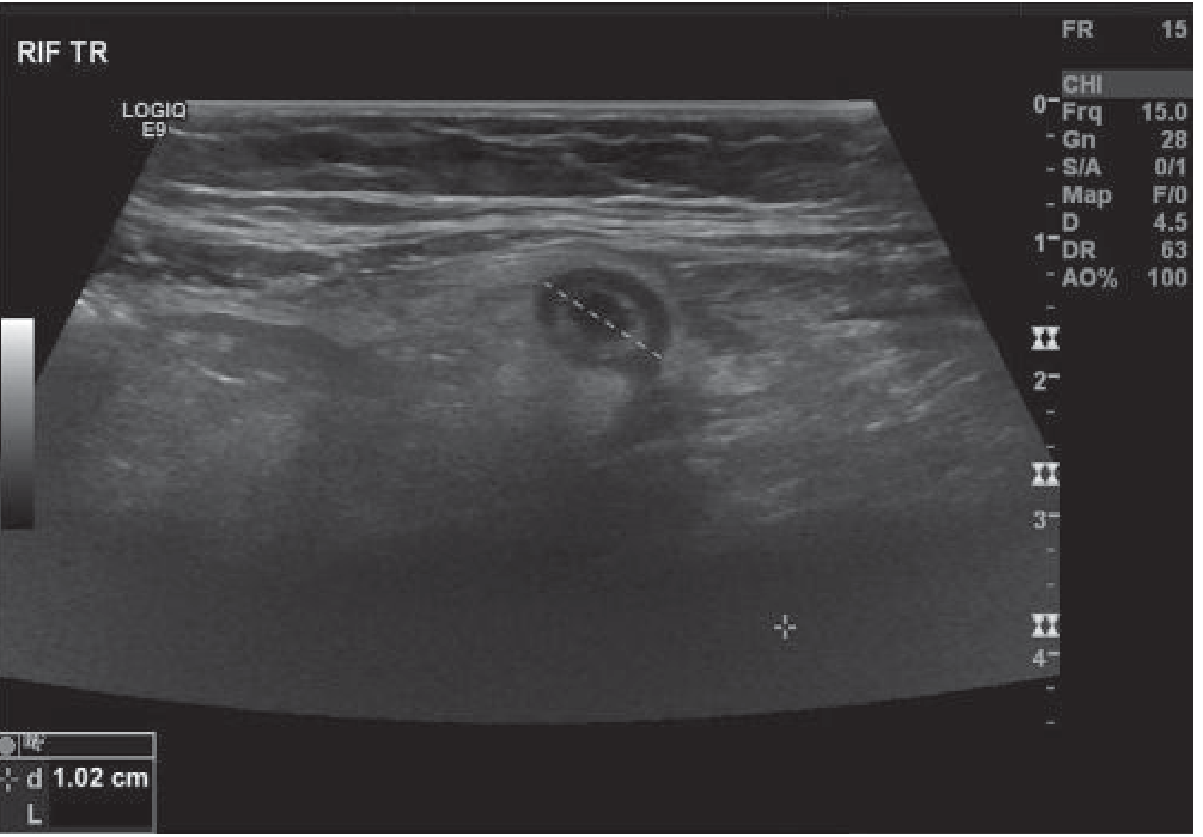
Fig. 6: Appendicitis on ultrasound - non-compressible blind-ending tubular structure in RIF measuring >7 mm. (Grainger & Allison's)
CT (contrast-enhanced): Gold standard for equivocal cases
- Thickened appendix (>6 mm), periappendiceal fat stranding
- Appendicolith as hyperdense focus
- Periappendiceal phlegmon or abscess in perforation
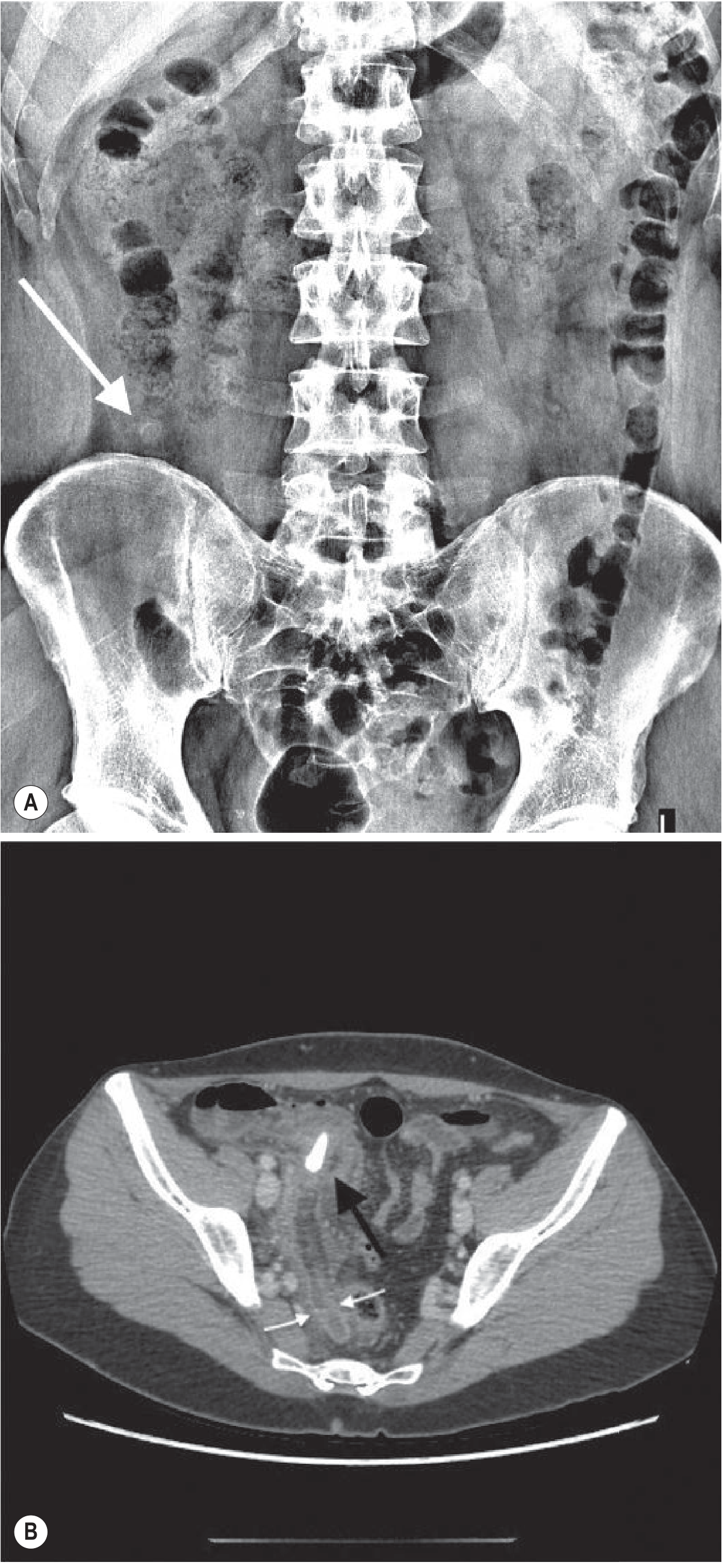
Fig. 7: Appendicitis. (A) AXR appendicolith in RIF. (B) CT confirming appendicolith within inflamed appendix. (Grainger & Allison's)
US pitfalls (false negatives): Focal tip appendicitis, retrocaecal appendix, gangrenous/perforated appendicitis, gas-filled appendix, massively enlarged appendix.
Acute Cholecystitis
- US is first-line: Gallstones (hyperechoic with posterior acoustic shadowing), thickened gallbladder wall (>3 mm), pericholecystic fluid, sonographic Murphy's sign (maximal tenderness with probe over gallbladder)
- CT if diagnosis uncertain or complications suspected
Acute Pancreatitis
- CT is the primary imaging modality; best performed 48-72 hours after onset
- CT Severity Index (Balthazar score): Grades A-E; combined with necrosis index
- Findings: Peripancreatic fat stranding, fluid collections, necrosis (non-enhancing pancreatic parenchyma)
Diverticulitis
- CT (oral + IV contrast): Pericolonic fat stranding, thickened bowel wall, diverticula, pericolic abscess, fistula
- US useful in thin patients
E. ABDOMINAL AORTIC ANEURYSM (AAA) - Vascular Catastrophe
- US: Bedside first-line; confirms diagnosis, measures diameter
- CT angiography: Definitive pre-operative assessment
- AXR: Curvilinear calcification in aortic wall (unreliable)
ROLE OF CT IN ACUTE ABDOMEN
CT with intravenous contrast is the workhorse of acute abdominal imaging. Key advantages:
- Rapid, comprehensive survey of all abdominal organs
- Identifies perforation, obstruction, ischaemia, inflammation, and vascular pathology
- Guides operative and interventional planning
Radiation dose reduction strategies:
- Automatic tube current modulation (ATCM)
- Iterative reconstruction algorithms (reduce image noise, allow lower mAs)
