Cardiovascular system
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Excellent - I have rich textbook content and high-quality anatomical diagrams. Now I'll compile a thorough, in-depth anatomical overview of the cardiovascular system.
Cardiovascular System - Anatomy & Structure (In-Depth)
Sources: Gray's Anatomy for Students, 4th Ed.; Braunwald's Heart Disease; Goldman-Cecil Medicine
1. Overview
The cardiovascular system consists of the heart (the pump) and a closed network of blood vessels. Its primary role is to circulate blood, delivering oxygen and nutrients to tissues and removing metabolic waste products.
2. Blood Vessels - General Structure
All blood vessel walls are composed of three concentric layers called tunics:
| Layer | Name | Composition |
|---|---|---|
| Outer | Tunica externa (adventitia) | Connective tissue |
| Middle | Tunica media | Smooth muscle ± elastic fibers |
| Inner | Tunica intima | Endothelial lining |
Arteries (3 classes)
- Large elastic arteries (e.g., aorta, pulmonary trunk, brachiocephalic, left common carotid, left subclavian) - rich in elastic fibers allowing expansion during systole and recoil during diastole to maintain continuous flow
- Medium muscular arteries (e.g., femoral, axillary, radial) - tunica media is predominantly smooth muscle, enabling regulation of diameter and blood distribution
- Small arteries and arterioles - control capillary filling and directly regulate systemic arterial pressure
Veins (3 classes)
- Large veins (e.g., superior vena cava, inferior vena cava, hepatic portal vein) - some smooth muscle in media; thickest layer is tunica externa
- Small and medium veins (e.g., superficial limb veins, deep leg veins) - thin media; tunica externa is thickest
- Venules - smallest veins; drain capillaries directly
Veins differ from arteries in that they have thinner tunica media, larger luminal diameters, often run as venae comitantes (paired vessels flanking arteries), and contain paired valves (especially in vessels below the heart) to prevent backflow.
Capillaries
The smallest vessels; connect arterioles to venules and are the site of gas, nutrient, and waste exchange with tissues.
3. The Heart - Position & Orientation
The heart is a hollow, muscular organ situated in the middle mediastinum of the thoracic cavity, enclosed within the pericardium.
Shape: Resembles a pyramid that has fallen onto one of its sides.
