Neuropraxia
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Searching Images
nerve injury classification neuropraxia axonotmesis neurotmesis Seddon Sunderland diagram
I now have comprehensive information from multiple authoritative textbooks. Here is a complete overview of neuropraxia:
Neuropraxia (Neurapraxia)
Definition
Neuropraxia is the mildest grade of peripheral nerve injury (Seddon Class I / Sunderland Grade I). It results from brief or mild compression, traction, or blunt trauma to a nerve that causes focal/segmental demyelination while leaving the axon completely intact.
"The nerve conducts normally distal to but not across the lesion, resulting in conduction block, which is the electrophysiological correlate of neuropraxia." — Bradley and Daroff's Neurology in Clinical Practice
Pathophysiology
- Temporary mechanical distortion of myelin → segmental demyelination
- No Wallerian degeneration (axons and endoneurial tubes are intact)
- Results in a local conduction block at the injury site
- Nerve conduction is normal distal to the lesion but blocked across it
- Motor function is typically lost, but some sensation and autonomic function may be preserved (larger myelinated fibres are more susceptible than small unmyelinated fibres)
Common causes:
- Compression (e.g., "Saturday night palsy" — radial nerve compression causing wrist drop)
- Displaced fracture or dislocation (stretch/pressure on adjacent nerve)
- Tourniquet palsy
- Iatrogenic: needle trauma, injection pressure (e.g., mental nerve block)
Classification Context: Seddon & Sunderland
| Seddon | Sunderland | Structures Injured | Wallerian Degeneration? | Recovery |
|---|---|---|---|---|
| Neuropraxia | Grade I | Myelin only (focal demyelination) | ❌ No | Full; days–12 weeks |
| Axonotmesis | Grade II | Axon + myelin; endoneurium intact | ✅ Yes | Good; proximal→distal |
| Axonotmesis | Grade III | Axon + endoneurium disrupted; perineurium intact | ✅ Yes | Fair; may need surgery |
| Axonotmesis | Grade IV | Axon + endoneurium + perineurium disrupted; epineurium intact | ✅ Yes | Poor; surgery usually needed |
| Neurotmesis | Grade V | Complete nerve transection | ✅ Yes | None without surgery |
| — | Grade VI (Mackinnon) | Mixed injury (conduction block + axonal loss) | Variable | Variable |
— Sabiston Textbook of Surgery, Bradley and Daroff's Neurology, Rockwood and Green's Fractures
Clinical Features
- Complete motor paralysis of muscles innervated by the affected nerve
- Preserved or partially preserved sensation and autonomic function (compared to axonotmesis)
- No signs of Wallerian degeneration on nerve conduction studies
- Tinel's sign is absent (no axonal degeneration)
Electrodiagnostic Findings (EMG/NCS)
- Nerve conduction: Normal distal to the lesion; conduction block across the lesion
- EMG: No fibrillation potentials or positive sharp waves (no denervation, since axons are intact)
- Distal motor latency and conduction velocity: Normal distal to injury for 72–96 hours after injury (axons remain electrically viable distally before degeneration — but in neuropraxia, they remain permanently viable since there is no axonal injury)
This pattern distinguishes neuropraxia from axonotmesis, where fibrillation potentials appear 2–3 weeks post-injury.
Prognosis & Recovery
- Recovery is always complete if the causative compression/stretch is removed
- Timeline: days to 12 weeks (typically 6–12 weeks for full remyelination)
- Recovery pattern is not proximal-to-distal (unlike axonal regeneration in axonotmesis) — improvement can occur at any point along the nerve simultaneously, because axons are intact
Management
- Non-operative in most cases — remove the offending cause (reduce fracture, release compression, remove tourniquet)
- Physiotherapy to maintain joint mobility and prevent contractures during recovery
- Serial clinical and electrophysiological monitoring
- If no recovery by 3 months, re-evaluate (may indicate a worse injury grade than initially suspected)
- Surgical exploration is not indicated for isolated neuropraxia
Clinical Examples
| Scenario | Nerve | Mechanism |
|---|---|---|
| "Saturday night palsy" / "crutch palsy" | Radial nerve | Prolonged compression in axilla |
| Tourniquet palsy | Variable | Ischaemia + compression |
| Humeral shaft fracture (mild) | Radial nerve | Stretch/contusion |
| Lingual nerve (post-tonsillectomy) | Lingual nerve | Surgical retraction |
| Mental nerve (after nerve block) | Mental nerve | Injection pressure |
| Cervical cord neuropraxia (athlete) | Cervical cord | Transient hyperflexion/hyperextension |
| Obturator nerve (pelvic surgery) | Obturator nerve | Stretch during lymph node dissection |
Cervical Cord Neuropraxia (Special Context)
A distinct entity in athletes: transient bilateral sensory or motor deficit (burning pain, numbness, tingling) in ≥2 extremities following neck hyperflexion or hyperextension. Symptoms are transient and fully reversible. Functional spinal stenosis on MRI is an absolute contraindication to return to contact/collision sports.
— Textbook of Family Medicine, 9e
Sources: Bradley and Daroff's Neurology in Clinical Practice | Rockwood and Green's Fractures in Adults, 10e | Current Surgical Therapy, 14e | Sabiston Textbook of Surgery | Miller's Review of Orthopaedics, 9e | Textbook of Family Medicine, 9e
Axonotmosis
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive data from multiple authoritative sources. Here is the full breakdown:
Axonotmesis
Definition
Axonotmesis is the intermediate grade of peripheral nerve injury (Seddon Class II / Sunderland Grades II–IV). It is characterized by disruption of axons and their myelin sheaths with consequent Wallerian degeneration, while the connective tissue scaffolding (endoneurium, perineurium, epineurium) is variably preserved.
"Axonotmesis is the term used for a more severe blunt injury to a nerve, which causes disruption of the axons and myelin sheaths with consequent axonal degeneration." — Rockwood and Green's Fractures in Adults, 10e
Pathophysiology
Immediate events (at the injury site)
- Axonal continuity is lost at the injury site
- The severed axon undergoes retrograde die-back to the nearest node of Ranvier proximally
- The cell body (perikaryon) undergoes chromatolysis: nuclear peripheralization, rough ER fragmentation, and perikaryal swelling — a proregenerative response
Wallerian Degeneration (distal to injury)
- Occurs within 72–96 hours of axonal disruption
- The distal axon and myelin sheath fragment and degenerate
- Schwann cells and macrophages phagocytose myelin and cellular debris
- Distal end organs (muscle fibers, sensory receptors) become denervated
- The nerve does not conduct at or distal to the injury zone
Distal nerve tube changes
- Schwann cells proliferate and switch to a pro-regenerative phenotype (upregulate neurotrophic factors, form Bands of Büngner)
- However, if the distal stump remains denervated >1 month, Schwann cells begin to atrophy and lose this phenotype
- Endoneurial tube fibrosis and shrinkage progressively obstruct axonal regrowth
Denervated muscle changes
- ~30% of muscle weight lost in the first month
-
60% loss by the fourth month
- Muscle fiber atrophy, sarcoplasm loss, and denervation hypersensitivity (upregulation of nicotinic ACh receptors beyond the motor endplate)
Nerve Regeneration
The key feature distinguishing axonotmesis from neurotmesis: the connective tissue framework is at least partially intact, allowing guided regeneration.