- Low-dose CT protocols (especially in young patients and children)
ROLE OF MRI IN ACUTE ABDOMEN
Growing role due to absence of ionising radiation. Particularly indicated for:
- Pregnant patients - avoids fetal radiation exposure; optimal for appendicitis, cholecystitis, renal colic
- Children - as per ALARA (As Low As Reasonably Achievable) principle
- Recurrent inflammatory bowel disease - avoids cumulative dose
- Meta-analysis (30 studies) shows high diagnostic accuracy for appendicitis and inflammatory conditions
Limitations: Longer scan time, limited availability, motion artefact, lower sensitivity for small amounts of free gas.
American College of Radiology (ACR) recommends selective use of MRI in appropriate clinical scenarios for acute abdomen workup.
APPROACH ALGORITHM
Acute Abdomen
│
├── Suspected perforation ──► Erect CXR → CT (confirmatory)
│
├── Bowel obstruction ──► AXR → CT (transition point, cause)
│
├── Appendicitis (non-pregnant adult) ──► US → CT (if US equivocal)
│
├── Appendicitis (pregnant / child) ──► US → MRI
│
├── Cholecystitis ──► US (first-line) → CT/HIDA
│
├── Pancreatitis ──► US (gallstones) → CT (at 48-72h)
│
├── AAA / vascular ──► US (bedside) → CT angiography
│
└── Unclear / complex ──► CT (contrast-enhanced)
SUMMARY TABLE
| Condition | First-Line | Second-Line | Key Findings |
|---|---|---|---|
| Perforation | Erect CXR | CT (lung windows) | Subdiaphragmatic free gas; Rigler's sign |
| SBO | AXR | CT | Central dilated loops, valvulae conniventes, string of beads |
| LBO | AXR | CT | Peripheral dilation, haustration, transition point |
| Appendicitis | US | CT / MRI | ≥7 mm non-compressible tube, periappendiceal stranding |
| Cholecystitis | US | CT | Gallstones, wall thickening, Murphy's sign |
| Pancreatitis | US | CT | Fat stranding, necrosis, fluid collections |
| Ischaemia | AXR | CT | Pneumatosis, portal venous gas, hypoenhancement |
| AAA | US | CT-A | Aneurysm diameter, retroperitoneal haematoma |
Source: Grainger & Allison's Diagnostic Radiology: A Textbook of Medical Imaging (Chapter 18 - Acute Abdomen Imaging), supplemented by Sabiston Textbook of Surgery.