- Apex - projects forward, downward, and to the left; formed by the inferolateral part of the left ventricle; sits deep to the left 5th intercostal space, 8-9 cm from the midsternal line (the apex beat)
- Base (posterior surface) - quadrilateral; faces posteriorly; composed of the left atrium (mostly), small portion of the right atrium, and the proximal great veins (SVC, IVC, and pulmonary veins); fixed to the pericardial wall opposite vertebrae TV-TVIII; the esophagus lies immediately posterior
Gray's Anatomy for Students, p. 226
Surfaces
| Surface | Faces | Composed of |
|---|---|---|
| Anterior (sternocostal) | Anteriorly | Mostly right ventricle; right atrium on the right; left ventricle on the left |
| Diaphragmatic (inferior) | Inferiorly | Left ventricle + small portion right ventricle; separated by posterior interventricular groove |
| Left pulmonary | Left lung | Left ventricle + portion of left atrium |
| Right pulmonary | Right lung | Right atrium |
Borders (Radiological Significance)
In a standard posteroanterior (PA) chest X-ray:
- Right border = superior vena cava + right atrium + inferior vena cava
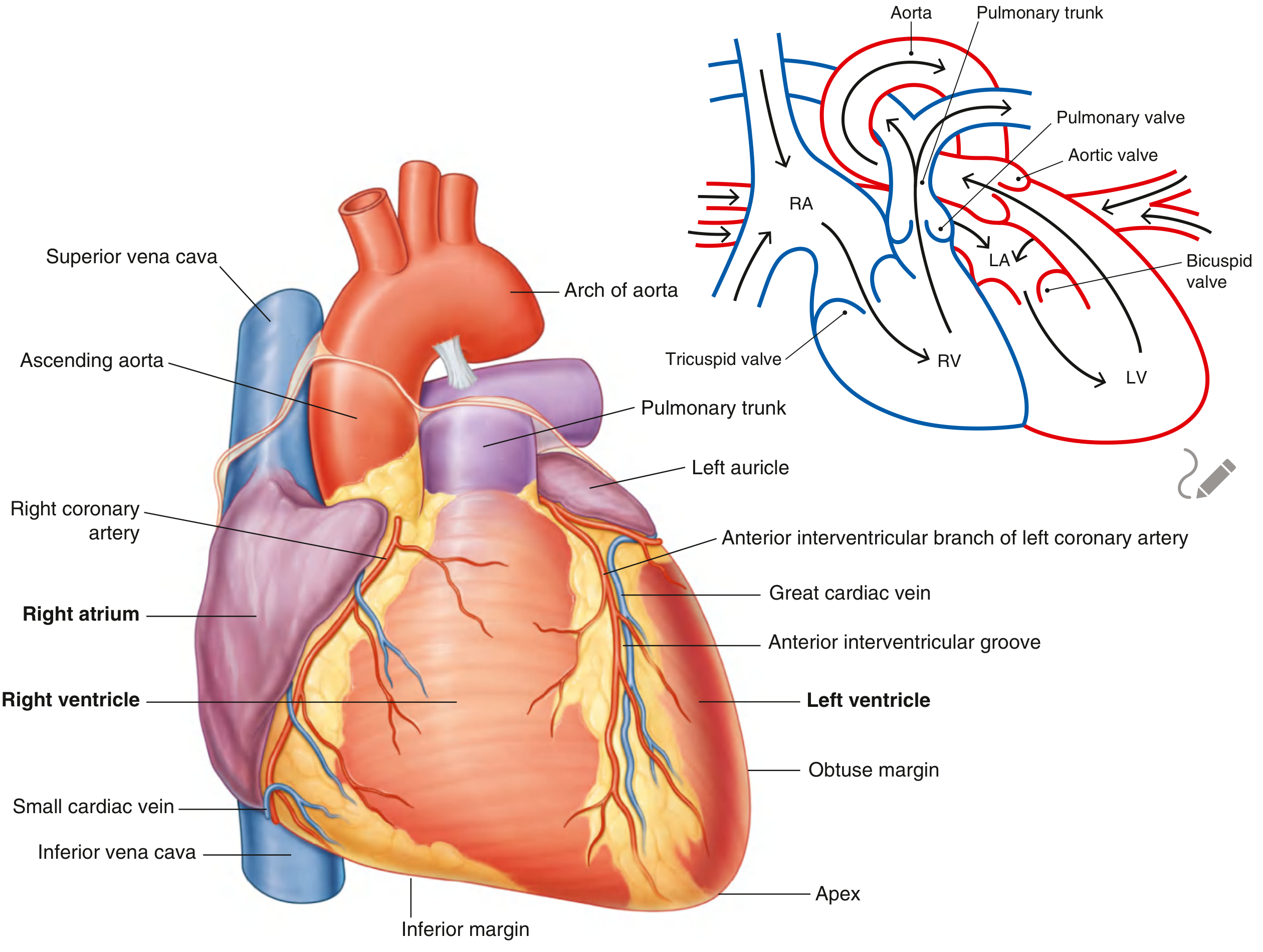
- Left border = arch of aorta + pulmonary trunk + left auricle + left ventricle
4. Cardiac Chambers
Right Atrium (RA)
- Receives deoxygenated blood from the superior vena cava (upper body), inferior vena cava (lower body), and coronary sinus (heart itself)
- Internal features:
- Pectinate muscles - muscular ridges in the anterior wall and auricle
- Crista terminalis - smooth muscular ridge separating the sinus venarum (smooth posterior part) from the trabeculated anterior part
- Fossa ovalis - oval depression in the interatrial septum; remnant of the fetal foramen ovale
Right Ventricle (RV)
- Receives blood from the RA through the tricuspid (right AV) valve
- Pumps blood into the pulmonary trunk via the pulmonary valve
- Internal features: trabeculae carneae (muscular ridges), papillary muscles (3: anterior, posterior, septal), chordae tendineae, and the moderator band (septomarginal trabecula) carrying right bundle branch fibers
- The outflow tract is called the conus arteriosus (infundibulum)
Left Atrium (LA)
- Receives oxygenated blood from the 4 pulmonary veins (2 right, 2 left)
- Has pectinate muscles confined to the left auricle
- Walls are slightly thicker than the RA
Left Ventricle (LV)
- Receives blood from the LA through the mitral (bicuspid/left AV) valve
- Pumps oxygenated blood into the aorta via the aortic valve
- Wall is approximately 3x thicker than the RV wall (reflecting higher systemic pressure demands)