- The proximal axon forms multiple growth cones (regenerative sprouting)
- Axons regrow through intact endoneurial tubes at 1–2 mm/day (~1 inch/month)
- Recovery proceeds proximal to distal
- Regenerating axons follow the same endoneurial pathway and reconnect with the same end organ (unlike neurotmesis)
- Full recovery, though slow, can approach near-normal
Sunderland Subclassification
Seddon's "axonotmesis" encompasses three Sunderland grades, each with different prognosis:
| Sunderland | Axon | Endoneurium | Perineurium | Epineurium | Prognosis | Surgery |
|---|---|---|---|---|---|---|
| Grade II | ✗ | ✓ Intact | ✓ Intact | ✓ Intact | Good — guided regeneration | Not usually |
| Grade III | ✗ | ✗ Disrupted | ✓ Intact | ✓ Intact | Variable — axonal misdirection, neuroma risk | Variable |
| Grade IV | ✗ | ✗ Disrupted | ✗ Disrupted | ✓ Intact | Poor — neuroma-in-continuity likely; no spontaneous recovery | Yes |
"If the sprouting axons are unable to reach the distal endoneurium, then a neuroma in continuity will develop, and no spontaneous recovery will occur (Sunderland class IV)." — Current Surgical Therapy, 14e
Clinical Features
- Complete loss of motor, sensory, and autonomic function (unlike neuropraxia, where sensation/autonomic may be partially preserved)
- No conduction at or distal to the injury on nerve conduction studies
- Progressive denervation atrophy of target muscles
- Tinel's sign may be present and advance distally as regeneration proceeds — a positive prognostic sign
Electrodiagnostic Findings (EMG/NCS)
| Finding | Timeframe | Significance |
|---|---|---|
| Absent motor/sensory response distal to injury | After 72–96 hrs | Wallerian degeneration complete |
| Fibrillation potentials & positive sharp waves | 2–3 weeks post-injury | Active denervation — hallmark of axonotmesis |
| Absent voluntary motor units in affected muscles | Immediately | Loss of axonal continuity |
| Nascent MUAPs (small, polyphasic) | Weeks–months | Early reinnervation |
| Advancing Tinel sign | Weeks–months | Ongoing axonal regeneration |
Studies are not diagnostically reliable for 3–6 weeks after injury due to the delay in Wallerian degeneration completion.
Prognosis
- Grade II: Excellent — complete recovery expected, axons follow intact endoneurial tubes to original targets
- Grade III: Fair — variable quality due to misdirected axons; some functional recovery but may be incomplete
- Grade IV: Poor — neuroma-in-continuity forms; surgical intervention needed
Recovery depends on:
- Distance from injury to target organ (longer = worse)
- Age (younger patients regenerate better)
- Timing of decompression/repair
- Severity of Schwann cell and endoneurial tube atrophy
Management
| Situation | Management |
|---|---|
| Grade II–III (confirmed or suspected) | Observation — allow spontaneous recovery; serial clinical + electrophysiologic assessment |
| No recovery by 3–4 months | Re-evaluate with EMG/NCS; consider surgical exploration |
| Grade IV (neuroma-in-continuity, no recovery) | Surgical: neurolysis, nerve grafting, or nerve transfer |
| Denervated muscle | Physiotherapy to prevent contracture; electrical stimulation |
- Peripheral nerve repair is best performed early (≤14 days), tension-free, in a clean wound bed
- Nerve gaps addressed with nerve conduit, decellularized nerve allograft, or autograft
- Nerve transfers considered for irreparable injuries (provide shorter reinnervation distance)
Classic Examples
| Injury | Nerve | Mechanism |
|---|---|---|
| Humeral shaft fracture | Radial nerve | Blunt contusion/crush — classically axonotmesis |
| "Stingers" with persistent weakness (athletes) | Brachial plexus roots | Traction/stretch |
| Crush injury to extremity | Variable | Direct compression |
| High-energy long bone fractures | Adjacent nerves | Distraction + blunt force |
Key Distinction: Axonotmesis vs. Neuropraxia vs. Neurotmesis
| Feature | Neuropraxia | Axonotmesis | Neurotmesis |
|---|---|---|---|
| Axon | Intact | Disrupted | Disrupted |
| Wallerian degeneration | ❌ | ✅ | ✅ |
| Endoneurium | Intact | Variably intact | Disrupted |
| Recovery | Full, fast (days–12 wks) | Good→Poor, slow (months) | None without surgery |
| Pattern | Not proximal→distal | Proximal→distal | Proximal→distal (if repaired) |
| Fibrillations on EMG | ❌ | ✅ | ✅ |
| Surgery | No | Sometimes | Always |
"The clinical features and neurophysiologic findings may be the same for axonotmesis and neurotmesis, yet there is a major difference in prognosis and management." — Rockwood and Green's Fractures in Adults, 10e
Sources: Bradley and Daroff's Neurology in Clinical Practice | Rockwood and Green's Fractures in Adults, 10e | Current Surgical Therapy, 14e | Ganong's Review of Medical Physiology, 26e | Miller's Review of Orthopaedics, 9e | Sabiston Textbook of Surgery
GB syndrome
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content from Adams & Victor, Bradley & Daroff, and Miller's Anesthesia. Here is the complete overview:
Guillain-Barré Syndrome (GBS)
Full name: Landry-Guillain-Barré-Strohl Syndrome | Also known as: Acute Inflammatory Demyelinating Polyradiculoneuropathy (AIDP)
Definition
GBS is an immune-mediated acute polyradiculoneuropathy characterized by rapidly progressive, ascending, symmetric limb weakness — with or without sensory disturbances — associated with reduced or absent reflexes. It is the most common cause of acute flaccid paralysis worldwide and the leading cause of acute generalized paralysis in the post-polio era.
Epidemiology
- Incidence: 1–2 per 100,000/year (mean 1.8/100,000)
- Affects all ages; incidence rises with age (0.8/100,000 <18 yrs → 3.2/100,000 ≥60 yrs)
- Males slightly more affected (M:F ratio 1.5:1)
- Nonseasonal (except AMAN, which has summer epidemics in China)
- Highest attack rates in persons aged 50–74 years
Antecedent Events (Triggers)
~60% of cases are preceded by an infection 1–3 weeks before neurological onset:
| Organism | Notes |
|---|---|
| Campylobacter jejuni | Most common identified antecedent; strongly linked to axonal subtypes (AMAN/AMSAN), anti-GM1 antibodies |
| Cytomegalovirus (CMV) | Common viral trigger |
| Epstein-Barr virus | |
| HIV | |
| Mycoplasma pneumoniae | |
| Haemophilus influenzae | Linked to MFS (anti-GQ1b) |
| Hepatitis E virus, Zika virus, Influenza A | |
| Vaccinations | Influenza (swine flu 1976 most notable); ~2/million doses COVID adenoviral vaccine |
| Surgery | Post-operative GBS is recognized |
| Immune checkpoint inhibitors | |
| Lymphoma (especially Hodgkin's) |
Pathophysiology & Immunology
The initiating event is molecular mimicry — the immune response against an infectious agent cross-reacts with peripheral nerve antigens.
