Vertical root fractures
Reading File
Finding Sources
Searching PubMed
"vertical root fracture" diagnosis treatment
Finding Sources
Reading Article
Reading Article
Finding Sources
Finding Sources
Searching the Web
vertical root fractures VRF etiology diagnosis management endodontics 2024
Finding Sources
Reading Web Page
vertical root fracture etiology diagnosis classification management treatment
I now have enough high-quality information to provide a comprehensive answer on vertical root fractures.
Vertical Root Fractures (VRFs)
Definition
A vertical root fracture (VRF) is a longitudinal fracture that begins on the internal canal wall and extends outward to the external root surface, running along the long axis of the tooth. The fracture may be partial or complete and can extend coronally from the apex in an oblique or longitudinal direction.
Epidemiology
- Incidence among root-canal-treated teeth: 4% to 32%
- 80% of VRFs are detected within 2 years after onset of initial symptoms
- Most common in posterior teeth (premolars > molars), especially maxillary premolars and mandibular molars
- Often diagnosed late due to nonspecific presentation, resulting in unnecessary treatments and progressive bone loss
Classification
VRFs can be classified by:
| Parameter | Types |
|---|---|
| Trajectory | Vertical, transverse, oblique |
| Extent | Complete (total separation) or incomplete (partial crack) |
| Location | Apical, mid-root, cervical |
| Origin | Internal canal wall extending outward (most common in endodontically treated teeth) |
Etiology and Risk Factors
VRFs are almost always iatrogenic in endodontically treated teeth. Key contributors:
Endodontic factors:
- Excessive removal of healthy dentin during root canal preparation (over-instrumentation)
- Prolonged contact with intracanal disinfectants and medicaments (e.g., NaOCl, Ca(OH)2) - alters dentin mechanical properties
- Aggressive lateral or vertical condensation of gutta-percha during obturation (excessive hydraulic pressure)
- Overly large preparation (thin dentinal walls)
Post-endodontic/restorative factors:
- Improper post selection (rigid posts in curved roots, oversized posts)
- Excessive force during post preparation (widening the canal excessively)
- Improper post cementation or expansion forces
Tooth/patient factors:
- Advanced patient age (dentin becomes more brittle)
- Type of tooth (maxillary premolars particularly vulnerable due to thin roots)
- Pre-existing dentinal cracks
- Heavy occlusal loading, bruxism
- Reduced moisture content of endodontically treated dentin (more brittle)
Pathogenesis
When a VRF occurs (complete or incomplete), it extends to the periodontal ligament. Soft tissue grows into the fracture space, increasing separation of root segments. On communication with the oral cavity through the gingival sulcus, a foreign-body inflammatory reaction develops. This leads to:
- Destruction of the surrounding alveolar bone
- Progressive periodontal breakdown
- Potential compromising of future implant placement if extraction is delayed
Clinical Features
VRFs are notoriously difficult to diagnose because their signs and symptoms mimic both endodontic failure and periodontal disease.
Signs and Symptoms:
| Feature | Description |
|---|---|
| Sinus tract / parulis | Present near the mid-root or cervical region (not just at the apex) |
| Deep, narrow periodontal pocket | Localized, isolated ("halo" or "J-shaped" pattern on X-ray) |
| Tenderness to percussion | Lateral percussion often positive |
| Swelling / abscess | Localized gingival or facial swelling |
| Gingival recession | On the affected side of the root |
| Symptoms often vague | Mild, intermittent discomfort; can be asymptomatic |
The "classic triad":
- Narrow isolated periodontal pocket
- Sinus tract at the fracture site
- History of root canal treatment
Diagnosis
Diagnosis is challenging and requires combining multiple modalities.
Clinical Examination
- Probing depths - look for narrow, deep, isolated pockets ("halo" pattern)
- Transillumination - may reveal fracture lines
- Staining with methylene blue or iodine - helps detect fracture lines intraorally or during surgery
- Exploratory surgery - the gold standard for definitive diagnosis
Radiographic Examination
Periapical X-ray:
- Limited: 2D nature creates anatomical noise and distortion
- Signs: J-shaped radiolucency alongside the root, apical and lateral bone loss, angular bone defects
- Fracture line is often NOT visible
Cone-Beam Computed Tomography (CBCT):
- Superior to periapical X-ray - provides 3D imaging with reduced noise
- Signs: "Halo" sign, presence of the fracture line, bone loss pattern
- Best available non-invasive diagnostic tool
- Can detect fractures missed on conventional radiographs
Radiographic patterns suggestive of VRF:
- Periapical bone loss + lateral bone loss together
- Diffuse lateral widening of the periodontal ligament space
- Alveolar bone loss along the full length of the root
Differential Diagnosis
VRFs must be distinguished from:
- Endodontic failure / persistent apical periodontitis - but typically associated with technical failures, no narrow pocket
- Primary/secondary periodontal disease - generalized pattern, multiple teeth
- Cemental tear - a separate condition that also causes localized bone loss and may mimic VRF; can coexist
- Perforations - from iatrogenic root perforations
- Cracked tooth syndrome - affects coronal dentin, pain on biting, not longitudinal to root
Management
The management of VRFs is guided by fracture extent, tooth condition, periodontal status, and patient preference.