- Internal features: trabeculae carneae, 2 papillary muscles (anterior and posterior), chordae tendineae
- No moderator band
5. Cardiac Valves
Atrioventricular (AV) Valves
These prevent backflow from ventricles into atria during systole. Their cusps are anchored to fibrous rings at the AV orifices, and their free margins attach to chordae tendineae arising from papillary muscles. The papillary muscles contract simultaneously with the ventricle, maintaining cusp tension and preventing eversion (prolapse) into the atria.
| Valve | Location | Cusps | Papillary muscles |
|---|---|---|---|
| Tricuspid (right AV) | Right AV orifice | 3: anterior, septal, posterior | 3 |
| Mitral/Bicuspid (left AV) | Left AV orifice | 2: anterior, posterior | 2 |
Semilunar Valves
These prevent backflow from great arteries into ventricles during diastole.
| Valve | Location | Cusps |
|---|---|---|
| Pulmonary | Opening into pulmonary trunk | 3 semilunar: left, right, anterior |
| Aortic | Opening into aorta | 3 semilunar: left, right, posterior |
Each semilunar cusp has a nodule (thickened center) and lunulae (thin lateral edges). Sinuses behind each cusp fill with blood during diastole, forcing the cusps closed. The left and right aortic sinuses (sinuses of Valsalva) are the origin sites of the left and right coronary arteries.
Clinical note: Necrosis of a papillary muscle following myocardial infarction can cause valve prolapse and acute regurgitation. - Gray's Anatomy for Students, p. 233
6. The Pericardium
The pericardium is a double-walled fibroserous sac enclosing the heart:
- Fibrous pericardium - tough outer layer; fused with the central tendon of the diaphragm inferiorly and continuous with the tunica adventitia of the great vessels superiorly
- Serous pericardium - two layers:
- Parietal layer - lines the inner surface of the fibrous pericardium
- Visceral layer (epicardium) - directly covers the heart surface
The pericardial cavity between the two serous layers contains a thin film of serous fluid (~10-50 mL), which reduces friction during cardiac motion.
Key recesses:
- Transverse sinus - posterior to the ascending aorta and pulmonary trunk, anterior to the superior pulmonary veins
- Oblique sinus - a blind recess behind the left atrium
7. Coronary Circulation
The heart receives its own blood supply exclusively from the right and left coronary arteries, which arise from the aortic sinuses (sinuses of Valsalva) immediately above the aortic valve.
