Alopecia types and patterns
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
Reading File
Finding Sources
I now have comprehensive material. Let me compile the full answer.
Alopecia: Types and Patterns
Alopecia (hair loss) is classified into two broad categories based on whether or not the hair follicle is permanently destroyed.
PRIMARY CLASSIFICATION: Scarring vs. Non-Scarring
| Feature | Non-Scarring (Non-Cicatricial) | Scarring (Cicatricial) |
|---|---|---|
| Follicle preserved? | Yes | No - replaced by fibrosis |
| Follicular openings | Present | Absent or reduced |
| Reversibility | Often reversible | Permanent |
| Key examples | AGA, telogen effluvium, AA | LPP, CCCA, FD, discoid lupus |
Harrison's Principles of Internal Medicine 22E, p. 2070
I. NON-SCARRING ALOPECIAS
1. Androgenetic Alopecia (AGA) - Pattern Alopecia
The most common cause of hair loss, affecting up to 80% of men and 50% of women during their lifetime. It is driven by DHT-mediated miniaturization of terminal hairs into vellus hairs. Both prevalence and severity increase with age. The parietal and occipital areas are typically spared.
Pathophysiology: 5α-reductase converts testosterone to DHT in scalp follicles. DHT triggers progressive shortening of the anagen phase, follicular miniaturization, and increased telogen shedding. Androgen-inducible TGF-β1 from dermal papilla cells suppresses hair growth. Castration before puberty prevents male-pattern baldness entirely.
Male-Pattern (Hamilton-Norwood Classification)
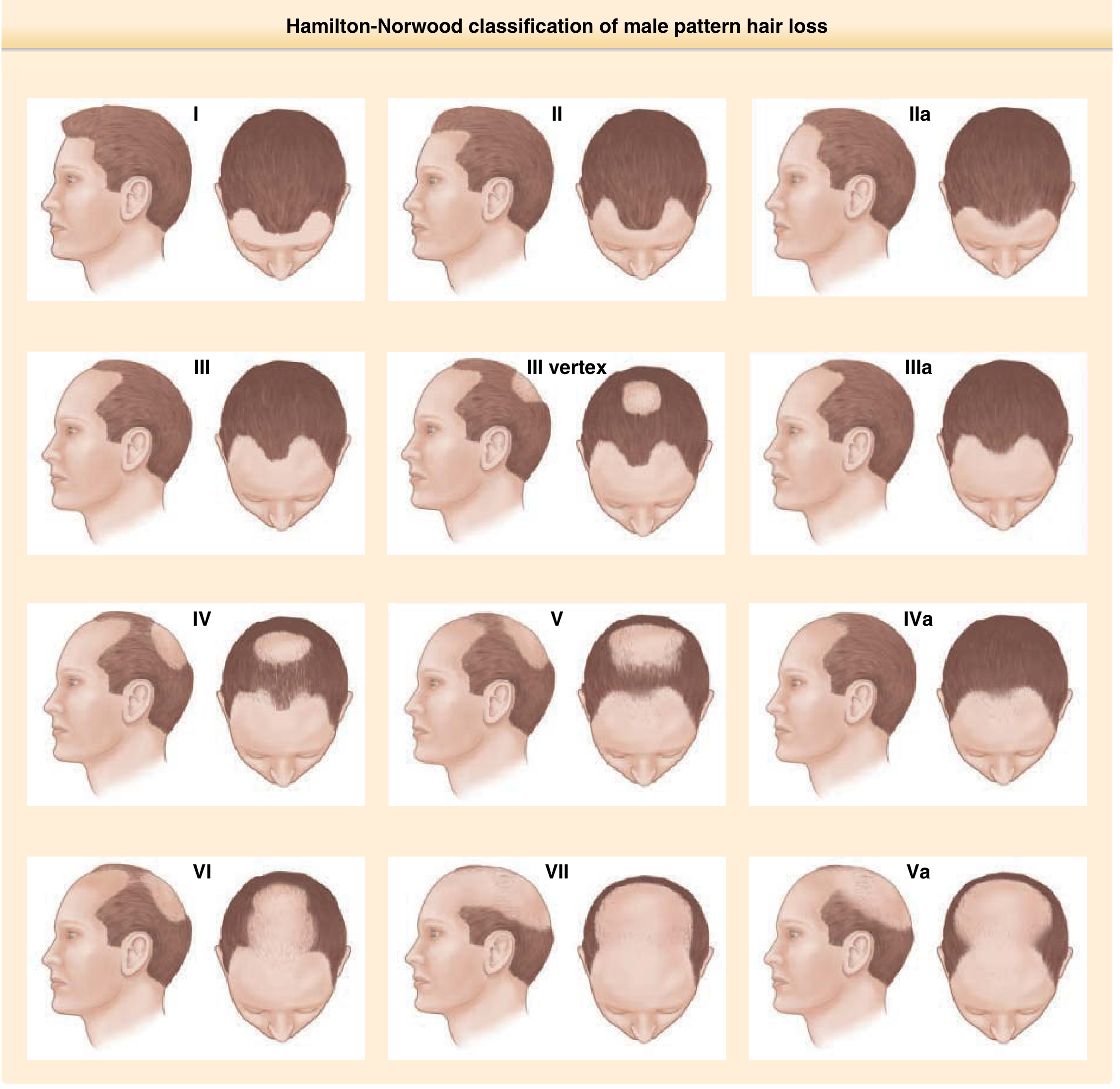
Hamilton-Norwood Classification - Fitzpatrick's Dermatology
- Begins in teens/twenties with recession at frontotemporal regions ("Geheimratswinkeln" / professor angles)
- Progresses to vertex thinning, then confluence over the crown
- Grades I-VII, with vertex-predominant and frontoparietal variants
- Follicles produce progressively finer, lighter hairs with each cycle
