Molecular genetics testing in THYROid cancers
"thyroid cancer"[MeSH Terms] AND "molecular testing" AND "genetic markers"
"thyroid neoplasms"[MeSH Terms] AND "molecular diagnostic techniques"[MeSH Terms]
"thyroid nodule" AND "molecular testing" AND "indeterminate cytology"
PMID: 42118459
Molecular Genetics Testing in Thyroid Cancers
Overview
Key Molecular Alterations by Tumor Type
1. Papillary Thyroid Carcinoma (PTC)
| Alteration | Frequency | Notes |
|---|---|---|
| BRAF V600E | ~45% | Most common; T1799A transversion in exon 15 |
| RAS mutations | 10-30% | HRAS, KRAS, NRAS (codon 61 most common) |
| RET/PTC rearrangements | 20% (adults); higher in children | RET/PTC1 and RET/PTC3 most common (>10 types total) |
| NTRK1 rearrangements | 5-13% | Fusions with heterologous sequences |
| AKAP9-BRAF | Rare | Associated with radiation exposure |
- The T1799A transversion causes valine-to-glutamic acid substitution at codon 600 (V600E), constitutively activating BRAF kinase and downstream MEK-ERK signaling
- Correlates with aggressive features: extrathyroid extension, advanced stage, lymph node involvement, distant metastases, and radioiodine resistance
- Also present in 20-40% of poorly differentiated and 30-44% of anaplastic thyroid carcinomas - suggesting it is an early event predisposing to dedifferentiation
- Detection methods: direct sequencing, real-time PCR, allele-specific SYBR green PCR, or colorimetric assays on FNA specimens
- Specificity >95% for PTC when detected
-
Result from chromosomal rearrangements fusing the tyrosine kinase domain of RET (not normally expressed in follicular cells) with heterologous genes
-
Strongly associated with radiation exposure (Chernobyl: 66% of post-disaster PTCs had RET/PTC1 or RET/PTC3)
-
RET/PTC3 - solid follicular variant; RET/PTC1 - classic/diffuse sclerosing variant
-
Since these mutations are mutually exclusive with BRAF and RAS, presence of any one virtually confirms PTC
-
Cummings Otolaryngology, p. 2370; Robbins Basic Pathology, p. 736-737
2. Follicular Thyroid Carcinoma (FTC)
| Alteration | Frequency | Notes |
|---|---|---|
| RAS mutations | 40-50% | Codon 61 of NRAS/HRAS (not codon 12 as in most cancers) |
| PAX8-PPARG rearrangement | 35-60% | t(2;3)(q13;p25) translocation |
| PIK3CA mutations | Rare-20% | Gain-of-function; also in ATC |
| PTEN loss-of-function | Variable | Seen in Cowden syndrome (germline) and sporadic FTC |
- Results from translocation t(2;3)(q13;p25), fusing the thyroid-specific paired domain transcription factor PAX8 with the nuclear hormone receptor PPARG
- Occurs in 35-60% of conventional FTC and follicular variant of PTC
- Also in ~13% of follicular adenomas and ~5% of follicular variant PTC
- Inhibits PPARG tumor suppressor activity while transactivating PAX8-responsive genes
- These tumors tend to be smaller, appear in younger patients, and show solid/nested patterns with more frequent vascular invasion
- PPARG protein overexpression is detectable by immunohistochemistry
-
Unlike most cancers where RAS mutations occur at codon 12, thyroid FTC favors codon 61 of NRAS and HRAS
-
Associated with tumor dedifferentiation, worse prognosis, and bone metastasis
-
Also found in 20-40% of poorly differentiated carcinomas, reflecting a shared histogenesis with FTC
-
Henry's Clinical Diagnosis, p. 1833; Robbins Basic Pathology, p. 736
3. Anaplastic Thyroid Carcinoma (ATC)
| Alteration | Frequency | Notes |
|---|---|---|
| TP53 mutations | 60-80% | Loss-of-function; most characteristic; rare in well-differentiated forms |