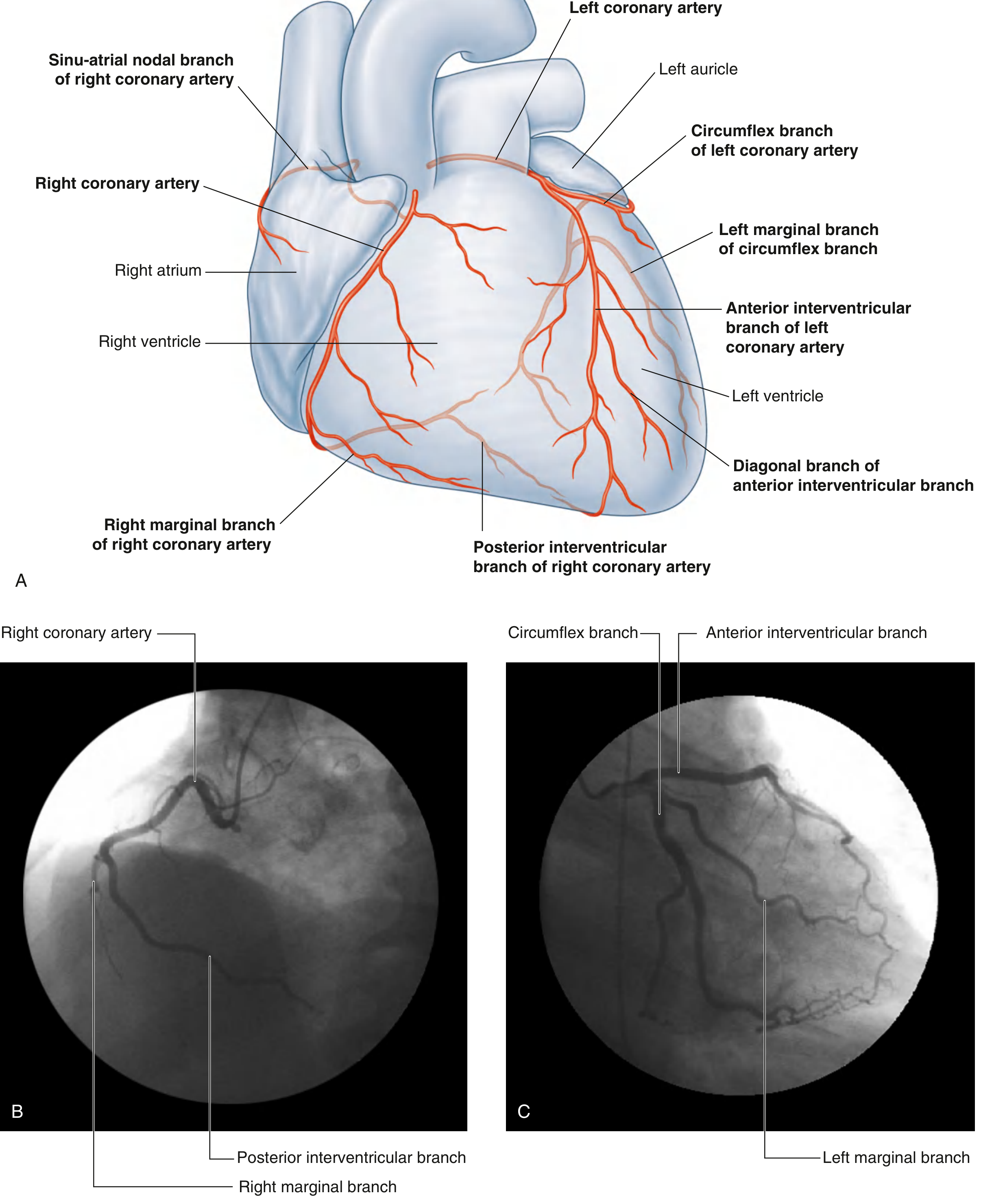
Right Coronary Artery (RCA)
- Arises from the right aortic sinus
- Travels in the right coronary sulcus (atrioventricular groove)
- Key branches:
- Sinu-atrial (SA) nodal branch - supplies SA node (in ~60% of people)
- Right marginal branch - supplies the right ventricular margin
- Posterior interventricular branch (= posterior descending artery, PDA) - runs in the posterior interventricular groove; supplies the posterior 1/3 of the interventricular septum and inferior LV wall
Left Coronary Artery (LCA)
- Arises from the left aortic sinus; the short trunk is the "left main stem"
- Divides into:
- Anterior interventricular branch (= left anterior descending, LAD) - runs in the anterior interventricular groove; supplies anterior 2/3 of the interventricular septum, anterior LV wall, and apex; most clinically important vessel
- Circumflex branch - travels in the left coronary sulcus; supplies the left atrium and posterior/lateral LV wall; gives a left marginal branch
Coronary Dominance
- Right dominant (~70% of people): RCA gives the posterior interventricular branch and supplies the AV node
- Left dominant (~15%): the circumflex branch provides the posterior interventricular branch
- Co-dominant (~15%): both arteries contribute
Gray's Anatomy for Students, p. 241-242
Cardiac Veins
- Great cardiac vein - accompanies the LAD in the anterior interventricular groove, then travels in the left coronary sulcus to become the coronary sinus
- Middle cardiac vein - accompanies the posterior interventricular artery
- Small cardiac vein - accompanies the right marginal artery
- Coronary sinus - the main venous collector; drains into the right atrium between the IVC orifice and the tricuspid valve
- A small amount of blood also drains directly into the chambers via the anterior cardiac veins and Thebesian veins
8. Cardiac Skeleton (Fibrous Skeleton)
Four fibrous rings (anuli fibrosi) surround the four cardiac valves and are interconnected by fibrous tissue, forming the cardiac skeleton. Functions:
- Provide attachment for valve cusps
- Provide attachment for atrial and ventricular musculature
- Act as electrical insulation between the atria and ventricles (forcing conduction to pass only through the AV node and His bundle)
9. Conducting System
The specialized conducting tissue initiates and coordinates the heartbeat:
| Component | Location | Function |
|---|---|---|
| SA node | Junction of SVC and right atrium (crista terminalis) | Primary pacemaker (~60-100 bpm) |
| AV node | Interatrial septum (Koch's triangle) | Delays impulse (~0.1 sec); backup pacemaker (~40-60 bpm) |
| Bundle of His | Upper interventricular septum | Conducts impulse from AV node |
| Right bundle branch | Right side of IV septum | To right ventricle |
| Left bundle branch | Left side of IV septum; divides into anterior and posterior fascicles | To left ventricle |
| Purkinje fibers | Subendocardium of both ventricles | Rapid spread to ventricular myocardium |
Blood supply to the SA and AV nodes is typically from the RCA (in most individuals).
10. Dual Circulation
The cardiovascular system operates as two circuits in series:
| Circuit | Path | Pump |
|---|---|---|
| Pulmonary (right heart) | RV → pulmonary trunk → lungs → pulmonary veins → LA | Right ventricle |
| Systemic (left heart) | LV → aorta → systemic tissues → SVC/IVC → RA | Left ventricle |
This dual-circuit arrangement is why the LV wall is thicker - it must generate enough pressure (~120 mmHg systolic) to perfuse the entire body, compared to ~25 mmHg generated by the RV for the pulmonary circuit.
11. Key Clinical Correlations
| Clinical Concept | Anatomical Basis |
|---|---|
| Apex beat (5th left ICS, MCL) | LV forms the cardiac apex |
| Heart attack (MI) | LAD occlusion most common ("widow maker"); posterior MI = RCA |
| Valve prolapse post-MI | Papillary muscle infarction disrupts chordae tendineae support |
| Tamponade | Pericardial fluid compresses cardiac chambers |
| Patent foramen ovale | Failed closure of the fossa ovalis (~25% of adults) |
| Coronary angioplasty (PCI) | Catheter via femoral → iliac → aorta → coronary ostium |
| Right border widening on CXR | RA enlargement (e.g., right heart failure, ASD) |
| Aortic dissection | Tear in aortic intima, blood enters tunica media |
This covers the cardiovascular system anatomy comprehensively - from vessel microstructure through cardiac chambers, valves, pericardium, coronary supply, conduction system, and dual circulation. Let me know if you want to go deeper into any specific area (e.g., embryological development, detailed valve anatomy, coronary artery territories, or the mediastinal relations of the great vessels).
This is a shared conversation. Sign in to Orris to start your own chat.