AIDP (classic demyelinating form)
- T-cell mediated autoimmune attack + humoral amplification
- Earliest event: complement deposition on the inner myelin surface
- Macrophages strip myelin lamellae from the axon (macrophage-mediated demyelination)
- Perivascular mononuclear infiltration (monocytes, macrophages, T lymphocytes) in the endoneurium
- Schwann cells upregulate class II MHC, potentially presenting antigen to autoreactive T cells
- Intense inflammation can cause secondary axonal degeneration (bystander effect)
Key autoantibodies
| Antibody | Associated subtype/variant | Trigger |
|---|---|---|
| Anti-GQ1b | Miller-Fisher syndrome (~90%+) | H. influenzae, C. jejuni |
| Anti-GM1 / Anti-GD1a | AMAN | C. jejuni (76% in Chinese AMAN) |
| Anti-GD1b, Anti-GT1b | Pharyngeal-cervical-brachial variant |
Pathological progression (AIDP):
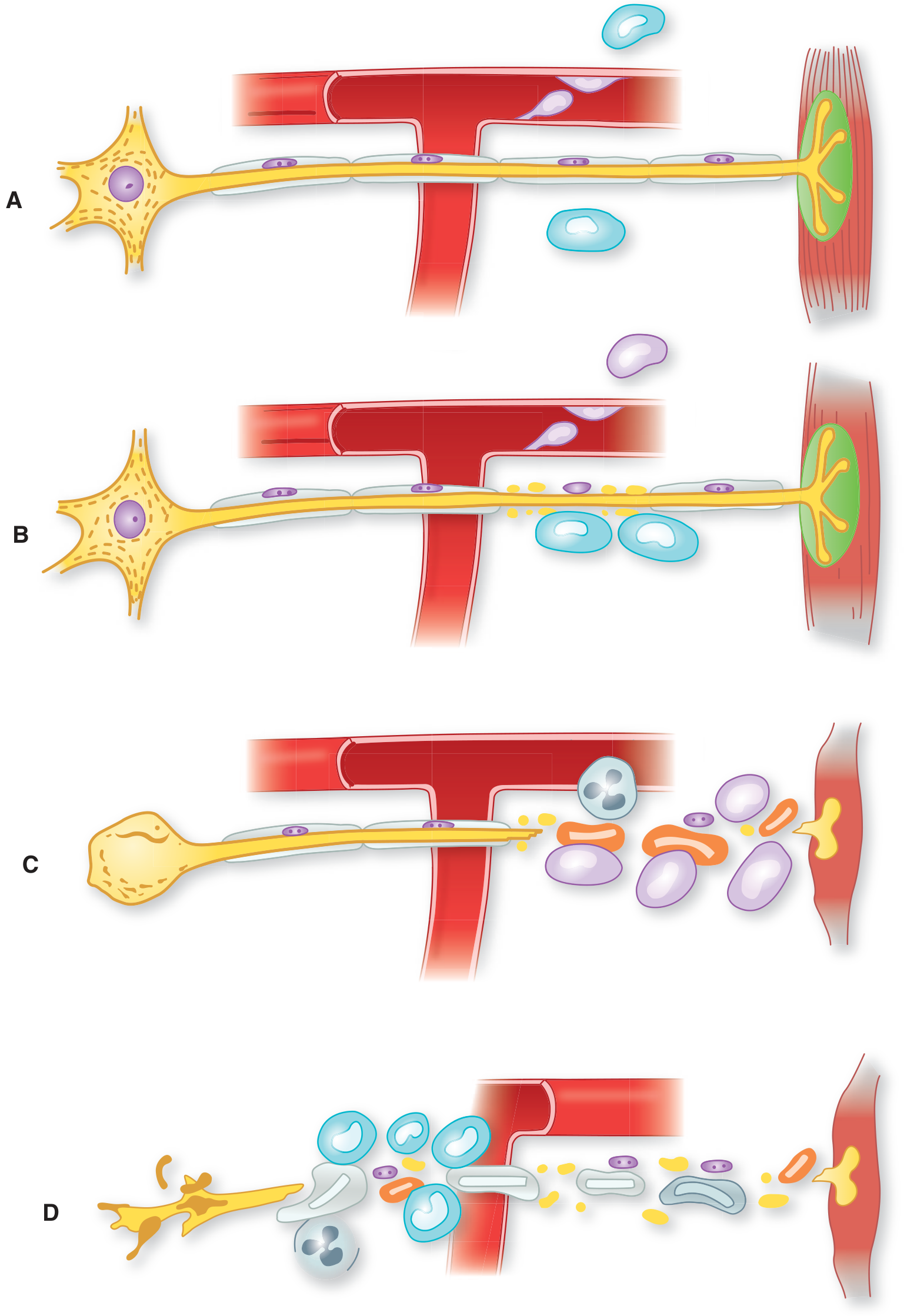
Cellular events in GBS: A → lymphocyte migration (no nerve damage); B → segmental demyelination (axon intact); C → axonal interruption + denervation atrophy; D → proximal axonal loss → neuronal death, no regeneration — Adams & Victor's Principles of Neurology, 12e
Classification of Subtypes
Common Subtypes
| Subtype | Pathology | Key Features | Antibody | Prognosis |
|---|---|---|---|---|
| AIDP (most common in West) | Demyelination | Classic ascending weakness + sensory symptoms | Variable | Good |
| AMAN (most common in Asia) | Axonal — motor only | Pure motor, no sensory; summer epidemics in children | Anti-GM1, anti-GD1a | Often rapid recovery |
| AMSAN | Axonal — motor + sensory | Fulminant, severe quadriparesis, prolonged ventilation | Anti-GD1a | Poor |
Rare Variants
| Variant | Triad / Key Features | Antibody |
|---|---|---|
| Miller-Fisher Syndrome (MFS) | Ophthalmoplegia + Ataxia + Areflexia; motor preserved | Anti-GQ1b (>90%) |
| Pharyngeal-cervical-brachial | Dysphagia, facial/cervical/brachial weakness | Anti-GD1a, anti-GT1b |
| Facial diplegia with paresthesias | Bilateral facial palsy | — |
| Acute pandysautonomia | Isolated autonomic failure | — |
| Paraparetic variant | Lower limb-predominant | — |
| Ataxic variant | Sensory ataxia without weakness | — |
Clinical Features
Motor
- Ascending, symmetric weakness beginning in lower limbs, spreading to upper limbs, facial, oropharyngeal, and (in severe cases) respiratory muscles
- Severity: mild difficulty walking → complete quadriplegia
- Areflexia/hyporeflexia — invariable feature (may be absent very early)
- Cranial nerve involvement in 45–75% of cases; bilateral facial paresis in ≥50%
Sensory
- Paresthesias (often worse in hands and fingers) are common at onset
- Objective sensory loss is not prominent — typically limited to distal vibration sense impairment
- Pain (limb, back, interscapular) in ~70% during acute phase; persists ≥1 year in one-third
Autonomic (65% of hospitalized patients)
- Most significant in the first 2–4 weeks (peak paralysis)
- Orthostatic hypotension, urinary retention, GI atony (ileus), iridoplegia
- Sinus tachycardia, hypertension, anhidrosis or diaphoresis
- Bradycardia, heart block, asystole — "vagal spells" triggered by tracheal suctioning
- ECG changes: T-wave abnormalities, ST depression, QT prolongation, heart block
- Up to two-thirds of deaths during recovery result from cardiovascular/respiratory dysfunction
Respiratory
- Respiratory failure requiring ventilation: 9–30% of hospitalized patients
- Higher risk with older age and rapid progression
- Monitor with bedside FVC and NIF (negative inspiratory force); intubate if FVC <20 mL/kg or rapid decline ("20-30-40 rule")
Diagnostic Criteria (Asbury & Cornblath)
Required
- Progressive weakness of both legs and arms
- Areflexia or hyporeflexia
Supportive — Clinical
- Progression over days to 4 weeks
- Relative symmetry
- Mild sensory symptoms/signs
- Bifacial palsies
- Autonomic dysfunction
- Absence of fever at onset
- Recovery beginning 2–4 weeks after progression ceases
Supportive — Laboratory
- Albuminocytological dissociation: elevated CSF protein with <10 cells/μL (normal cell count)
- Electrodiagnostic features: conduction slowing or block
Investigations
CSF Analysis
- Classic finding: high protein, normal cells (albuminocytological dissociation)