| BRAF V600E | ~44% | Shared with PTC (de-differentiation pathway) |
| RAS mutations | 20-60% | Shared with FTC (de-differentiation) |
| PIK3CA mutations | ~20% | Gain-of-function |
- Robbins Basic Pathology, p. 737; Cummings Otolaryngology, Table 122.1
4. Medullary Thyroid Carcinoma (MTC)
| Alteration | Frequency | Context |
|---|---|---|
| RET germline mutation | ~95-100% of hereditary MTC | Familial MTC, MEN2A, MEN2B |
| RET somatic mutation | ~25-50% of sporadic MTC | Often codon M918T (same as MEN2B germline) |
| HRAS/KRAS mutations | Up to 25% | Sporadic MTC, mutually exclusive with RET |
-
RET is on chromosome 10q11.2 and encodes a transmembrane tyrosine kinase receptor
-
Over 100 germline mutations described; codon C634 is the most common
-
The ATA (2015) risk classification for hereditary MTC is based on the specific RET mutation:
- Highest risk: M918T (MEN2B) - thyroidectomy within first months of life
- High risk: C634 and A883F - thyroidectomy by age 5
- Moderate risk: all other mutations - annual surveillance or thyroidectomy
-
All patients with MTC/C-cell hyperplasia should undergo germline RET testing to rule out hereditary disease
-
Somatic RET mutations in sporadic MTC are associated with nodal metastases and higher disease-specific mortality
-
Sabiston Textbook of Surgery, p. 1518
Incidence Summary Table (Cummings Otolaryngology)
| Genetic Alteration | PTC | FTC | PDTC | ATC | MTC |
|---|---|---|---|---|---|
| RET rearrangement | 20% | - | Rare | - | - |
| NTRK1 rearrangement | 5-13% | - | - | - | - |
| RET point mutation | - | - | - | - | Sporadic 30-50%; MEN2 ~95% |
| BRAF mutation | 45% | - | 15% | 44% | - |
| RAS mutation | 10% | 40-50% | 44% | 20-60% | - |
| PIK3CA mutation | Rare | Rare | Rare | 20% | - |
| PPARG rearrangement | - | 35% | Rare | - | - |
| TP53 | Rare | Rare | 15-30% | 60-80% | Rare |
Clinical Applications
A. Preoperative Molecular Testing of Indeterminate FNA (Bethesda III/IV)
| Approach | Examples | Principle |
|---|---|---|
| Rule-in (mutation detection) | ThyroSeq v3, RosettaGX Reveal | High specificity; positive = strong evidence of malignancy |
| Rule-out (gene expression) | Afirma Gene Expression Classifier (GEC), Afirma GSC | High sensitivity/NPV; negative = benign, avoid surgery |
- ThyroSeq v3 (Genomic Classifier): NGS-based panel detecting point mutations (BRAF, RAS, TERT, TP53, PIK3CA), gene fusions (RET/PTC, NTRK, PAX8-PPARG, ALK, THADA), and copy number alterations in 112 genes; also measures gene expression
- Afirma GSC: mRNA expression classifier using 10,196 genes on FNA material; negative result ("benign") avoids surgery in ~50% of indeterminate nodules
- RosettaGX Reveal: microRNA-based classifier
Key meta-analysis (2026): A PRISMA-guided meta-analysis of 132 studies (66,448 nodules) found molecular testing significantly reduced surgical rates compared to conventional management (OR 2.258, 95% CI 1.548-3.293) without evidence of missed clinically significant malignancies. Second-generation assays outperformed first-generation platforms. [PMID: 42118459]
B. Prognostic and Risk Stratification
- BRAF V600E on FNA: independently predicts higher recurrence risk; informs extent of surgery and intensity of postoperative surveillance in PTC
- TERT promoter mutations: when co-occurring with BRAF or RAS, dramatically worsen prognosis in differentiated thyroid cancer; used in individualized patient management via NGS panels
- RET mutation subtype in MTC: drives the timing of prophylactic thyroidectomy in gene carriers