1. Extraction (Traditional and Most Common)
- Standard treatment for complete VRF
- Early extraction is recommended to minimize progressive bone destruction that may compromise future implant placement
- Followed by implant rehabilitation or prosthetic replacement
2. Conservative / Tooth-Preserving Approaches
Intentional Replantation:
- Tooth is extracted, fracture surfaces are bonded/sealed extra-orally, then the tooth is replanted
- Success depends on careful handling, minimal extra-oral time, and intact periodontal status
- Variable long-term outcomes; best for single-rooted teeth with accessible fractures
Adhesive / Bonding Techniques:
- Fracture segments bonded with materials such as SuperEBA cement, MTA (Mineral Trioxide Aggregate), or adhesive resins
- Can be done via intentional replantation or surgical access
Regenerative Procedures:
- Guided tissue regeneration to address bone loss
- Experimental and limited evidence
Root Resection / Hemisection:
- For multi-rooted teeth: removal of the affected root while preserving the rest of the tooth
- Mandibular molars are best candidates
Surgical Exploration + Bonding:
- Mucoperiosteal flap reflection to access the fracture
- Bonding under direct vision with MTA or similar materials
Key Decision Factors for Treatment:
- Periodontal status - intact bone = better prognosis for preservation
- Extent and location - incomplete vs. complete; apical vs. cervical
- Tooth type - single-rooted vs. multi-rooted
- Fragment condition - viability of root segments
- Clinician skill and patient consent
Prevention (Best Approach)
- Avoid over-instrumentation during root canal preparation
- Use appropriate canal shaping instruments and techniques (minimize dentin removal)
- Avoid excessive condensation pressures during obturation
- Select post type and size appropriately (prefer fiber posts over rigid metallic posts)
- Use proper cementation technique for posts
- Early identification of susceptible teeth and roots (thin roots, narrow canals)
Prognosis
- Complete VRFs in endodontically treated teeth carry a poor prognosis for tooth retention
- Extraction rates remain high overall
- Tooth-preserving techniques (intentional replantation, adhesive bonding) show variable short-term success but lack strong long-term evidence
- A 2025 systematic review (Corbella et al., Aust Endod J 2025) evaluated surgical techniques for confirmed VRFs, reflecting continued investigation into preservation options
- The 2025 ESE Position Statement (PMID 39840523) provides current evidence-based guidance on longitudinal cracks and fractures including VRFs
- A 2024 review by Salihu & Stavileci (PMID 38402413) emphasizes that standardized protocols and further long-term research are still needed
Summary Table
| Aspect | Key Points |
|---|---|
| Definition | Longitudinal fracture along the root's long axis |
| Most common in | Endodontically treated teeth (4-32% incidence) |
| Main causes | Over-instrumentation, gutta-percha condensation, improper posts |
| Classic signs | Isolated narrow pocket, sinus tract, history of RCT |
| Best imaging | CBCT > periapical X-ray |
| Gold standard diagnosis | Exploratory surgery |
| Treatment | Extraction (most common); preservation possible in select cases |
| Prevention | Conservative endodontic technique, appropriate post selection |
Butterfly effect of vertical root fracture ??
Finding Sources
Searching the Web
butterfly effect vertical root fracture radiographic sign bone loss pattern
Searching PubMed
"vertical root fracture" butterfly radiographic sign bone loss
Reading Web Page
butterfly effect bone loss pattern vertical root fracture buccal lingual bilateral
Searching the Web
"butterfly" "vertical root fracture" buccal lingual bone loss bilateral pattern radiograph
Now I have comprehensive data to give a precise and well-sourced answer. The "butterfly effect" in VRF is specifically about the bilateral bone resorption pattern seen on both buccal and lingual/palatal surfaces.
