Warburg effect
Reading File
Searching the Web
Warburg effect cancer metabolism aerobic glycolysis mechanism
Finding Sources
Searching PubMed
"Warburg effect" cancer metabolism aerobic glycolysis
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a thorough, well-illustrated answer. Here is the full response:
The Warburg Effect
Definition and Historical Background
The Warburg effect (also called aerobic glycolysis) is the observation that cancer cells preferentially convert glucose to lactate via glycolysis even when oxygen is abundant - a condition in which normal, non-proliferating cells would instead use the far more efficient mitochondrial oxidative phosphorylation pathway.
Otto Warburg first described this in the early 1920s, observing enhanced glucose uptake and lactate production in tumor cells compared to normal cells, even in oxygenated conditions. He received the Nobel Prize in 1931 for this discovery. - Robbins & Kumar Basic Pathology, p. 238
Normal vs. Cancer Cell Metabolism
| Feature | Normal (quiescent) cell | Cancer cell (Warburg) |
|---|---|---|
| O2 present | Oxidative phosphorylation | Aerobic glycolysis |
| O2 absent | Anaerobic glycolysis | Anaerobic glycolysis |
| ATP yield / glucose | ~30-32 mol | ~4 mol |
| ATP production rate | Slow but efficient | Fast but inefficient |
| End product | CO2 + H2O | Lactate |
| Biosynthetic output | Low (CO2 lost) | High (carbon retained) |
The Central Paradox - and Its Answer
Glycolysis yields only 2 ATP per glucose vs. oxidative phosphorylation's ~36 ATP per glucose. So why use it?
The answer is elegantly simple: growing cells need carbon, not just energy.
Oxidative phosphorylation's net reaction is:
Glucose + 6 O2 → 6 CO2 + 6 H2O
All carbon is exhaled as CO2. Nothing is left to build new cellular components. A dividing cell must replicate DNA, RNA, proteins, lipids, and organelles - it needs carbon skeletons, not just ATP.
Aerobic glycolysis shunts carbon-containing glycolytic intermediates into anabolic pathways:
- Nucleotide synthesis (via glucose-6-phosphate, ribose-5-phosphate through the HMP shunt)
- Amino acid synthesis (serine from 3-phosphoglycerate; glutamate from glutamine via TCA)
- Lipogenesis (acetyl-CoA and citrate from mitochondrial TCA intermediates)
- NADPH production (via the hexose monophosphate shunt, for biosynthetic reductive reactions)
Importantly, this is not unique to cancer. Rapidly proliferating normal cells (embryonic tissues, activated lymphocytes) also rely on aerobic glycolysis. "Warburg metabolism" is a general property of growing cells that cancer cells exploit and hard-wire permanently. - Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 284
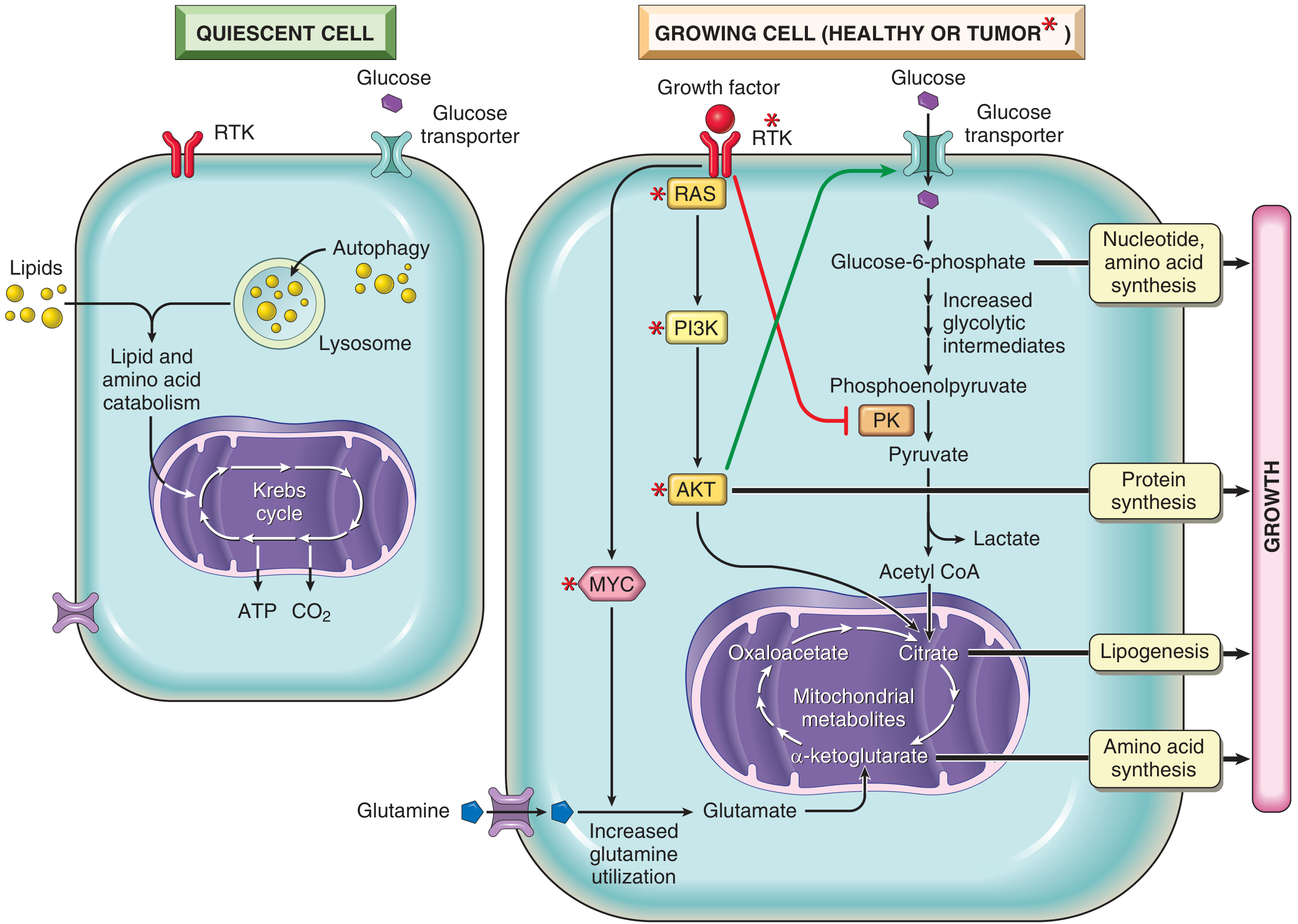