Make same for ectopic pregnancy for 10 marks
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
Loading Image
Reading File
Loading Image
I now have all the content and images needed for a comprehensive answer. Let me compose the full MD Radiology exam answer:
ECTOPIC PREGNANCY - RADIOLOGY APPROACH
MD Radiology Examination Answer (10 Marks)
DEFINITION
Ectopic pregnancy (EP) is the abnormal implantation of the embryo outside of the endometrial cavity. It is a leading cause of maternal death in the first trimester of pregnancy, primarily from rupture and haemorrhage.
EPIDEMIOLOGY & SITES OF IMPLANTATION
- Overall incidence: 2% in the general population; rises to 2.1%-8.6% in the IVF population and 11% with underlying fallopian tube abnormality
- Fallopian tube: 82% (most common - especially ampulla)
- Ovary: 5%
- Intra-abdominal: 1.4%
- Caesarean scar: 1%
- Cervix: <1%
- Interstitium (cornual): rare but most dangerous
- Bilateral EP: 1:750-1580; Heterotopic (co-existing IUP + EP): 1 in 3000 general population; up to 1 in 100 in IVF patients
RISK FACTORS
| Category | Specific Factors |
|---|---|
| Tubal damage | Pelvic inflammatory disease, STI history |
| Prior surgery | Tubal surgery, tubal sterilisation |
| Contraception | IUD in situ at time of conception |
| Reproductive | IVF/ART, previous ectopic pregnancy |
| Demographics | Age 35-44, cigarette smoking |
| Other | Prior pharmacologically induced abortion |
PATHOPHYSIOLOGY
Fertilisation normally occurs in the ampullary segment of the fallopian tube. In EP, the fertilised ovum implants before reaching the endometrial cavity, most often due to:
- Damage to tubal mucosa from prior infection (preventing transport)
- Tubal surgery or strictures
- Defects in the ovum causing premature implantation
- Elevated oestradiol/progesterone inhibiting tubal migration
The ovum penetrates the muscular wall; maternal blood seeps into tubal tissue. The tube gradually distends until rupture occurs, causing potentially catastrophic haemorrhage.
IMAGING APPROACH
Modality Hierarchy
Suspected Ectopic Pregnancy
│
Urine/Serum β-hCG (positive)
│
Transvaginal Ultrasound (FIRST-LINE)
│
├── IUP confirmed → EP excluded (unless heterotopic risk)
├── EP confirmed → Treat
└── Indeterminate → Serial β-hCG + repeat US / MRI / Laparoscopy
1. TRANSVAGINAL ULTRASOUND (TVUS) - PRIMARY MODALITY
TVUS is the imaging modality of choice for evaluating newly diagnosed pregnancy location. It is superior to transabdominal US due to:
- Higher frequency transducer (better near-field resolution)
- Closer proximity to pelvic structures
- No need for full bladder
- Earlier detection of intrauterine or extrauterine gestation
Transabdominal US should always be performed in addition for a wider field of view, detection of haemoperitoneum extending to the hepatorenal fossa, and assessment of adnexal masses not seen on TVUS.