C. Targeted Therapy Selection
| Mutation | Drug(s) | Indication |
|---|---|---|
| BRAF V600E | Dabrafenib + trametinib | ATC (FDA-approved); RAIR PTC |
| RET mutation/fusion | Selpercatinib, pralsetinib | MTC and RET-fusion+ differentiated thyroid cancer |
| NTRK fusion | Larotrectinib, entrectinib | NTRK-positive thyroid cancer |
| RAS / MAPK pathway | Sorafenib, lenvatinib | Differentiated thyroid cancer (multi-kinase inhibitors) |
| RET (MTC) | Vandetanib, cabozantinib | Advanced/metastatic MTC |
D. Hereditary Syndrome Screening
- MEN2A/2B: Germline RET testing is mandatory for all MTC patients and recommended for first-degree relatives
- Cowden syndrome (PTEN): Associated with follicular thyroid tumors; germline PTEN testing indicated when clinical criteria met
- Familial adenomatous polyposis (APC): Associated with cribriform-morular variant of PTC
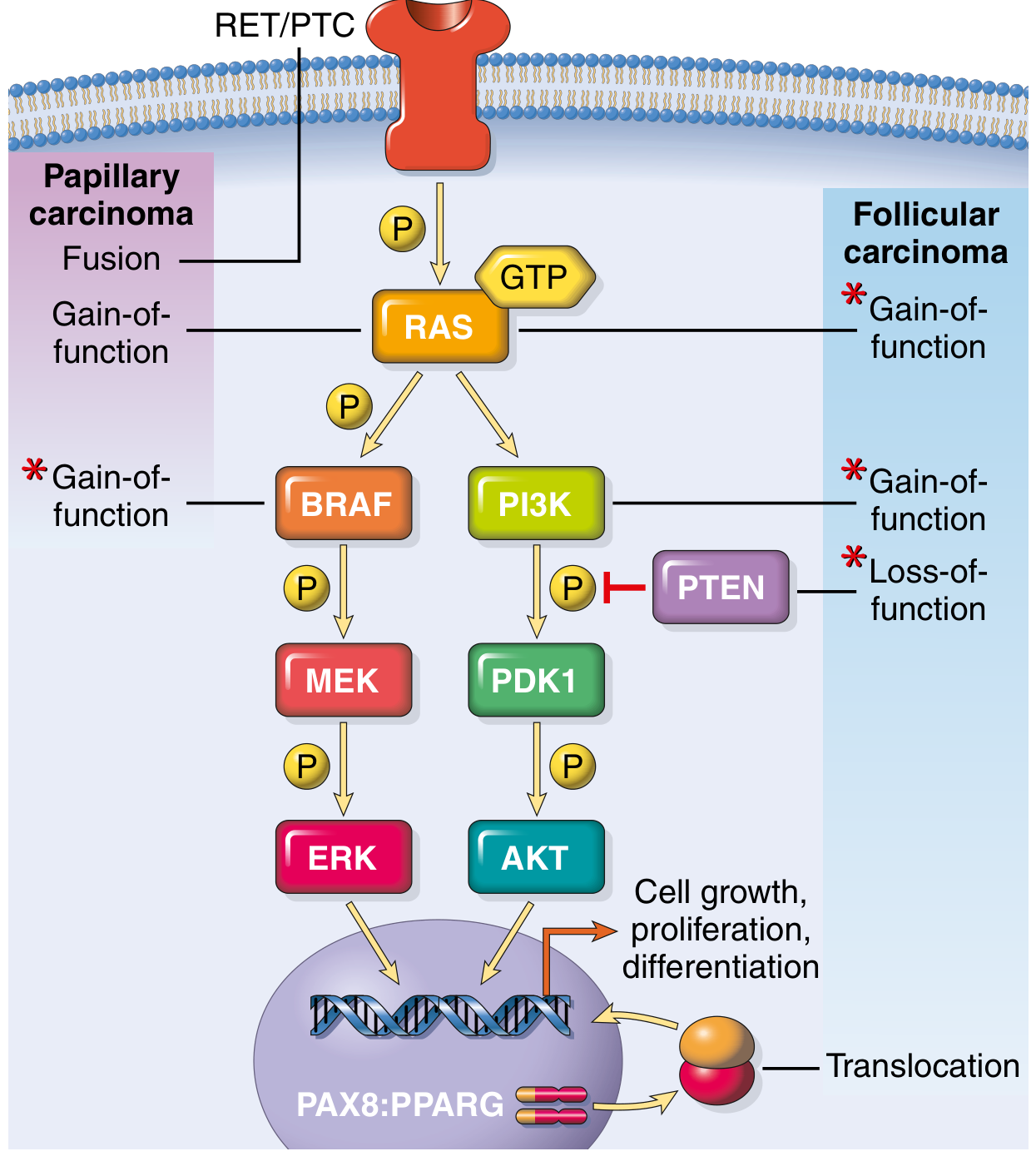
Signaling Pathways Summary
- MAPK pathway (RAS -> RAF -> MEK -> ERK): predominantly activated in PTC via BRAF V600E, RAS mutations, or RET/PTC and NTRK fusions
- PI3K/AKT pathway (RAS -> PI3K -> PDK1 -> AKT): predominantly activated in FTC via RAS mutations, PIK3CA gain-of-function, or PTEN loss-of-function; also important in ATC progression
- These two pathways converge on cell growth, proliferation, and differentiation; the PAX8:PPARG fusion acts as an independent nuclear oncogenic event in FTC
Sources
- Henry's Clinical Diagnosis and Management by Laboratory Methods, pp. 1832-1834
- Robbins & Kumar Basic Pathology, pp. 736-737
- Cummings Otolaryngology Head and Neck Surgery, pp. 2369-2371
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 1, pp. 131-133
- Sabiston Textbook of Surgery, pp. 1517-1518
- Nguyen et al., Endocr Pathol 2026 - [Meta-analysis, 66,448 nodules, PMID: 42118459]
- Ferraz C, Rev Endocr Metab Disord 2024 - [PMID: 37902897]
- Dettmer MS, Virchows Arch 2026 - [PMID: 41242985]
Prevention of open book deformity in Rhinoplasty, double barrel mandible in mandibular reconstruction, CAD/CAM benefits in cosmesis of mandibular reconstruction, genetic testing in medullary ca thyroid,
"open book deformity" rhinoplasty nasal tip prevention
rhinoplasty "open book" nasal tip alar cartilage
"double barrel" fibula mandibular reconstruction flap
CAD CAM virtual surgical planning mandible reconstruction outcomes
rhinoplasty nasal tip "open roof" deformity prevention columellar strut
medullary thyroid carcinoma RET mutation genetic testing guidelines
PMID: 38930078
PMID: 39579327
rhinoplasty "open book" nasal tip prevention techniques
open book deformity rhinoplasty nasal tip prevention techniques surgery
virtual surgical planning CAD CAM mandibular reconstruction cosmesis accuracy
https://www.ncbi.nlm.nih.gov/books/NBK558970
PMID: 38077486
open book deformity rhinoplasty columellar strut shield graft prevention tip alar cartilage splaying
medullary thyroid cancer germline RET somatic testing recommendations 2024
1. Prevention of Open Book Deformity in Rhinoplasty
What Is It?
Why It Happens
- The interdomal ligament connecting the two domes
- The scroll ligament attaching upper and lower lateral cartilages
- Intact caudal septum as a central support
- Preserved lower lateral cartilage strip width (complete strip)
Prevention Strategies
1. Columellar Strut Graft (most important)
- Holds the two medial crura together, preventing lateral splaying
- Resists downward tension and displacement
- Splints the columella