- Protein often >45 mg/dL; may be >200 mg/dL in severe cases
- CSF pleocytosis >50 cells/μL should cast doubt on GBS diagnosis (consider Lyme, HIV, CMV)
Electrodiagnostics (EMG/NCS)
- May be normal in the first week — characteristic changes emerge at 1–2 weeks
- AIDP: reduced conduction velocity, prolonged distal latencies, conduction block, absent/prolonged F-waves, temporal dispersion
- AMAN: reduced/absent CMAPs with normal SNAPs, normal conduction velocity (no demyelination)
- AMSAN: markedly reduced/absent CMAPs and SNAPs; abundant fibrillations on needle EMG
Antibodies
- Anti-GQ1b in Miller-Fisher syndrome
- Anti-GM1 in AMAN (especially post-C. jejuni)
Treatment
Immunotherapy (equally effective options)
| Treatment | Dose | Notes |
|---|---|---|
| IV Immunoglobulin (IVIG) | 0.4 g/kg/day × 5 days (total 2 g/kg) | First-line; safe in pregnancy |
| Plasma exchange (PE) | 5 exchanges over 2 weeks | Equally effective; safe in pregnancy |
- Combination of IVIG + PE is not superior to either alone
- Corticosteroids are NOT beneficial (no evidence of benefit; may worsen outcome)
- Neither treatment alters the extent of nerve damage or disease progression — they accelerate recovery
Supportive Care (crucial)
- Respiratory monitoring: serial FVC, NIF; prophylactic intubation if FVC <20 mL/kg
- Cardiac monitoring in ICU (continuous ECG, arterial line)
- DVT prophylaxis (high risk due to immobility)
- Pain management (gabapentin, opioids, carbamazepine)
- Physiotherapy and rehabilitation
- Nutritional support; nasogastric feeding if bulbar involvement
Prognosis
- Mortality: ~1–5% (down from 33% before positive-pressure ventilation)
- ~80% recover independent ambulation by 6 months
- ~10–15% have persistent severe disability
- ~5–10% relapse (consider CIDP if >2 relapses)
- Poor prognostic factors: older age, rapid progression, preceding C. jejuni infection, AMSAN subtype, need for ventilation, absent CMAPs on EMG
Differential Diagnosis
| Category | Condition |
|---|---|
| Peripheral nerve/root | Acute intermittent porphyria, diphtheria, critical illness polyneuropathy, vasculitic neuropathy, Lyme polyradiculopathy |
| Neuromuscular junction | Myasthenic crisis, botulism, tick paralysis |
| Muscle | Inflammatory myopathy, hypokalaemia, rhabdomyolysis, hypermagnesaemia |
| Spinal cord | Transverse myelitis, cord compression (urgent MRI — sensory level, early urinary retention) |
| Brainstem | Basilar artery thrombosis, central pontine myelinolysis |
Sources: Adams and Victor's Principles of Neurology, 12e | Bradley and Daroff's Neurology in Clinical Practice | Miller's Anesthesia, 10e | Goldman-Cecil Medicine
Thanks
You're welcome! Feel free to ask whenever you're ready to continue — whether it's neurotmesis to complete the nerve injury series, or any other topic.
Common personel nerve (CPN)
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Common personel nerve (CPN)
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
common peroneal fibular nerve anatomy branches foot drop
Loading Image
Reading File
I now have comprehensive content. Here is the full overview:
Common Peroneal Nerve (CPN)
Also called: Common Fibular Nerve (CFN) — the preferred anatomical term per FCAT nomenclature
Anatomy & Course
Origin
- Arises from the sciatic nerve in the popliteal fossa (dorsal divisions of L4, L5, S1, S2)
- The sciatic nerve divides into the CPN and the tibial nerve close to the popliteal fossa
Course
- Runs along the lateral border of the popliteal fossa adjacent to the biceps femoris tendon
- Winds around the neck of the fibula (lateral aspect) — most vulnerable point
- Passes through the origin of peroneus longus muscle ("fibular tunnel")
- Divides into its two terminal branches: the deep and superficial peroneal nerves
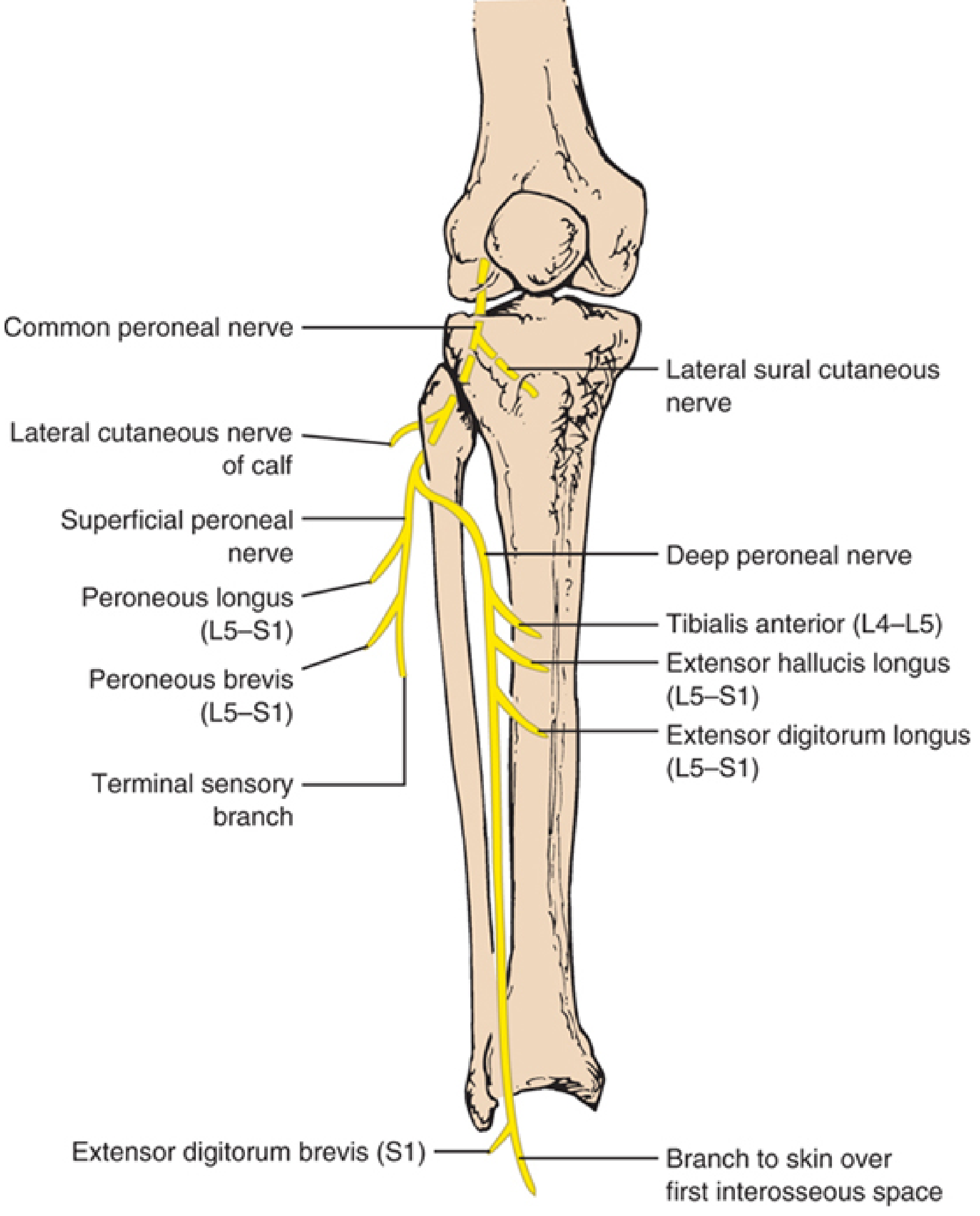
Common peroneal nerve anatomy — Localization in Clinical Neurology, 8e
Branches & Their Functions
Before Division (in popliteal fossa)
| Branch | Distribution |
|---|---|
| Lateral sural cutaneous nerve | Skin over upper lateral leg; joins medial sural cutaneous nerve (from tibial) → forms sural nerve |
| Lateral cutaneous nerve of the calf | Skin on lateral aspect of the leg below the knee |
Deep Peroneal Nerve (Anterior Tibial Nerve)
Traverses the anterior compartment of the leg.