US FINDINGS - INTRAUTERINE PREGNANCY (Normal - to exclude EP)
Normal Early IUP Milestones:
- Gestational sac (round, thick echogenic ring with sonolucent centre): first sign of IUP; appears eccentrically within endometrial cavity as pregnancy progresses
- Yolk sac within the gestational sac: diagnostic of IUP (and excludes EP at that site)
- Embryo with cardiac activity: definitive viable IUP
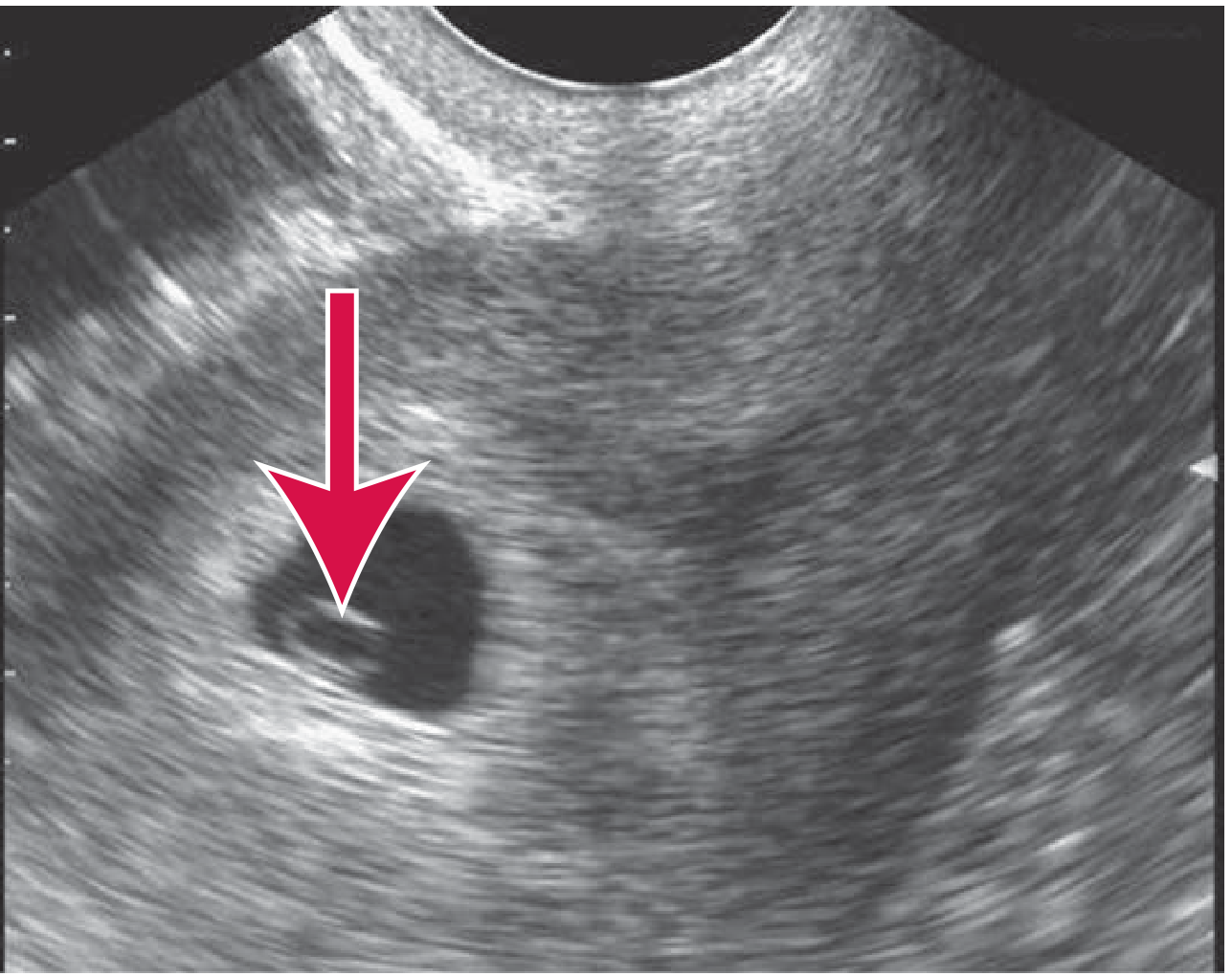
Fig. 1: Normal IUP - yolk sac (arrow) within gestational sac on transvaginal US. (Tintinalli's Emergency Medicine)
Double Decidual Sac Sign (DDSS): Two concentric echogenic rings separated by a hypoechogenic space (decidua capsularis + parietalis). Best seen on transabdominal US. Helps distinguish a true gestational sac from a pseudogestational sac. Sensitivity 64%-95%.
US FINDINGS - ECTOPIC PREGNANCY
Direct Signs of EP (listed in order of specificity):
| Sign | Description | Sensitivity | Specificity |
|---|---|---|---|
| Living extrauterine embryo | Embryo with cardiac activity outside uterus | <10%-25% | ~100% |
| Extrauterine gestational sac with yolk sac | Sac + yolk sac in adnexa | 10%-17% | ~100% |
| Tubal ring ("ring of fire") | Hyperechoic ring with central hypoechoic area; increased vascularity on colour Doppler around it | 20%-65% | 99.5%-100% |
| Adnexal mass separate from ovary | Any non-simple-cyst adnexal mass | 84% | 98% (most sensitive + specific combined finding) |
| Heterogeneous adnexal mass | Non-specific; can represent haematoma around ectopic | Common | Moderate |
Indirect Signs of EP:
Empty uterus + free pelvic fluid is a critical combination:
| Ancillary Finding | Risk of EP (%) |
|---|---|
| Any free pelvic fluid | 52% |
| Complex pelvic mass | 72% |
| Moderate/large free pelvic fluid | 86% |
| Tubal ring sign | >95% |
| Adnexal mass + free fluid | 97% |
| Hepatorenal (Morrison's pouch) free fluid | ~100% |
Echogenic free fluid (haemoperitoneum) = 96% specificity for EP and suggests rupture.
Pseudogestational sac: Intrauterine fluid collection seen in 8%-29% of EP - represents decidual cast/bleeding into endometrial cavity. Centrally located (unlike true sac which is eccentric). Clots within it may mimic a fetal pole. Key pitfall - must not be mistaken for an IUP.