Female-Pattern (Ludwig / Sinclair Classification)

Female pattern AGA (Grade III, Ludwig) - Fitzpatrick's Dermatology
- Ludwig pattern (most common): diffuse centroparietal thinning with preservation of the frontal hairline. Graded I-III (Ludwig) or I-V (Sinclair scale).
- Christmas-tree pattern (Olsen): hair part widens anteriorly, creating a triangular zone of thinning pointing toward the frontal hairline.
- A small subset shows a male-type temporal recession pattern.
- Most women have normal menses and fertility; if hirsutism, menstrual irregularities, or acne are present, evaluate for hyperandrogenism (PCOS, adrenal/ovarian tumor).
Andrews' Diseases of the Skin, p. 872; Fitzpatrick's Dermatology, p. 1525
Treatment: Topical minoxidil (both sexes), finasteride 1 mg/day (men), dutasteride (men), spironolactone/cyproterone acetate (women), low-dose oral minoxidil, hair transplantation.
2. Telogen Effluvium
Excessive shedding of telogen (club) hairs, typically 3-5 months after a triggering event that prematurely converts anagen hairs to telogen. The hair is lost "at the root" with a visible depigmented club-shaped bulb.
Common triggers:
- Surgery, high fever, severe illness
- Parturition (postpartum hair loss) - hair shed 3-5 months after delivery
- Crash dieting / protein deficiency
- Drugs: warfarin, heparin, beta-blockers, lithium, retinoids, propylthiouracil, interferons, colchicine
- Thyroid disease (hypothyroidism and hyperthyroidism)
- Iron deficiency
Patterns:
- Acute telogen effluvium: typically resolves within 6 months
- Chronic telogen effluvium: shortened anagen phase persists (>6 months); associated with pattern alopecia
- Diffuse hair thinning without a specific distribution
Diagnosis: Pull test - >4-6 club hairs from 40 hairs grasped = positive. Normal daily loss is ~100-150 hairs; telogen effluvium causes 150-400+/day.