- Must not extend to the anterior nasal spine (causes clicking as it slips over bone)
- Material preference: septal cartilage (ideal, no warping); rib cartilage as alternative; ear cartilage too soft for base stabilization
2. Interdomal Suture (Tip-Unifying Suture)
3. Transdomal Sutures
4. Preserve the Complete Strip (Cephalic Trim Discipline)
- Always leave a minimum 6-8 mm complete strip of the lower lateral cartilage
- Avoid discontinuous (non-complete-strip) resections, which eliminate cartilage spring and promote alar buckling
- A strip narrower than 5 mm is at high risk of structural collapse
5. Tip Support Reconstitution after Open Approach
- Columellar strut graft placement
- Interdomal sutures
- Medial crural suture to caudal septum (tongue-in-groove or septal extension graft)
6. Septal Extension Graft / Caudal Extension Graft
7. Lateral Crural Strut Grafts
8. Alar Rim Grafts
Summary Table
| Technique | Mechanism of Prevention |
|---|---|
| Columellar strut graft | Unifies medial crura; maintains base stability |
| Interdomal suture | Directly closes dome separation |
| Transdomal sutures | Refines and narrows each dome |
| Complete strip preservation (≥6mm) | Maintains lateral crura spring |
| Septal extension graft | Strong base stabilization, tip projection control |
| Lateral crural strut | Prevents alar bowing/buckling |
| Alar rim grafts | Prevents alar margin collapse |
2. Double-Barrel Fibula Flap in Mandibular Reconstruction
Concept
Technique
- Single fibula flap harvested as usual, with its peroneal vascular pedicle
- The fibula is osteotomized into multiple segments
- One segment is folded/stacked 180° on top of another, secured with mini-plates or screws - creating approximately 24-28 mm of bone height, mimicking the native alveolar + basal bone height of the mandible
- The stacked configuration is secured to the reconstruction plate and anastomosed as a single flap (one vascular pedicle serves both layers via intact periosteum)
- A skin paddle can be used simultaneously for intraoral lining (chimeric LSMAP - latissimus dorsi, serratus anterior, muscle, adipose, peroneal) to cover the plate and provide soft tissue
Why Double-Barrel Improves Cosmesis
Facial Contour Restoration
- Taller bone height more closely approximates the native mandibular height from basal bone to alveolar crest
- Prevents the "sunken" lower face appearance that results from insufficient bone height with a single fibula
- The reconstructed mandible projects the overlying skin and soft tissue appropriately, restoring jawline contour
Dental Rehabilitation (Crucial for Cosmesis)
- Single-barrel fibula: typically 12-14 mm bone height, often insufficient for implant placement without extensive bone grafting
- Double-barrel fibula: ~24-28 mm, adequate implant depth (≥10 mm needed), positioned in the alveolar plane
- Implant-supported prostheses restore dental arch, lip support, vermilion show, and facial width - all cosmetically critical
Systematic Review Evidence (2024)
- Flap survival: 98.3% success
- Dental implant failure rate: only 1.74%
- Aesthetic outcomes were positive though inconsistently assessed
- DBFF is a viable, safe alternative for combined bony and dental reconstruction [PMID: 38930078]
Considerations / Limitations
| Advantage | Limitation |
|---|---|
| Greater bone height for implants | More complex dissection |
| Better facial contour restoration | Requires careful periosteal preservation for dual perfusion |
| Single vascular pedicle | Risk of partial segment devascularization |