The "Butterfly Effect" in Vertical Root Fractures
What It Is
The butterfly effect (also called the butterfly pattern or butterfly sign) in VRF refers to the characteristic bilateral bone resorption that occurs on both the buccal AND lingual/palatal surfaces simultaneously around a vertically fractured root. When viewed from above (axial plane - as on CBCT) or conceptualized surgically, the two opposing crescent-shaped bone defects flanking the root resemble butterfly wings on either side.
Why It Happens - The Mechanism
VRFs typically propagate in a bucco-lingual direction (along the plane connecting the buccal and lingual surfaces). This is because:
- The fracture line runs along the long axis of the root in the bucco-lingual plane
- The inflammatory response and bacterial penetration follow the fracture line outward to the periodontal ligament
- Bone resorption begins facing the fracture - i.e., on both the buccal and lingual sides simultaneously
- This creates two opposing bone defects, one on each side of the root
The Two Wings - Different Shapes (Lustig et al., 2000)
The classic study by Lustig et al. on 110 VRF cases revealed that buccal and lingual resorption have distinctly different shapes, which together form the butterfly:
| Side | Pattern | Shape | Reason |
|---|---|---|---|
| Buccal | Dehiscence (V-shaped, oblong triangle) | Narrow, deep, rapid | Thin cortical plate - resorbs quickly in apicocoronal direction, propagates diagonally |
| Lingual/Palatal | U-shaped, shallow, rounded | Wider, slower | Thicker cortex + spongeous bone creates a "shield phenomenon" - spongeous bone resorbs first, then lateral spread |
The buccal wing is sharper and deeper (like a V); the lingual wing is rounder and shallower (like a U). Together, they form the bilateral butterfly outline around the root.
Key Findings from Lustig et al. (2000) Study
- 91% of VRF cases showed the V-shaped dehiscence (buccal)
- 9% showed fenestration of the buccal plate
- Lingual resorption was present in additional cases but was always less severe than buccal
- Strong positive correlation (p < 0.0001) between type/duration of symptoms and amount of buccal bone resorption
- The resorptive defect always faced the fracture line
Clinical Significance
1. Surgical Diagnosis
When a mucoperiosteal flap is reflected during exploratory surgery, seeing the bilateral osseous defects (buccal V + lingual U) on either side of the root is strongly diagnostic of VRF - this is the butterfly pattern in its most direct form.
2. CBCT Diagnosis
On axial (cross-sectional) CBCT slices, the butterfly pattern becomes visible as:
- Bone loss on both the buccal and palatal/lingual sides of the root
- Two crescentic radiolucent areas flanking the root symmetrically or asymmetrically
- When both buccal and palatal bone loss are present on CBCT in an endodontically treated tooth, VRF is strongly suspected
3. Probing Pattern
Clinically, when deep probing defects are found on BOTH the facial and lingual aspects of the same root, this is considered highly suggestive of VRF (the American Association of Endodontists guidelines recognize this as near-pathognomonic when combined with a sinus tract).
4. Sinus Tracts
The butterfly pattern can manifest as sinus tracts on both buccal AND lingual surfaces of the same tooth simultaneously - a finding virtually unique to VRF. Any other etiology almost never produces bilateral sinus tracts.
Comparison with Other Bone Loss Patterns in VRF
| Radiographic/Clinical Pattern | Description |
|---|---|
| Halo sign | 360° periradicular radiolucency surrounding the root (periapical + lateral) |
| J-shaped radiolucency | Periapical + lateral bone loss on one side only |
| Butterfly pattern | Bilateral buccal + lingual bone loss (the wings) |
| Fenestration | Isolated window defect through the buccal plate |
| Widened PDL space | Early sign along the lateral root surface |
Why Radiographic Detection Is Difficult
Because VRF fractures propagate bucco-lingually, the bone resorption is on the buccal and lingual surfaces - these are superimposed over the root on a standard periapical X-ray (which is a 2D projection). The butterfly wings are essentially hidden "behind" the root image. This is why:
- Standard periapical X-rays miss the butterfly pattern
- Only when resorption extends interproximally does it become visible on 2D X-ray
- CBCT is essential to visualize this bilateral butterfly pattern as it provides true cross-sectional (axial) views
Summary
The "butterfly effect" in VRF = bilateral, opposing bone resorption on both the buccal (V-shaped/sharp) and lingual (U-shaped/rounded) surfaces of a fractured root. It reflects the bucco-lingual propagation of the fracture line and the differential cortical bone thickness on each side. It is best seen on CBCT axial slices or during exploratory surgery, and is a powerful diagnostic indicator of VRF that is virtually invisible on standard 2D periapical radiographs.