| Muscle | Root | Function | Test |
|---|---|---|---|
| Tibialis anterior | L4–L5 | Dorsiflexion + inversion of foot | Dorsiflex foot against resistance; walk on heels |
| Extensor hallucis longus | L5–S1 | Extension of great toe + dorsiflexion | Dorsiflex distal phalanx of big toe against resistance |
| Extensor digitorum longus | L5–S1 | Extension of 4 lateral toes + dorsiflexion | Dorsiflex toes against resistance |
| Extensor digitorum brevis | L5–S1 | Extension of great toe + 3 medial toes | Dorsiflex proximal phalanges against resistance |
| Peroneus tertius | L5–S1 | Dorsiflexion + eversion | — |
Sensory: Skin over the first interosseous space (web space between 1st and 2nd toes) — very small area; preserved in superficial peroneal nerve lesions.
Superficial Peroneal Nerve
Innervates the lateral compartment of the leg.
| Muscle | Root | Function | Test |
|---|---|---|---|
| Peroneus longus | L5–S1 | Plantarflexion + eversion | Evert foot against resistance |
| Peroneus brevis | L5–S1 | Plantarflexion + eversion | Evert foot against resistance |
Sensory: Lateral lower two-thirds of the leg + entire dorsum of the foot and toes (except the first web space).
Anatomical Variant
In 20–28% of individuals, an accessory deep peroneal nerve arises from the superficial peroneal nerve and supplies the lateral part of extensor digitorum brevis (4th–5th digits) — wraps around the lateral malleolus.
Why Is the CPN So Vulnerable?
The CPN is the most frequently injured nerve in the lower extremity and the most common compressive neuropathy of the leg. Its vulnerability at the fibular neck is due to:
- It is superficial — lies directly against bone with minimal soft tissue protection
- It is tethered — fixed at the sciatic bifurcation proximally and at the fibular tunnel distally, making it susceptible to traction
- The fibular tunnel (origin of peroneus longus) is a tight fibro-osseous channel
Causes of CPN Injury
At the Fibular Head / Neck (most common site)
| Mechanism | Examples |
|---|---|
| Compression (most common cause) | Intraoperative improper positioning/padding, leg crossing (habitual), casts, orthoses, antithrombotic stockings, prolonged bed rest |
| Traction/stretch | Acute forceful foot inversion (football kicking → "punter's palsy"), prolonged squatting ("strawberry pickers' palsy"), yoga ("yoga foot drop"), lithotomy position |
| Trauma | Fibular fracture, knee dislocation, lacerations, blunt trauma, gunshot wounds |
| Iatrogenic | Knee surgery (total knee arthroplasty, arthroscopy, lateral meniscus repair), lateral decubitus position |
| Intraneural ganglia | From disruption of superior tibiofibular joint capsule → synovial fluid tracks along articular branch — underappreciated cause |
| Weight loss | "Slimmer's paralysis" — loss of protective fat pad |
| Postpartum | Stirrup compression, prolonged squatting during labour, "pushing palsy" (bilateral) |
| Tumours/masses | Osteochondroma (compresses nerve at fibular neck), schwannoma, Baker cyst, ganglion |
In a series of 318 knee-level CPN lesions: stretch/contusion 51%, laceration 12%, tumour 13%, entrapment 9%, iatrogenic 4%, gunshot 4%.
Clinical Features of CPN Palsy
Motor
- Foot drop — inability to dorsiflex the foot (hallmark)
- Steppage gait — patient raises knee high to clear the plantar-flexed foot
- Weakness of toe extension (EHL, EDL)
- Weakness of foot eversion (peroneus longus/brevis) — may be spared in selective deep peroneal lesions
- Deep peroneal (anterior compartment) is more commonly affected than the whole nerve — weakness more prominent in dorsiflexion/toe extension than eversion
Sensory
- Loss over lateral lower two-thirds of leg and dorsum of foot (superficial peroneal distribution)
- First web space preserved in pure superficial peroneal lesions; lost in deep peroneal or complete CPN lesions
- Pain is rare (except with intraneural ganglia, which typically present with knee/peroneal distribution pain and fluctuating weakness with weight bearing)

Differential Diagnosis of Foot Drop
| Condition | Key Distinguishing Features |
|---|---|
| L5 radiculopathy | Also affects tibialis posterior (foot inversion — L5, tibial nerve), medial hamstrings, gluteus medius; may have back pain; paraspinals abnormal on EMG |
| Sciatic nerve lesion (fibular division predominant) | Short head of biceps femoris affected (innervated by fibular division of sciatic in thigh) — spared in CPN lesion |
| Lumbosacral plexopathy (lumbosacral trunk) | Multiple root levels; involves other L4/L5 muscles not innervated by CPN |
| Anterior tibial compartment syndrome | Deep peroneal nerve affected within compartment; compartment pressure elevated; emergency |
| Stroke / upper motor neuron | Spasticity, hyperreflexia, Babinski |
Key EMG rule: Short head of biceps femoris is innervated by the fibular division of the sciatic nerve in the thigh — abnormal in sciatic lesion, normal in CPN lesion (critical localizing point).
Investigations
Electrodiagnostics (EMG/NCS)
- Nerve conduction: Motor studies recording tibialis anterior or EDB — reduced/absent CMAP; focal conduction block or slowing across the fibular head can sometimes be demonstrated
- Contrary to ulnar nerve at the elbow, localized slowing at the fibular head is not the most common finding — axonal loss is the most frequent pathophysiology
- Axonal loss: diffusely low/absent fibular motor + superficial peroneal sensory amplitudes
- Needle EMG: Denervation (fibrillations, positive sharp waves) in CPN-innervated muscles (tibialis anterior, peronei, EDB); short head of biceps femoris normal (distinguishes from sciatic/L5); tibialis posterior and medial gastrocnemius normal (distinguishes from L5 radiculopathy)
- Normal paraspinal muscles (distinguishes from L5 root)
Imaging
- Ultrasound: Slightly more accurate than MRI for compressive fibular neuropathies; thickened nerve (cross-sectional area >8 mm²) in ~70%; identifies intraneural ganglia and soft-tissue masses
- MRI: Effective for intraneural ganglia; shows denervation edema in anterior and lateral compartment muscles (T2 hyperintensity)
Management
Conservative
- Remove the offending cause (improve positioning, remove cast/bandage, avoid leg crossing)
- Ankle-foot orthosis (AFO) — custom-made plastic; improves steppage gait and prevents equinus contracture
- Physiotherapy: stretching, strengthening, gait training
- Most acute demyelinating (neuropraxia) lesions recover fully within days to 12 weeks
Surgical Indications
- No spontaneous improvement after 3 months of conservative management
- Pain or slowly progressive lesion (may indicate intraneural ganglion or tumour)
- Penetrating injury or known neurotmesis
- Options: neurolysis, excision of compressive lesion (ganglion, osteochondroma), nerve grafting
Prognosis
- Uniformly good for acute demyelinating (neuropraxia) lesions
- Delayed and incomplete recovery for axonal loss lesions and stretch injuries
- The distal fibular motor amplitude (recording tibialis anterior) is the best prognostic indicator — correlates with extent of axonal loss
- Studies should be performed bilaterally and compared for accurate assessment
Sources: Localization in Clinical Neurology, 8e | Bradley and Daroff's Neurology in Clinical Practice | Adams and Victor's Principles of Neurology, 12e | Gray's Anatomy for Students
Tibialis posterior tendon trasfer for foot drop.