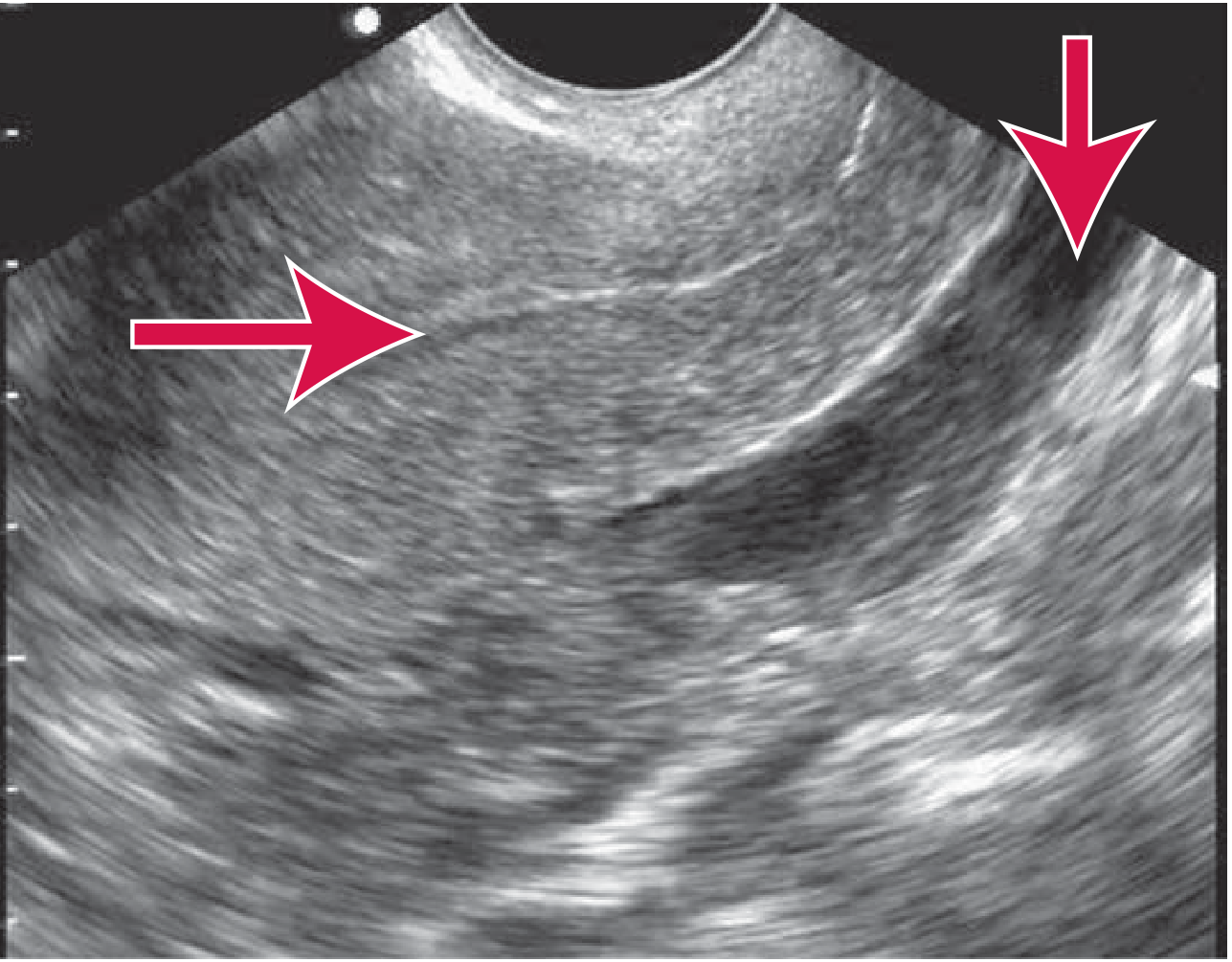
Fig. 2: Ectopic pregnancy - empty uterus with free fluid in posterior cul-de-sac. (Tintinalli's Emergency Medicine)
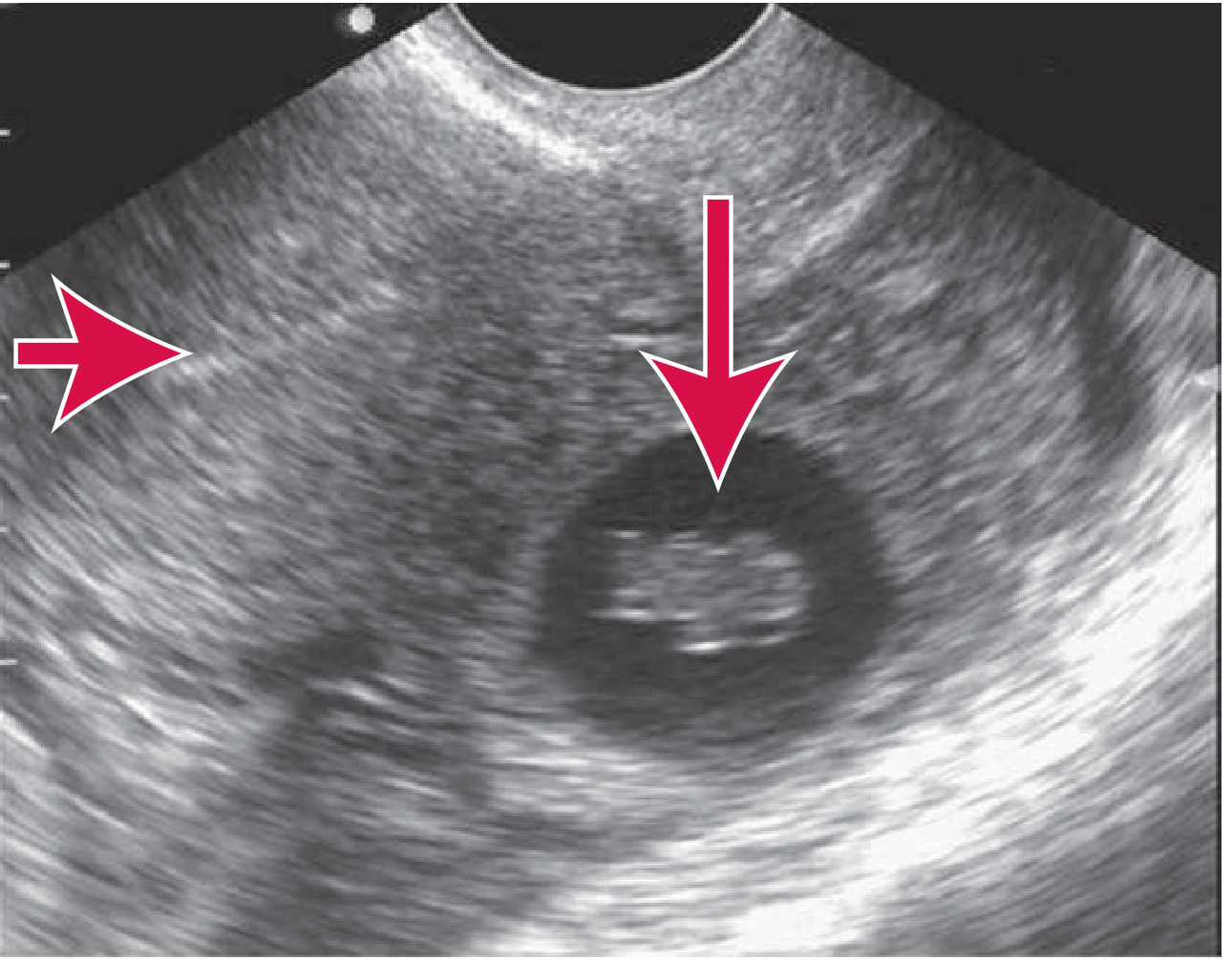
Fig. 3: Diagnostic ectopic pregnancy on US - living extrauterine embryo (vertical arrow) with empty uterus (horizontal arrow). (Tintinalli's Emergency Medicine)
2. β-hCG AND THE DISCRIMINATORY ZONE
The discriminatory zone is the β-hCG level at which an IUP should be visible on US:
- TVUS discriminatory zone: 1,500-2,000 mIU/mL
- Transabdominal US: ~6,000 mIU/mL
Interpretation:
- β-hCG > discriminatory zone + empty uterus = suspect EP
- β-hCG < discriminatory zone + empty uterus = indeterminate (early normal pregnancy cannot be excluded; repeat)
- β-hCG levels do NOT correlate with the size or viability of an EP
Important caveat: EP can occur even at very low β-hCG levels (<500 mIU/mL). Intervention should NOT be based on a single hCG level alone in a haemodynamically stable patient.
β-hCG Expected Levels (Post-Conception):
| Post-Conception | β-hCG (mIU/mL) |
|---|---|
| <1 week | 5-50 |
| 1-2 weeks | 50-500 |
| 2-3 weeks | 100-5,000 |
| 3-4 weeks | 500-10,000 |
| 4-5 weeks | 1,000-50,000 |
In a normal IUP, β-hCG doubles every 48-72 hours. In EP, the rise is typically slower (suboptimal rise) or β-hCG may plateau/decline.
3. SPECIAL SUBTYPES AND US FEATURES
Interstitial (Cornual) Ectopic Pregnancy
- Implants in the intramural portion of the fallopian tube within the uterine wall
- US: Eccentrically positioned gestational sac within the endometrial cavity or ≤5 mm of surrounding myometrium (interstitial line sign - echogenic line extending from endometrial cavity to gestational sac)
- Presents later than tubal EP (higher β-hCG at diagnosis)