Andrews' Diseases of the Skin, p. 870
3. Alopecia Areata (AA)
A chronic, immune-mediated (T cell-driven), non-scarring hair loss disorder. CD8+ cytotoxic T cells and IFN-γ target the anagen hair bulb, causing premature catagen transition. The hair follicle bulge (stem cell region) is spared, explaining why regrowth is possible.
Clinical patterns:
| Pattern | Description |
|---|---|
| Patchy | One or more well-circumscribed oval/round patches, most common |
| Totalis | Complete loss of scalp hair |
| Universalis | Complete loss of all body hair (scalp + body) |
| Ophiasis | Band-like loss along the temporal/occipital margin (worse prognosis) |
| Sisaipho (inverse ophiasis) | Spares the occipital band |
| Diffuse AA | Diffuse shedding without distinct patches (mimics telogen effluvium) |
Key clinical features:
- Exclamation mark hairs (tapered/broken at the scalp end) at the patch margins
- Nail pitting in ~20% of cases
- Associated with thyroiditis, vitiligo, and other autoimmune diseases
- Positive family history in ~25% of cases
Treatment: Topical/intralesional/systemic corticosteroids, topical minoxidil, JAK inhibitors (baricitinib, ritlecitinib - FDA approved), contact immunotherapy (DPCP/SADBE).
Fitzpatrick's Dermatology, p. 229
4. Anagen Effluvium
Acute, diffuse loss of anagen hairs - typically caused by agents that abruptly interrupt active hair growth.
- Chemotherapy (daunorubicin, taxanes, anthracyclines) - most common cause; hair loss within 1-2 months of high-dose therapy
- Radiation to the scalp
- Severe protein malnutrition, arsenic/thallium poisoning
Hair loss is usually reversible after stopping the agent; however, taxane/anthracycline regimens can cause persistent chemotherapy-induced alopecia, which may benefit from topical or oral minoxidil.
5. Tinea Capitis
Dermatophyte infection of the scalp, particularly in children. Produces patchy hair loss with scaling; hairs break off at the surface ("black dot" pattern with endothrix infection). Treated with systemic antifungals (griseofulvin, terbinafine).
6. Traction Alopecia
Prolonged mechanical tension on hair follicles from tight hairstyles (braids, weaves, ponytails, dreadlocks, topknots in Sikh boys). Initially non-scarring and reversible; chronic traction leads to follicular atrophy and permanent cicatricial alopecia. More common in African American women. Distribution is typically along the frontal hairline and temples.
7. Trichotillomania (Hair-Pulling Disorder)
Self-induced hair loss from compulsive hair pulling. Clinically distinctive: asymmetric, geometrically shaped patches with short/bristly anagen hairs (not smoothly devoid as in AA). Hairs of varying lengths present. Treatment targets underlying psychopathology.
8. Pressure Alopecia
Hair loss following prolonged immobility/unconsciousness due to ischemia from pressure. May be permanent.
II. SCARRING (CICATRICIAL) ALOPECIAS
In cicatricial alopecia, the follicular bulge is destroyed by inflammation and replaced by fibrotic tissue, causing permanent hair loss. Clinically: smooth scalp, absent follicular openings.
Classified as primary (follicle is the target) or secondary (follicle is collateral damage).