Fig. 6.22 from Robbins & Kumar Basic Pathology - quiescent cells vs. growing/tumor cells. Note how RAS, PI3K, AKT, and MYC (asterisked = frequently mutated in cancer) drive the reprogramming toward aerobic glycolysis and biosynthesis.
Why Aerobic Glycolysis Is Also Faster
Even though less efficient per molecule of glucose, ATP generation by glycolysis is kinetically faster than by oxidative phosphorylation. For rapidly proliferating cells that need immediate energy supply, speed of ATP generation matters. - Basic Medical Biochemistry, p. 1040
Molecular Drivers - How Cancer Hard-Wires the Warburg Effect
In normal cells, aerobic glycolysis is tightly regulated and ceases when growth signals stop. In cancer, oncogenic mutations lock these pathways on:
1. RAS / PI3K / AKT Signaling
- Upregulates glucose transporters (GLUT1, GLUT3) and glycolytic enzymes
- Promotes shunting of mitochondrial intermediates toward lipid biosynthesis
- Activates factors driving protein synthesis
- Receptor tyrosine kinases phosphorylate and inhibit pyruvate kinase (PK), damming upstream glycolytic intermediates that get siphoned off for DNA, RNA, and protein synthesis
2. MYC Oncogene
- Drives transcription of multiple glycolytic enzymes
- Upregulates glutaminase - enabling mitochondrial use of glutamine as a carbon source for TCA cycle intermediates
- Feeds both energy and biosynthesis needs
3. HIF-1 (Hypoxia-Inducible Factor-1)
- Normally activated by hypoxia; in cancer it can be constitutively active
- Drives expression of glycolytic enzymes and glucose transporters
- Implicated in transcriptional reprogramming toward aerobic glycolysis
4. Tumor Suppressors - Loss of the Brakes
-
p53: normally inhibits expression of genes involved in biosynthesis of cellular building blocks; lost in most cancers → no brake on anabolism
-
NF1 / PTEN: normally suppress RAS and PI3K signaling → their loss amplifies pro-growth metabolism
-
STK11 (LKB1): serine/threonine kinase that regulates multiple metabolic pathways; germline loss causes Peutz-Jeghers syndrome; somatic mutations found in many carcinomas
-
Robbins & Kumar Basic Pathology, p. 239; Robbins, Cotran & Kumar, p. 284-285
Additional Benefits of Aerobic Glycolysis for Tumor Cells
The Basic Medical Biochemistry textbook enumerates five key advantages:
- Rapid ATP generation for proliferation, despite inefficiency
- Glycolytic intermediates as feedstock for amino acid (serine, glycine), purine, and pyrimidine biosynthesis
- NADPH production via the HMP shunt, supporting reductive biosynthesis and antioxidant defense
- Lactate production acidifies the tumor microenvironment, promoting cellular invasion and metastasis