Finding Sources
Finding Sources
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Acl and MCL injury xray finding.
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Searching Images
Segond fracture ACL tear knee radiograph x-ray
Reading File
Loading Image
I now have comprehensive data. Here is the complete overview:
ACL and MCL Injury — X-Ray Findings
Key Concept Upfront
Ligaments are not visible on plain X-ray. ACL and MCL tears themselves cannot be directly seen on radiographs. However, X-ray is essential as the first-line investigation to identify:
- Associated bony avulsion fractures (pathognomonic markers of ligament injury)
- Joint effusion / lipohemarthrosis
- Joint space widening under stress
- Tibial slope and limb alignment
MRI is the definitive modality for direct ligament visualization.
ACL Injury — X-Ray Findings
Standard Views
AP, lateral, sunrise (patella), and intracondylar notch views are obtained.
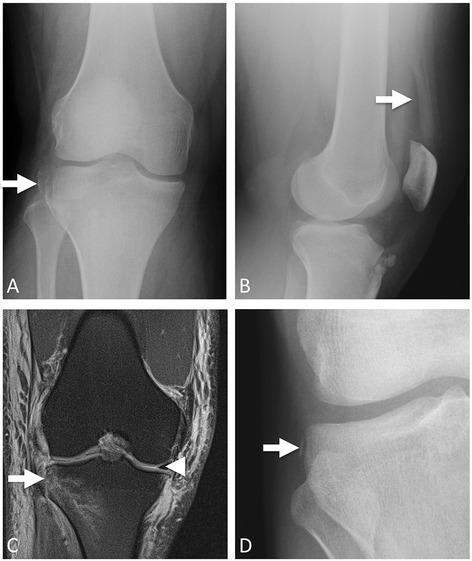
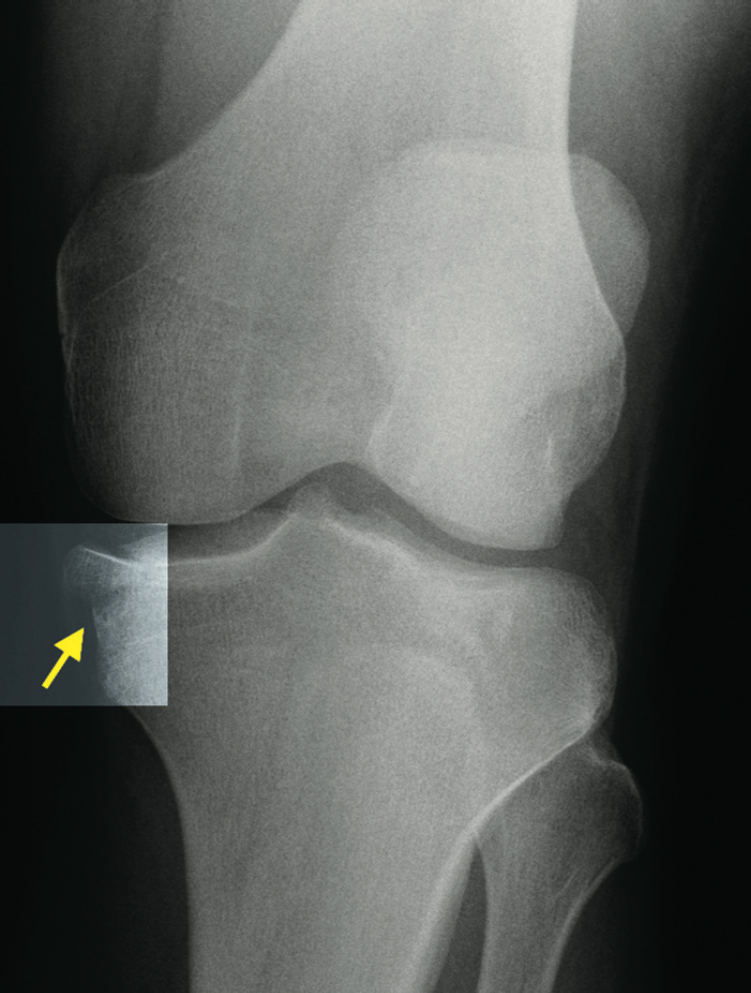
1. Segond Fracture ⭐ (Pathognomonic for ACL Tear)
The most important X-ray finding in ACL injury.
- Definition: Small, vertically oriented cortical avulsion fracture off the posterolateral margin of the lateral tibial plateau
- Mechanism: Avulsion by the anterolateral ligament (ALL) or lateral joint capsule during forced internal rotation + varus stress
- Location on X-ray: Lateral tibial plateau, just distal to the articular surface — AP view
- ACL association: ACL rupture present in 75–100% of Segond fractures
- Also highly associated with lateral meniscus tear and medial meniscus tear (~75% each)
2. Tibial Eminence / Intercondylar Eminence Fracture
- Avulsion of the ACL tibial insertion — more common in children (instead of midsubstance ACL tear)
- Seen on lateral view as a displaced bony fragment lifted off the tibial eminence
- Classified by Meyers & McKeever (Type I–III based on displacement)
- On AP: irregular or absent tibial eminence; on lateral: fragment displaced superiorly into joint
3. Lipohemarthrosis (Lateral View)
- Fat-fluid level in the suprapatellar bursa on lateral X-ray
- Indicates an intra-articular fracture with release of bone marrow fat
- Strongly suggests ACL tibial avulsion or tibial plateau fracture
- Specific but not exclusive to ACL injury
4. Blumensaat Line (Lateral View — Indirect Sign)
- Blumensaat line = line drawn along the roof of the intercondylar notch on lateral X-ray
- In a normal knee at ~30° flexion, the inferior pole of the patella should lie on this line
- Not an X-ray sign of ACL injury per se — used on MRI: intact ACL fibers should parallel Blumensaat line on sagittal imaging
5. Posterior Tibial Slope (Lateral View)
- Measured on lateral radiograph
- Values >12° are associated with ACL graft failure after reconstruction
- Important in surgical planning
6. Joint Effusion
- Hemarthrosis beginning within 12 hours of injury is highly suggestive of ACL tear (vs. meniscal tears which cause delayed swelling at 12–24 hours)
- Seen as suprapatellar soft tissue fullness on lateral view
Summary — ACL X-ray Findings
| Finding | View | Significance |
|---|---|---|
| Segond fracture | AP | Pathognomonic; ACL tear in 75–100% |
| Tibial eminence avulsion | Lateral | Pediatric ACL equivalent |
| Lipohemarthrosis (fat-fluid level) | Lateral | Intra-articular fracture/avulsion |
| Hemarthrosis (soft tissue swelling) | Lateral | Acute ligament/bone injury |
| Tibial slope >12° | Lateral | ACL graft failure risk |
MCL Injury — X-Ray Findings
MCL tears are almost never directly visible on plain X-ray. X-ray is used to detect associated bony injuries.