A. LYMPHOCYTIC PRIMARY CICATRICIAL ALOPECIAS
1. Lichen Planopilaris (LPP)
- Predominant in White women, age 40-60
- Perifollicular scaling, erythema, burning/itching
- Targets the isthmus-bulge region (lymphocytic infiltrate)
- Trichoscopy: perifollicular scale, absent follicular openings
- Spectrum includes:
- Classic LPP: patchy occipital/vertex involvement
- Frontal Fibrosing Alopecia (FFA): progressive recession of the frontal and temporal hairline; loss of eyebrows/eyelashes; also affects Asian and African-heritage women
- Graham Little-Piccardi-Lasseur Syndrome: triad of scalp cicatricial alopecia + non-scarring axillary/pubic alopecia + follicular keratosis of the trunk/limbs
2. Central Centrifugal Cicatricial Alopecia (CCCA)
- Most common scarring alopecia in Black women
- Begins at the crown/vertex, expands centrifugally
- Associated with hot combs, chemical relaxers, and certain hair care practices (though causation is debated)
- Histology: premature desquamation of the inner root sheath
3. Discoid Lupus Erythematosus (DLE)
- Erythematous plaques with adherent scale; central atrophy and hypopigmentation with a rim of hyperpigmentation
- Active inflammation at periphery, scarring at center
- Can occur isolated to skin or with systemic lupus (minority)
4. Alopecia Mucinosa (Follicular Mucinosis)
- Well-demarcated erythematous/skin-colored patches; follicular papules; mucin deposition in outer root sheath
- Not a true primary cicatricial alopecia (no fibrotic scar)
- Must rule out underlying cutaneous T-cell lymphoma / mycosis fungoides
B. NEUTROPHILIC PRIMARY CICATRICIAL ALOPECIAS
1. Folliculitis Decalvans (FD)
- ~11% of primary cicatricial alopecias; young-middle aged adults, slight male predominance
- Starts at vertex: erythematous patches + follicular pustules (Staphylococcus aureus)
- Tufted folliculitis: 5-15 hairs emerging from a single dilated orifice - pathognomonic
- Treatment: prolonged antibiotics (rifampicin + clindamycin combination), topical antiseptics
2. Dissecting Cellulitis of the Scalp
- Deep, fluctuant nodules/abscesses on the vertex/occipital scalp
- Part of the follicular occlusion tetrad (with acne conglobata, hidradenitis suppurativa, pilonidal sinus)
C. MIXED CICATRICIAL ALOPECIAS
Erosive Pustular Dermatosis of the Scalp - pustules, erosions, and crusts; mainly elderly.
D. SECONDARY CICATRICIAL ALOPECIAS
The follicle is destroyed as "innocent bystander." Causes include:
- Deep burns
- Radiation dermatitis
- Cutaneous malignancies / metastases
- Sarcoidosis
- Morphea (linear scleroderma)
- Necrobiosis lipoidica
- Cutaneous tuberculosis
- Chronic pressure/ischemia
Dermatology 2-Volume Set 5e, p. 1404; Fitzpatrick's Dermatology, p. 393; Harrison's 22E, p. 2080
QUICK REFERENCE SUMMARY
| Type | Scarring? | Key Pattern | Reversible? |
|---|---|---|---|
| Male AGA | No | Frontotemporal → vertex | With treatment |
| Female AGA | No | Centroparietal (frontal hairline spared) | With treatment |
| Telogen effluvium | No | Diffuse | Usually yes |
| Alopecia areata | No | Patchy, totalis, universalis, ophiasis | Often yes |
| Anagen effluvium | No | Diffuse (acute) | Usually yes |
| Tinea capitis | No | Patchy with scale/black dots | Yes |
| Traction alopecia | Late: yes | Frontal/temporal margins | Early: yes |
| Trichotillomania | No | Asymmetric, bizarre shapes | Yes |
| Lichen planopilaris | Yes | Vertex, FFA = frontal band | No |
| CCCA | Yes | Vertex → centrifugal | No |
| Discoid lupus | Yes | Irregular plaques | No |
| Folliculitis decalvans | Yes | Vertex + pustules/tufts | No |
| Alopecia areata (AA) | No | Exclamation hairs, nail pitting | Variable |
Sources: Harrison's Principles of Internal Medicine 22E | Andrews' Diseases of the Skin | Fitzpatrick's Dermatology Vol 1-2 | Dermatology 2-Volume Set 5e (Elsevier)
Hypo pigmentation patches is seen in
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Now I have comprehensive textbook data. Let me compile the full answer.
Hypopigmentation Patches - Causes and Classification
Hypopigmented patches result from reduced (but not absent) melanin in the skin, as opposed to depigmentation (complete absence). They are classified by distribution and etiology.