| One-stage jaw and dental rehabilitation possible | Segments <2 cm risk devascularization |
| High flap survival (98.3%) | Aesthetic evidence still of low certainty |
3. CAD/CAM Benefits in Cosmesis of Mandibular Reconstruction
What Is CAD/CAM in This Context?
- High-resolution maxillofacial CT scan of the patient
- Digital 3D reconstruction of the mandible and donor site (usually fibula)
- Virtual surgery: tumor resection and reconstruction are simulated on the computer
- Fabrication of patient-specific cutting guides, positioning guides, and reconstruction plates via additive manufacturing (3D printing)
- Transfer of the virtual plan to the operating room via custom surgical tools
Specific Cosmetic Benefits
1. Accurate 3D Spatial Reconstruction
- Chin projection (the mental protuberance can be 2 cm anterior to the occlusal plane - often over-reduced in freehand surgery)
- Mandibular arch width and symmetry
- Temporomandibular joint spatial relationships
2. Facial Contour Precision
- Pre-bent or 3D-printed custom titanium reconstruction plates match the patient's exact anatomy
- Eliminates the distortion from intraoperative plate-bending, which can cause subtle lower facial asymmetry
- Custom plates can incorporate both lower border contour and occlusal plane alignment simultaneously
3. Improved Dental Rehabilitation (Occlusion-Driven Workflow)
- The alveolar bone plane sits medial to the basal bone - these do not overlap
- VSP allows the reconstruction to be planned from the occlusal plane downward
- Result: osseointegrated implants are placed in the correct position for prosthetic rehabilitation
- Restoring complete dental arch = restoration of lip support, cheek fullness, and lower facial projection
4. Reduced Operative Time and Ischemia Time
- Pre-cut fibula cutting guides allow the fibula segments to be prepared rapidly and accurately
- Reduced flap ischemia time correlates with higher flap viability - preserved tissue vascularity benefits long-term soft tissue drape and contour
- Studies report reduced total operative time with SDS vs. freehand
5. Superior Teaching and Planning Tool
- SDS significantly enhances understanding of 3D defect and challenges before the patient is in the OR
- Fewer intraoperative surprises = fewer compromises in reconstruction
Advantages Summary (Cummings Otolaryngology Box 92.1)
- Better understanding of mandibular pathology in three dimensions
- Accurate mandibular reconstruction
- Reduced flap ischemia and operative time
- Improved potential for dental implantation and occlusal reconstruction
Limitations
- Cost: VSP adds cost; debated whether cost-effective (though some studies show net savings from reduced OR time and implant waste)
- Planning-surgery time lag: tumor may progress between VSP and surgery date, making cutting guides less applicable - particularly in oncologic cases where margin revision is common
- Availability: not universally accessible, though commercial platforms (e.g., DePuy Synthes ProPlan, Stryker) are now widely available
- Cannot fully account for intraoperative variability in resection margins
"SDS-assisted reconstructions have the advantage of decreasing operative and ischemia time as well as providing superior outcomes in terms of maintaining and restoring 3D spatial relationships of the reconstruction, which are valuable in oral rehabilitation where reestablishing dental occlusion with osseointegrated implants is considered." - Cummings Otolaryngology, p. 1688
- Probst et al., Innov Surg Sci 2023 [PMID: 38077486]