- Rupture causes catastrophic haemorrhage due to proximity to uterine arteries
Cervical Ectopic Pregnancy
- US: Figure-of-8 appearance to the uterus (gestational sac in cervical canal below the level of uterine vessels)
- Must be distinguished from a miscarriage in progress (products of conception prolapsing through cervical canal)
- Colour Doppler: demonstrates vascularity around the cervical sac in a true cervical EP
Caesarean Scar Ectopic Pregnancy (CSP)
- Rising incidence with increasing Caesarean delivery rates
- US: Gestational sac implanted within the anterior lower uterine segment at the CS scar
- Thin or absent myometrium anteriorly
- Colour Doppler: increased vascularity at scar site
Ovarian Ectopic Pregnancy
- US: Ring-like structure within ovarian parenchyma
- Cannot be separated from the ovary (unlike tubal EP)
4. COLOUR DOPPLER IN ECTOPIC PREGNANCY
- Ring of fire sign: Marked peripheral vascularity around the ectopic gestational sac due to trophoblastic invasion with low-resistance, high-velocity flow. Highly specific (99.5%-100%) but low sensitivity (20%-65%)
- Helps distinguish an ectopic sac from a corpus luteum cyst (also shows flow, but less pronounced and different pattern)
- Useful in identifying interstitial EP: vascular ring within the myometrium away from the endometrial cavity
5. MRI IN ECTOPIC PREGNANCY
MRI is not routinely used for EP (cost, availability, time). Its role is limited to:
- Diagnostic uncertainty where US is indeterminate
- Delayed EP presentation where β-hCG is not elevated
- Differentiating a resolving EP from other pelvic masses
- Evaluation of rare/unusual sites (scar, abdominal, interstitial) for pre-operative planning
MRI features of EP:
- T2: Heterogeneous adnexal mass; may show low-T2 signal serpiginous structures (flow voids in large vessels)
- T1: Haemorrhage appears T1 hyperintense
- The gestational sac can be identified as a T2-hyperintense ring structure
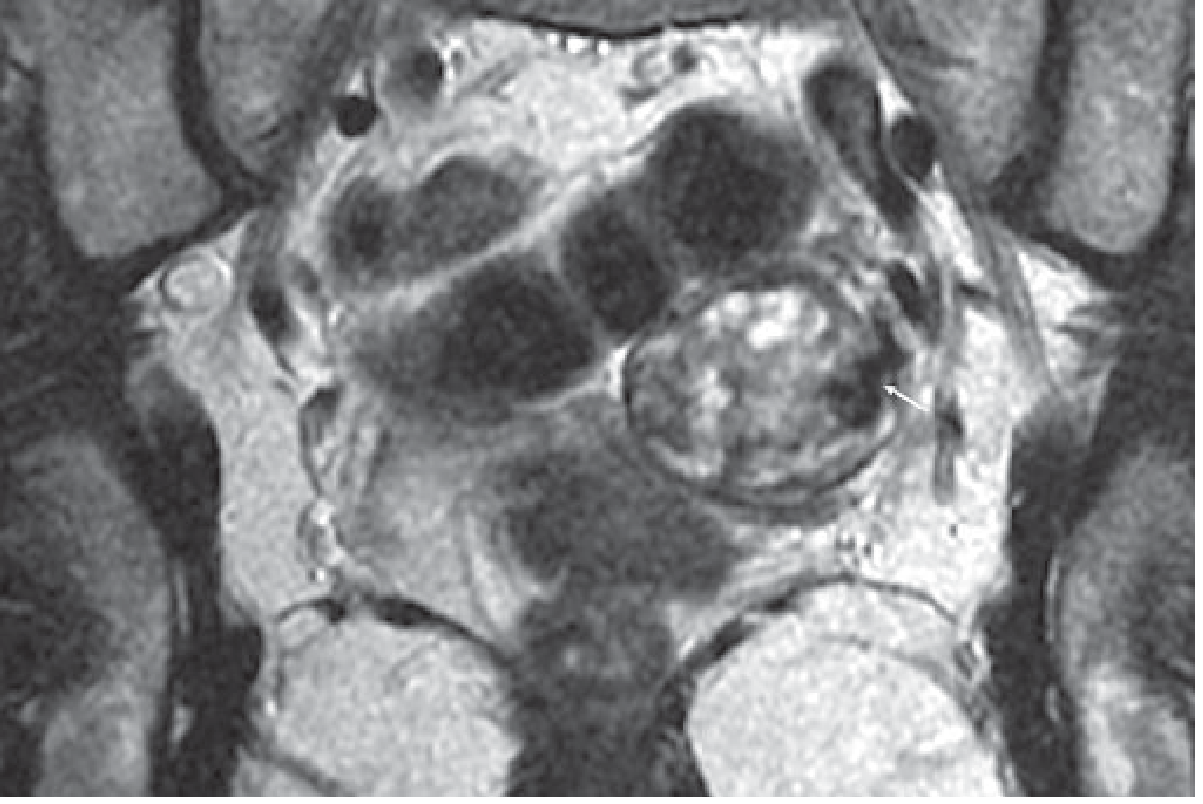
Fig. 4: MRI of ectopic pregnancy - T2-weighted coronal image showing left adnexal heterogeneous mass with flow voids (white arrow). (Grainger & Allison's Diagnostic Radiology)
6. IMAGING ALGORITHM
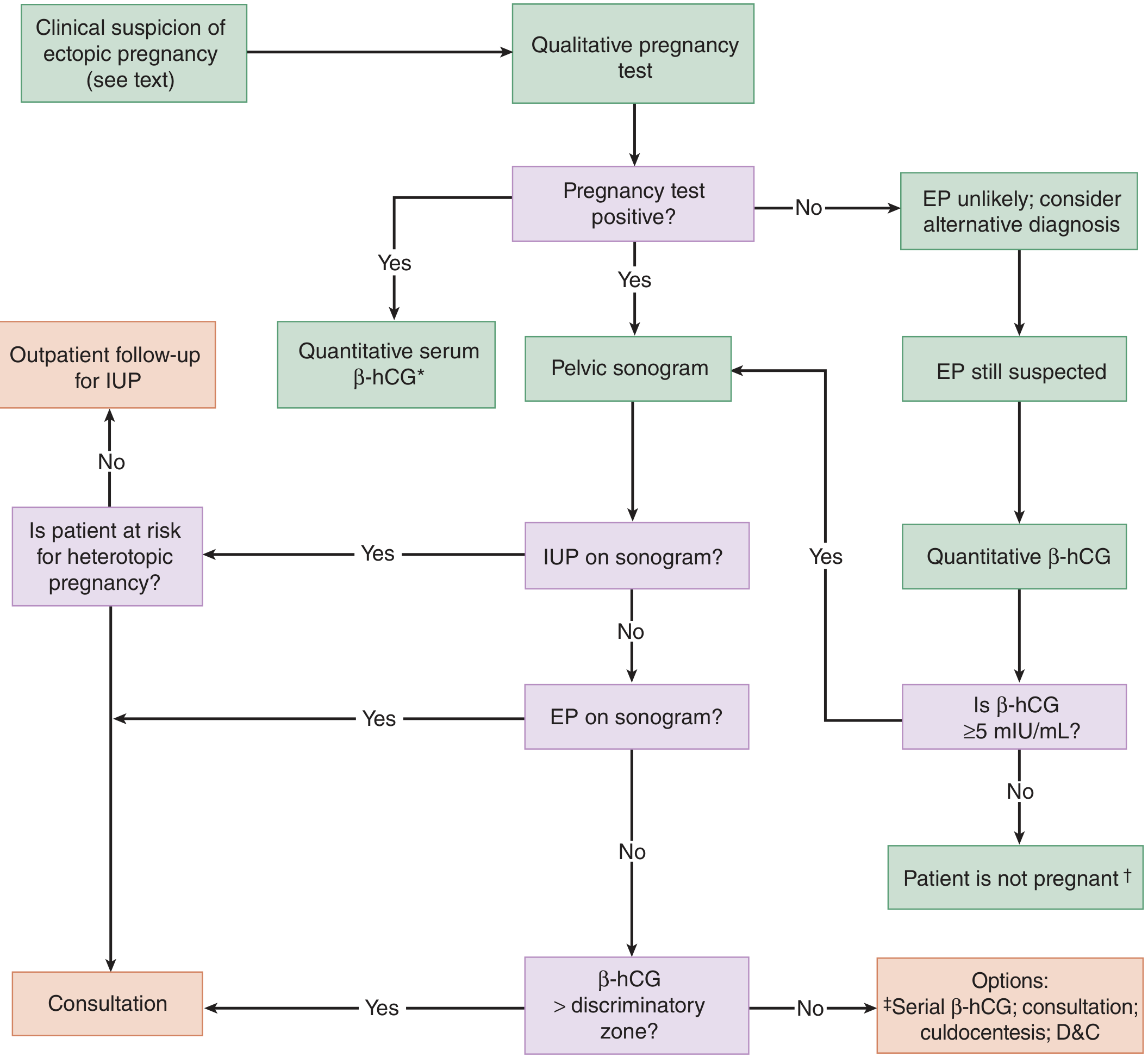
Fig. 5: Clinical-imaging algorithm for suspected ectopic pregnancy. (Tintinalli's Emergency Medicine)
7. IMAGING FINDINGS IN RUPTURED ECTOPIC PREGNANCY
Rupture is a surgical emergency. Imaging findings include:
- Free haemoperitoneum: Echogenic free fluid in the cul-de-sac, paracolic gutters, and hepatorenal fossa (Morrison's pouch - this indicates large volume haemorrhage, ~100% risk of EP)
- CT may be performed incidentally (trauma workup) or if diagnosis is uncertain:
- Free high-density fluid (haemoperitoneum: 35-70 HU) in the peritoneal cavity
- Adnexal mass ± active extravasation on CT angiography
- Empty uterus with thickened endometrium
A haemodynamically unstable patient with free intraperitoneal fluid and a positive pregnancy test should be assumed to have a ruptured EP and managed surgically without delay.
SUMMARY TABLE
| Feature | Diagnostic Value |
|---|---|
| IUP confirmed on TVUS | EP excluded (unless IVF/heterotopic risk) |
| Yolk sac in adnexa | Diagnostic of EP |
| Tubal ring + ring of fire (Doppler) | Specificity 99.5%, sensitivity 20-65% |
| Adnexal mass separate from ovary | Sensitivity 84%, specificity 98% |
| Empty uterus + β-hCG >discriminatory zone | High suspicion for EP |