- Reduced acetyl-CoA production alters histone acetylation and epigenetic gene regulation, potentially favoring pro-proliferative gene expression patterns
- Basic Medical Biochemistry - A Clinical Approach, p. 1040
Glutamine: The Second Fuel
Beyond glucose, tumor cells avidly consume glutamine:
- Enters mitochondria to replenish TCA cycle intermediates (anaplerosis)
- Glutaminase (upregulated by MYC) converts glutamine → glutamate → α-ketoglutarate
- Provides carbon for amino acid and lipid synthesis
- Can generate additional pyruvate via malic enzyme
Clinical Relevance: PET Scanning
The practical clinical application of the Warburg effect is FDG-PET (18F-fluorodeoxyglucose positron emission tomography):
-
Tumors' "glucose hunger" means they preferentially take up injected radioactive glucose analog
-
Most tumors are PET-positive; rapidly growing ones are markedly so
-
Used for cancer staging, treatment response assessment, and recurrence detection
-
Robbins & Kumar Basic Pathology, p. 238
Oncometabolites - A Related Concept
Gain-of-function mutations in IDH1 and IDH2 (isocitrate dehydrogenase) cause an abnormal reaction: instead of converting isocitrate → α-ketoglutarate, mutant IDH produces 2-hydroxyglutarate (2-HG), an oncometabolite. 2-HG inhibits enzymes that depend on α-ketoglutarate (including TET2 DNA demethylases and histone demethylases), causing widespread epigenetic dysregulation and contributing to the transformed state. This links aberrant metabolism directly to cancer gene regulation. - Robbins & Kumar Basic Pathology, p. 240
Recent Research Perspectives
A 2023 review (Wang & Patti, Trends Cell Biol 2023, PMID 37117116) proposed a new framing: the Warburg effect may be a signature of mitochondrial overload - when mitochondria become saturated by the high biosynthetic demands of proliferating cells, excess pyruvate is redirected to lactate as an overflow valve. This reframes the effect as a consequence of biosynthetic activity rather than an inherent cancer-specific metabolic preference.
Summary
The Warburg effect reflects a fundamental metabolic re-wiring in cancer: glucose carbon is preserved in anabolic intermediates rather than being burned off as CO2. This is achieved by diverting pyruvate to lactate, keeping upstream carbon-rich intermediates available for building new cells. Oncogene mutations (RAS, MYC, PI3K/AKT) and tumor suppressor losses (p53, PTEN, STK11) lock this state on permanently. The resulting "glucose hunger" is the basis for PET scanning, and targeting cancer metabolism - through LDHA inhibitors, glutaminase inhibitors, or PDK inhibitors - remains an active therapeutic frontier.
This is a shared conversation. Sign in to Orris to start your own chat.