1. Pellegrini-Stieda Lesion (Pellegrini-Stieda Disease)
- Definition: Calcification / ossification of the proximal MCL (at or near the femoral attachment) following injury
- Represents a chronic/healed MCL injury — a late finding (weeks to months post-injury)
- Seen on AP view as a linear or curvilinear calcification along the medial femoral condyle
- Patient presents with medial knee pain, local tenderness, and a palpable mass at the femoral MCL attachment
- Due to incomplete MCL rupture → periosteal reaction → heterotopic ossification
2. Medial Joint Space Widening (Stress Views)
- Valgus stress radiograph: widening of the medial joint space indicates MCL incompetence
- Grading:
- Grade I (sprain): <5 mm opening
- Grade II (partial tear): 5–9 mm opening
- Grade III (complete tear): ≥10 mm opening (or 3–5 mm more than contralateral side)
3. Avulsion Fractures at MCL Attachment
- MCL avulsion from medial femoral epicondyle (proximal MCL)
- MCL avulsion from medial tibial flare (distal MCL)
- Small flakes of bone visible on AP view at the medial joint margin
4. Reverse Segond Fracture
- Medial counterpart of the Segond fracture
- Small cortical avulsion off the medial tibial plateau (deep MCL / medial meniscotibial ligament attachment)
- Highly associated with PCL injury and MCL injury
- Indicates severe rotational instability (anteromedial)
Summary — MCL X-ray Findings
| Finding | View | Significance | Timing |
|---|---|---|---|
| Pellegrini-Stieda ossification | AP | Chronic/healed MCL injury | Late (weeks–months) |
| Medial joint space widening (stress) | AP valgus stress | Grades MCL laxity | Acute |
| Medial femoral/tibial avulsion flake | AP | Bony MCL avulsion | Acute |
| Reverse Segond fracture | AP | MCL + PCL injury | Acute |
Combined ACL + MCL Injury ("Terrible Triad" / O'Donoghue Triad)
When ACL + MCL are both injured, the classic O'Donoghue's unhappy triad = ACL + MCL + medial meniscus tear (modern series more commonly show lateral meniscus involvement).
X-ray findings may include:
- Segond fracture (ACL component)
- Medial joint space widening on valgus stress (MCL component)
- Diffuse hemarthrosis / lipohemarthrosis
Recommended X-ray Series for Knee Ligament Injury
| View | Purpose |
|---|---|
| AP weight-bearing | Segond fracture, medial/lateral joint space, MCL avulsion |
| Lateral | Lipohemarthrosis, tibial eminence avulsion, tibial slope, Blumensaat line, effusion |
| Valgus stress AP | Grade MCL laxity |
| Intracondylar notch (tunnel view) | Loose bodies, osteochondral defects |
| Sunrise (skyline) | Patellar fracture, patellofemoral assessment |
Bottom line: Plain X-rays are normal in most isolated ACL and MCL tears. The key radiographic marker for ACL injury is the Segond fracture (pathognomonic); for MCL, Pellegrini-Stieda ossification (chronic) and medial joint space widening on stress views (acute). MRI is required for definitive diagnosis and surgical planning.
— Sources: Grainger & Allison's Diagnostic Radiology | Miller's Review of Orthopaedics, 9e | Rockwood and Green's Fractures in Adults, 10e | Rosen's Emergency Medicine | Bailey & Love's Surgery, 28e | S Das Manual on Clinical Surgery, 13e
Can you please explain about the brain and functions
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Here is a comprehensive overview of the brain and its functions, drawn from authoritative neuroscience and medical physiology textbooks.
The Brain — Structure and Functions
Overview
The human brain is the most complex organ in the body — weighing approximately 1.4 kg and containing roughly 86 billion neurons. It is divided into several major regions, each with distinct and overlapping functions.
Major Divisions of the Brain
1. Cerebral Hemispheres (Telencephalon)
The cerebral hemispheres form the largest part of the brain and consist of:
- Cerebral cortex (grey matter outer layer)
- Underlying white matter (connecting fibres)
- Deep nuclei: basal ganglia, hippocampus, amygdala
Overall functions: perception, higher motor functions, cognition, memory, and emotion.
Each hemisphere controls the opposite (contralateral) side of the body. In most people, the left hemisphere is dominant for language.
The Four Lobes of the Cerebral Cortex
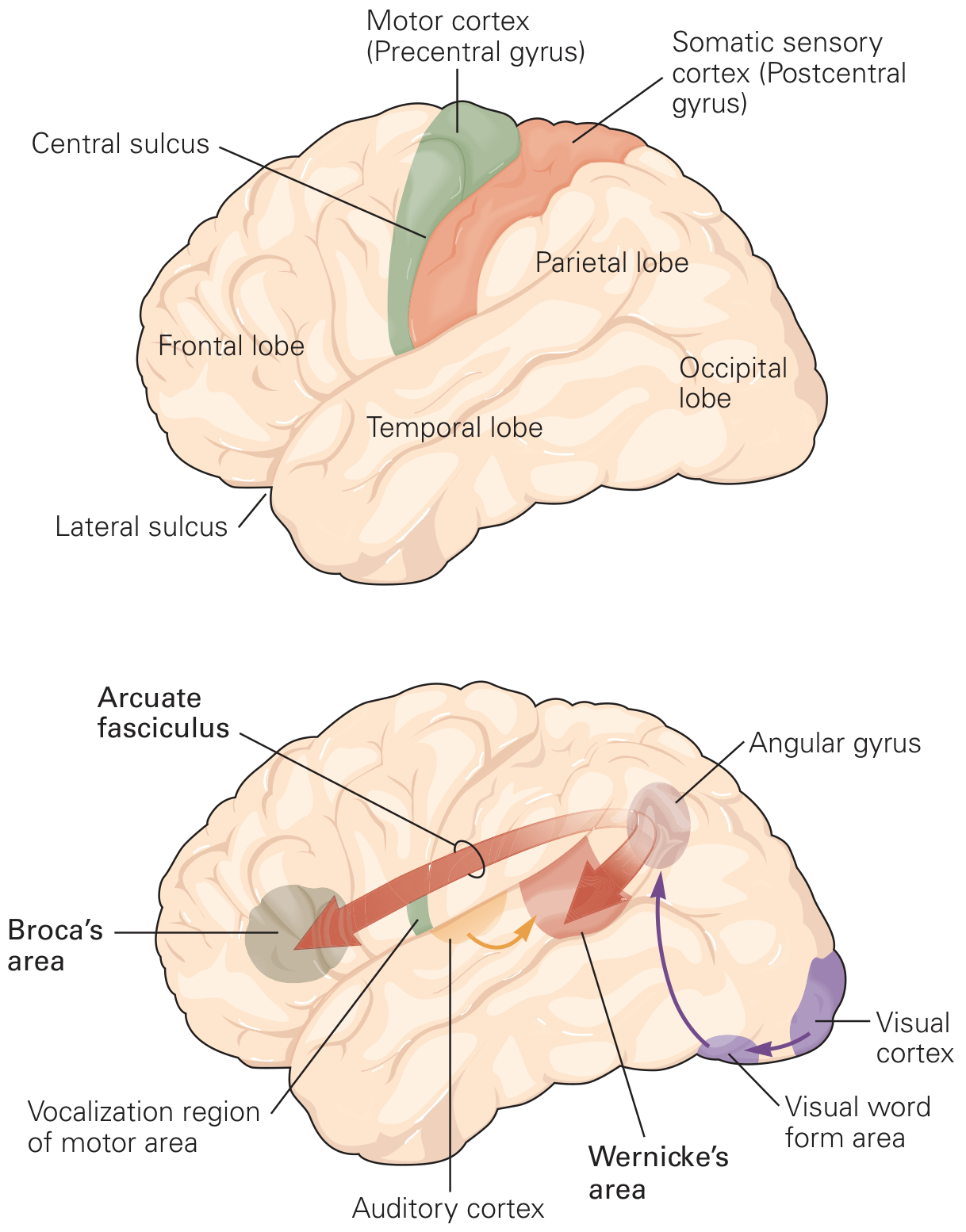
The lobes are separated by prominent grooves called sulci (singular: sulcus). The crests between them are gyri.
