Montgomery T tube
Reading File
Finding Sources
Finding Sources
Searching the Web
Montgomery T tube tracheal stent indications placement complications
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Here is a comprehensive overview of the Montgomery T-Tube:
Montgomery T-Tube
What It Is
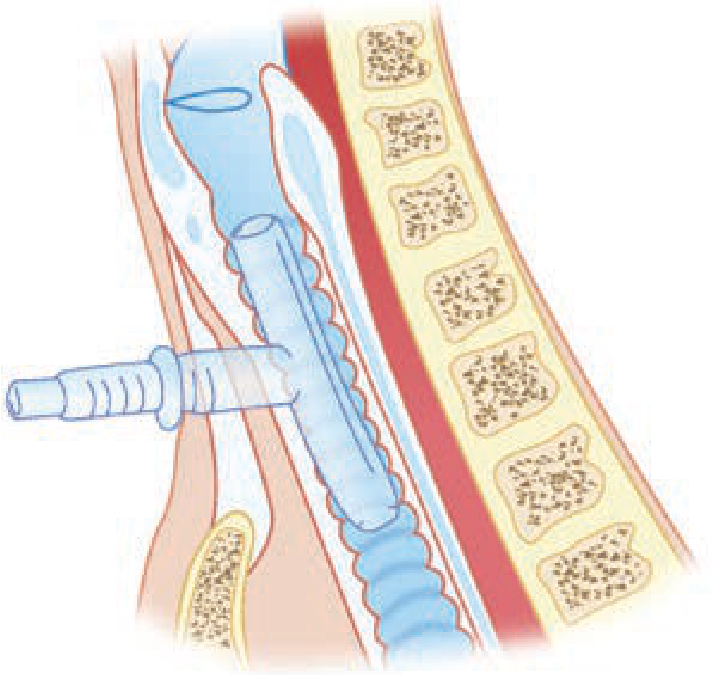
The Montgomery T-tube (also called the "Safe-T-Tube") is a silicone, T-shaped airway stent that functions simultaneously as a tracheal stent and a tracheostomy tube. It is a modification of a standard tracheostomy tube but has no inner cannula. The "T" shape consists of:
- Upper (vertical) limb - extends superiorly through the subglottis/stenotic segment toward the glottis
- Lower (vertical) limb - extends inferiorly in the trachea
- Horizontal (external) limb - exits through the tracheostomy stoma for access, suctioning, and ventilation
The diagram below illustrates the T-tube positioned in the trachea with the horizontal limb exiting through the tracheostomy:
Material & Design
- Made of implant-grade silicone - soft, pliable, and non-adherent smooth surface
- Available in clear or radiopaque material
- MRI-safe
- Comes in multiple series: Pediatric, Standard, Thoracic, Extra-Long, and Tapered
- A safety ring-and-groove system secures a plug to cap the external limb, allowing the patient to breathe and speak normally via the upper airway when plugged
Indications
The T-tube is used in benign and malignant tracheal/laryngotracheal disease:
| Category | Examples |
|---|---|
| Acute airway trauma | Blunt laryngotracheal injury |
| Tracheal/subglottic stenosis | Post-intubation, post-tracheostomy stenosis |
| Reconstructed/reconstituted trachea | After segmental resection and anastomosis |
| Stenosis not amenable to surgery | Long-segment stenosis, poor surgical candidates |
| Combined laryngotracheal stenosis | After simultaneous glottis + subglottis repair |
| Cervical trachea defects | When the cervical trachea cannot be repaired or reconstructed |
It is most commonly used for subglottic and upper tracheal stenosis and serves as an alternative to a solid stent when phonation is desired - the hollow lumen allows air passage to the vocal cords when the external limb is plugged. - Cummings Otolaryngology, p. 1217
As the Tintinalli's Emergency Medicine textbook notes: "The mainstay of treatment for symptomatic tracheal stenosis is surgical resection and anastomosis. When surgical treatment is not possible, the option exists for insertion of airway stents as a bridge to surgery, as a treatment for patients who are not surgical candidates, and in cases where there is a long segment of stenosis."
Contraindications
- Aspiration by the patient (risk of material entering the lung through the stent)
- Patients requiring positive pressure-assisted respiration (the T-tube is not compatible with standard mechanical ventilation via the tracheal route without special adaptors)
Advantages Over Solid Stents
| Feature | Solid Stent | Montgomery T-tube |
|---|---|---|
| Phonation | No | Yes (when external limb plugged) |
| Endotracheal intubation from above | Possible (through lumen) | Possible (through lumen) |
| Tracheostomy dependency | Yes (stent blocks airway above stoma) | No - upper limb patent |
| Suctioning access | Limited | Both limbs accessible |
Placement
- Inserted by an ENT or thoracic surgeon experienced with the device
- Placed under general anesthesia, typically with rigid bronchoscopy or direct laryngoscopy
- The external limb is plugged with the provided ring/plug system when the patient breathes spontaneously through the upper airway
- For anesthesia: a balloon catheter is used to occlude the upper end of the T-tube to create a closed system for ventilation
Nursing & Post-Operative Care
- Humidification and regular suctioning of both upper and lower limbs are essential - mucous plugging and crusting are the most common complications - Tintinalli's, Ch. 247
- Daily saline nebulizers are prescribed
- Carbocysteine may be added if mucus plugging is problematic
- The patient must be educated about the single-lumen design and its inherent higher risk of obstruction compared to double-cannula tubes
Complications
Early (perioperative)
- Postoperative fever
- Bleeding
- Excessive mucus secretion
- Irritating cough
- Short-term dyspnea
Late (long-term)
- Granulation tissue formation - most common at the upper edge, often due to friction from tube displacement during swallowing or speaking
- Mucous plugging / obstruction - from impaired expectoration
- Secondary infection / microbial colonization
- Tube dislodgement - migration from coughing or swallowing
- Ischemic mucosal injury - if pressure on mucosa exceeds 20-40 mmHg capillary pressure
Emergency Management of T-Tube Obstruction
- Suction both the upper and lower vertical limbs
- If obstruction persists after suctioning - remove the entire T-tube
- Re-establish airway via tracheostomy with an appropriately sized tracheostomy tube or endotracheal tube
- Do NOT attempt to pass an endotracheal tube blindly if the T-tube is still in situ
- Consult specialist (ENT/thoracic surgery) for re-insertion - Tintinalli's Emergency Medicine, Ch. 247
Relationship to Other Tracheal Stents
The Dumon tube is the other most commonly used silicone stent. Unlike the Montgomery T-tube, the Dumon is secured endoluminally via external studs and also has bronchial versions. The T-tube's unique advantage is its external access limb and the ability to support phonation.
A stent can also be fashioned from just the vertical limb of a T-tube (oversewn at the top, secured with a suture through the anterior commissure), used specifically as an endolaryngeal stent for laryngeal injuries - Cummings Otolaryngology, p. 1201; Scott-Brown's Otorhinolaryngology, Ch. 76.
This is a shared conversation. Sign in to Orris to start your own chat.