| Echogenic free pelvic fluid | 96% specificity for EP |
| Hepatorenal free fluid | ~100% risk of EP |
| T2 heterogeneous adnexal mass on MRI | Useful in indeterminate/delayed cases |
KEY RADIOLOGICAL POINTS FOR EXAM
- TVUS is first-line imaging - superior to transabdominal for early pregnancy
- The most sensitive (84%) and specific (98%) US sign is an adnexal mass separate from the ovary (excluding simple cysts)
- Pseudogestational sac occurs in 8%-29% of EP - do not mistake for IUP
- Double decidual sac sign best distinguishes true sac from pseudosac
- Discriminatory zone: 1,500-2,000 mIU/mL for TVUS; absence of IUP above this level = suspect EP
- Ring of fire on colour Doppler = trophoblastic vascularity - highly specific
- Interstitial EP presents late, is most dangerous; look for eccentric sac with <5 mm surrounding myometrium
- Echogenic cul-de-sac fluid = haemoperitoneum = 96% specific for EP
- MRI reserved for indeterminate cases and unusual sites
- A ruptured EP with haemodynamic instability requires immediate surgery - do not delay for further imaging
Sources: Grainger & Allison's Diagnostic Radiology (Chapter 35), Tintinalli's Emergency Medicine (Chapter 98), Berek & Novak's Gynecology, Creasy & Resnik's Maternal-Fetal Medicine
Make full
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
!
An error occurred (ValidationException) when calling the ConverseStream operation: The model returned the following errors: messages.1.content.34.image.source.base64.data: At least one of the image dimensions exceed max allowed size for many-image requests: 2000 pixels
We encountered an error while processing your request. Please try again or reach out to us for help.
This is a shared conversation. Sign in to Orris to start your own chat.