A. Frontal Lobe
The largest lobe — separated from the parietal lobe by the central sulcus.
| Area | Function |
|---|---|
| Prefrontal cortex | Executive function, decision-making, planning future actions, restraint of emotions, working (short-term) memory, personality |
| Primary motor cortex (precentral gyrus) | Controls voluntary movement on the contralateral side; organized as a motor homunculus (face inferior/lateral, legs superior/medial) |
| Broca's area (left posterior inferior frontal lobe) | Speech production — damage causes expressive (Broca's) aphasia: patient understands language but cannot produce fluent speech |
| Frontal eye fields | Voluntary eye movements |
B. Parietal Lobe
Located posterior to the frontal lobe, between the central sulcus and the occipital lobe.
| Area | Function |
|---|---|
| Primary somatosensory cortex (postcentral gyrus) | Receives and processes touch, pain, temperature, and proprioception from the contralateral body; arranged as a sensory homunculus |
| Association areas | Body image, spatial awareness, orientation of self in space, relating body to environment |
| Angular gyrus | Integration of visual and auditory information; reading; polymodal sensory processing |
C. Temporal Lobe
Located below the lateral sulcus (Sylvian fissure).
| Area | Function |
|---|---|
| Primary auditory cortex (Heschl's gyri) | Processing of sound and basic auditory information |
| Wernicke's area (left posterior superior temporal gyrus) | Language comprehension — damage causes receptive (Wernicke's) aphasia: fluent but meaningless speech; poor comprehension |
| Inferior temporal cortex | Recognition of faces and objects |
| Hippocampus (deep, medial temporal) | Explicit (declarative) memory formation and consolidation — new learning |
| Amygdala (deep, medial temporal) | Emotional responses, fear, emotional memory; connects to hypothalamus for autonomic emotional responses |
D. Occipital Lobe
The most posterior lobe.
| Area | Function |
|---|---|
| Primary visual cortex (V1 — along calcarine fissure) | Receives raw visual input from the retina (via thalamus) |
| Visual association areas (V2–V5) | Color perception, motion detection, depth, object recognition |
Two visual pathways:
- "Where" pathway (dorsal — parietal): spatial location and movement
- "What" pathway (ventral — temporal): object and face recognition
2. Diencephalon ("Between Brain")
Thalamus
- The sensory and motor relay station of the brain
- Almost all sensory information going to the cortex, and motor information coming from the cortex to the brainstem/spinal cord, passes through the thalamus
- Specific thalamic nuclei relay specific modalities (e.g., lateral geniculate nucleus → vision; medial geniculate nucleus → hearing; VPL nucleus → body sensation)
Hypothalamus
- Lies below the thalamus
- Master regulator of homeostasis:
- Body temperature regulation
- Food intake and satiety
- Water balance (thirst, ADH secretion)
- Circadian rhythms and sleep-wake cycles
- Endocrine control — secretes releasing/inhibiting hormones controlling the pituitary gland (the "master endocrine gland")
- Autonomic regulation; emotional and sexual behaviour
3. Limbic System
A group of interconnected structures forming an inner ring around the brainstem.
Mnemonic: HOME
- Homeostasis — hypothalamus
- Olfaction — olfactory cortex
- Memory — hippocampus
- Emotions and drives — amygdala, cingulate gyrus
| Structure | Function |
|---|---|
| Hippocampus | Explicit/declarative memory (facts and events); spatial navigation |
| Amygdala | Fear, emotional learning, threat detection; modulates autonomic responses via hypothalamus |
| Cingulate gyrus | Attention, motivation, error detection, pain processing |
| Hypothalamus | Drives (hunger, thirst, sex, aggression), autonomic and endocrine integration |
| Olfactory cortex | Primary processing of smell — the only sense that bypasses the thalamus |
4. Basal Ganglia
Deep nuclei of the cerebral hemispheres: caudate nucleus, putamen, globus pallidus, substantia nigra, subthalamic nucleus.
- Form the extrapyramidal motor system
- Function in initiation, selection, and smooth execution of voluntary movement
- Suppress unwanted movements
- Role in habit formation and procedural learning
- Dopamine (from substantia nigra → striatum) is essential for normal basal ganglia function
- Dysfunction: Parkinson's disease (dopamine deficiency → tremor, rigidity, bradykinesia), Huntington's disease (chorea), dystonia
5. Brainstem
Connects the cerebral hemispheres to the spinal cord. Comprises three parts:
| Part | Key Functions |
|---|---|
| Midbrain (mesencephalon) | Control of eye movements (CN III, IV); auditory and visual relay nuclei; contains substantia nigra and red nucleus (motor) |
| Pons | Balance and posture (with medulla); relays cerebellar information; respiratory regulation; CN V, VI, VII, VIII nuclei |
| Medulla oblongata | Vital centres: respiratory control, cardiovascular (heart rate + blood pressure) control; swallowing, coughing, vomiting reflexes; CN IX–XII nuclei |
The brainstem also houses the Reticular Activating System (RAS) — a diffuse network responsible for consciousness, arousal, and sleep-wake cycles. Damage to the RAS causes coma.
Cranial nerve nuclei III–XII are located in the brainstem.
6. Cerebellum ("Little Brain")
Located in the posterior fossa, attached to the dorsal pons and medulla.
| Function |
|---|
| Coordination of movement — smooth, accurate, well-timed |
| Maintenance of posture and balance |
| Motor learning (e.g., learning to ride a bike) |
| Coordination of head and eye movements |
The cerebellum integrates:
- Sensory position information (from spinal cord)
- Motor commands (from cerebral cortex)
- Balance information (from vestibular organs of the inner ear)
Damage: ataxia (uncoordinated movement), intention tremor, dysdiadochokinesia, nystagmus, dysarthria.
Quick Reference Summary
| Region | Key Functions |
|---|---|
| Frontal lobe | Executive function, voluntary movement, speech production (Broca's) |
| Parietal lobe | Somatosensory processing, body awareness, spatial orientation |
| Temporal lobe | Hearing, speech comprehension (Wernicke's), face/object recognition, memory |
| Occipital lobe | Vision |
| Thalamus | Sensory and motor relay station |
| Hypothalamus | Homeostasis, endocrine control, autonomic regulation |
| Hippocampus | Explicit memory, new learning |
| Amygdala | Emotion, fear, emotional memory |
| Basal ganglia | Movement initiation/selection, habit learning |
| Brainstem | Consciousness (RAS), vital functions (breathing, HR, BP), cranial nerve reflexes |
| Cerebellum | Movement coordination, balance, motor learning |
Sources: Principles of Neural Science, 6e (Kandel) | Costanzo Physiology, 7e | Schwartz's Principles of Surgery, 11e | Barash Clinical Anesthesia, 9e | Bradley and Daroff's Neurology in Clinical Practice | Neuroanatomy through Clinical Cases, 3e
This is a shared conversation. Sign in to Orris to start your own chat.