Yes create a image
Generating Image
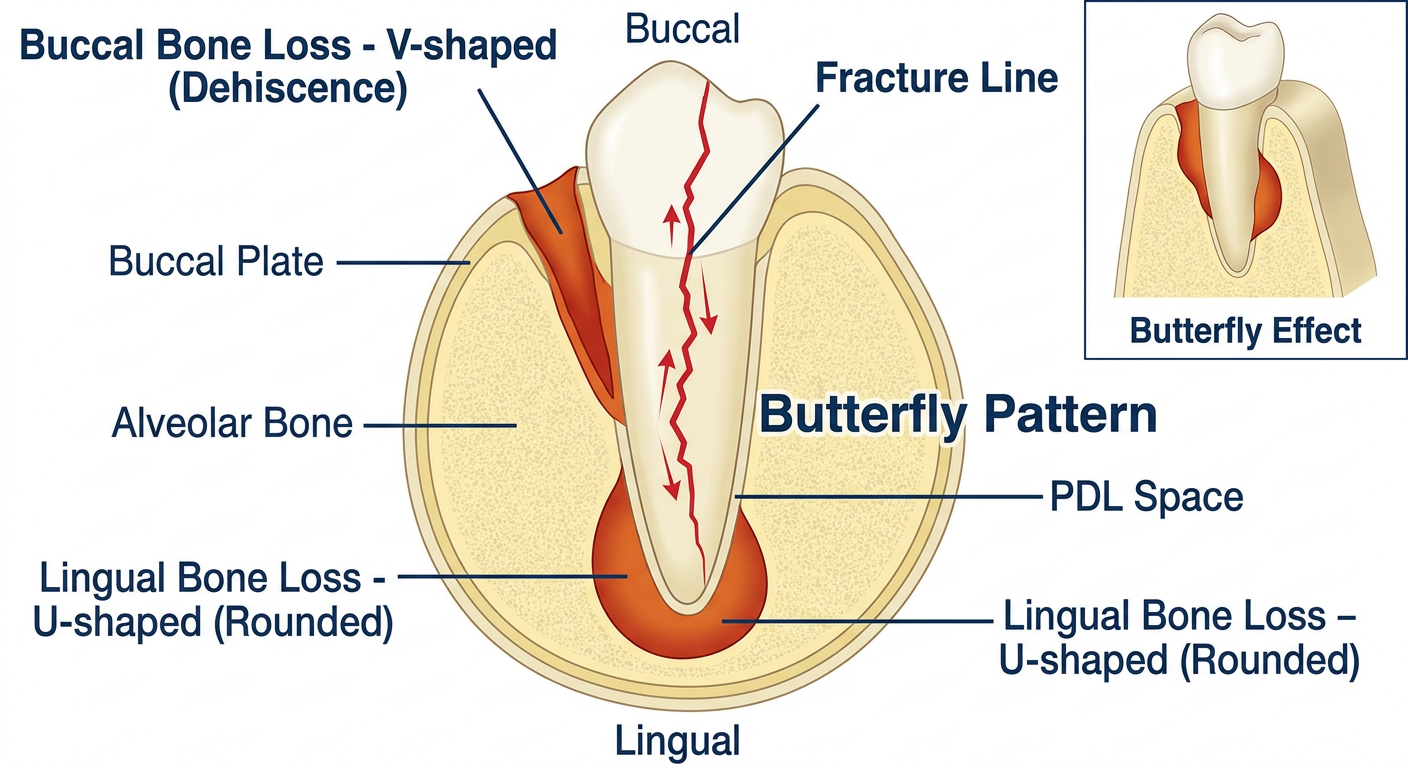
Here's the diagram illustrating the Butterfly Effect of VRF. It shows:
- Center: The root in cross-section (axial view) with the vertical fracture line running bucco-lingually (in red)
- Buccal wing (top): The sharp, deep V-shaped dehiscence - rapid resorption due to the thin buccal cortical plate
- Lingual wing (bottom): The shallow, rounded U-shaped defect - slower resorption due to the thicker lingual cortex ("shield phenomenon")
- Together, the two opposing bone defects create the classic butterfly wings appearance around the fractured root
This pattern is best visualized on CBCT axial slices or during exploratory surgery, and is virtually invisible on standard 2D periapical radiographs because the buccal and lingual surfaces are superimposed over the root image.
This is a shared conversation. Sign in to Orris to start your own chat.