4. Genetic Testing in Medullary Thyroid Carcinoma
Background
Who Should Be Tested - Universal Germline RET Testing
- A significant proportion of "apparently sporadic" MTC are actually the first manifestation of a hereditary syndrome
- Early identification of germline carriers allows prophylactic thyroidectomy in at-risk family members before malignancy develops
- Germline RET mutation subtype determines the aggressiveness and timing of intervention (ATA risk classification)
What Is Tested
A. Germline Testing (Constitutional / Blood DNA)
| Scenario | Recommendation |
|---|---|
| All newly diagnosed MTC patients | Germline RET sequencing |
| First-degree relatives of RET mutation carriers | Germline RET sequencing |
| MEN2 syndrome evaluation | Full RET sequencing including codons 609, 611, 618, 620, 630, 634, 768, 790, 791, 804, 883, 918 |
| Hirschsprung disease + MTC family history | RET testing (loss-of-function vs. gain-of-function mutations) |
B. ATA Risk Classification Based on RET Mutation Subtype
| ATA Risk Category | Key Mutations | Thyroidectomy Timing | Aggressiveness |
|---|---|---|---|
| Highest (ATA-HST) | Codon M918T (MEN2B) | Within first months of life | Macroscopic MTC + nodal mets possible within 1st year |
| High (ATA-H) | Codon C634, A883F | By age 5 (or sooner if calcitonin elevated) | Aggressive; pheochromocytoma + hyperparathyroidism risk |
| Moderate (ATA-MOD) | All other mutations | Annual surveillance or thyroidectomy (individualized) | Slower growing |
C. Somatic Testing (Tumor DNA from Resected Specimen)
- Confirming sporadic nature
- Identifying somatic RET mutations (~25-50% of sporadic MTC), especially codon M918T - these tumors have higher nodal metastasis rates, persistent disease, and disease-specific mortality, warranting more aggressive surveillance
- Guiding targeted therapy selection:
- Selpercatinib (RET-specific inhibitor) - first-line in RET-mutant advanced/metastatic MTC
- Pralsetinib - RET-selective inhibitor
- Older multikinase inhibitors (vandetanib, cabozantinib) inhibit RET but with off-target toxicity
D. Additional Somatic Biomarkers in Advanced/Metastatic MTC
- RAS mutations (HRAS, KRAS - up to 25% of sporadic MTC) - mutually exclusive with RET; guide MEK/MAPK-targeted approaches
- Calcitonin and CEA doubling times - still key prognostic biomarkers
- Comprehensive next-generation sequencing (NGS) panels now preferred for tissue to capture RET mutations/fusions + RAS in a single assay
E. Family Member Screening Protocol
- Offer genetic testing to all first-degree relatives
- Test children as early as clinically indicated (timing based on ATA risk category)
- Mutation-positive relatives undergo total thyroidectomy at recommended age
- Mutation-negative relatives can be discharged from intensive MTC surveillance
Emerging Evidence (2026)
Sources
- Sabiston Textbook of Surgery 8th ed., pp. 1517-1518 (RET and MTC)
- Cummings Otolaryngology Head and Neck Surgery, pp. 1687-1691 (Mandibular reconstruction, SDS/VSP, CAD/CAM)
- Creasy & Resnik's Maternal-Fetal Medicine (MTC/MEN2)
- StatPearls: Rhinoplasty, Rhinoplasty Tip-Shaping Surgery (NBK558970, NBK567750)
- Khayat et al., J Clin Med 2024 - [Systematic Review, Double-barrel fibula, PMID: 38930078]
- Probst et al., Innov Surg Sci 2023 - [VSP/CAD-CAM review, PMID: 38077486]
- Mete et al., Endocr Pathol 2024 - [Consensus: Biomarker testing in thyroid cancer, PMID: 39579327]
- Onuma et al., Surgery 2026 - [Germline RET panel testing landscape, PMID: 41371824]