MASTER CLASSIFICATION (Harrison's 22E, Table 61-9)
I. Primary Cutaneous Disorders
A. Diffuse
- Generalized vitiligo
B. Localized / Patchy
- Postinflammatory hypopigmentation
- Idiopathic guttate hypomelanosis
- Pityriasis (tinea) versicolor
- Vitiligo
- Chemical- or drug-induced leukoderma (e.g., topical imiquimod, oral imatinib)
- Nevus depigmentosus / Blaschko-linear hypopigmentation (pigmentary mosaicism)
- Progressive macular hypomelanosis
- Piebaldism
II. Systemic Diseases
A. Diffuse
- Oculocutaneous albinism (OCA types I-VII)
- Hermansky-Pudlak syndrome (+ platelet storage defect, lung disease)
- Chédiak-Higashi syndrome (+ giant lysosomal granules, recurrent infections)
- Phenylketonuria (tyrosine deficiency reduces melanin synthesis)
B. Localized / Patchy
- Systemic sclerosis (scleroderma) - perifollicular pigment retained
- Melanoma-associated vitiligo-like leukoderma
- Sarcoidosis (overlying cutaneous lesions)
- Cutaneous T-cell lymphoma / Mycosis fungoides (hypopigmented MF variant)
- Tuberculoid and indeterminate leprosy
- Onchocerciasis ("leopard skin")
- Blaschko-linear hypopigmentation (pigmentary mosaicism)
- Incontinentia pigmenti (Stage IV)
- Tuberous sclerosis (ash-leaf spots)
- Waardenburg syndrome / Shah-Waardenburg syndrome
- Vogt-Koyanagi-Harada (VKH) syndrome
Harrison's Principles of Internal Medicine 22E, p. 440
KEY CONDITIONS IN DETAIL
1. Vitiligo
- Loss of melanocytes (autoimmune T-cell mediated destruction)
- Well-demarcated, chalk-white (truly depigmented) patches
- Distribution: periorificial (mouth, eyes, nose), hands, feet, flexor wrists, ankles, elbows, knees, body folds
- Associated: Hashimoto's thyroiditis (most common - up to 30%), Graves' disease, Addison's disease, pernicious anemia, alopecia areata, uveitis
- Wood's lamp: bright white fluorescence (accentuates depigmentation)
- Treatment: topical ruxolitinib (JAK inhibitor), tacrolimus, corticosteroids, phototherapy (NB-UVB)
2. Pityriasis (Tinea) Versicolor
- Malassezia furfur (yeast) infection - produces azelaic acid which inhibits melanin synthesis
- Fine, scaly, hypopigmented (or hyperpigmented) macules/patches on the trunk, upper arms, neck
- Wood's lamp: yellow-green fluorescence
- KOH: "spaghetti and meatballs" (hyphae + spores)
- Treatment: topical/oral azoles, selenium sulfide
3. Pityriasis Alba
- Common in children/adolescents; associated with atopic dermatitis
- Ill-defined, slightly scaly, hypopigmented patches on the face (cheeks), upper arms
- Post-inflammatory; improves with emollients and low-potency topical steroids
4. Leprosy (Hansen's Disease) - Tuberculoid / Indeterminate Type
- Few asymmetric hypopigmented patches with well-defined or ill-defined edges
- Key distinguishing feature: associated anesthesia, anhidrosis, and alopecia within the patch
- Palpable thickened peripheral nerves at borders
- Biopsy: dermal granulomas with very few/no bacilli (tuberculoid); sparse lymphocytic infiltrate (indeterminate)
- Must be differentiated from: pityriasis alba, vitiligo, progressive macular hypomelanosis, tinea versicolor, pityriasis rosea, sarcoidosis
5. Tuberous Sclerosis - Ash-Leaf Spots
- Earliest cutaneous sign of tuberous sclerosis (often present at birth)
- Lance-ovate (ash-leaf) or polygonal hypopigmented macules, 1-3 cm
- Pigment reduced (not absent); may need Wood's lamp examination in fair-skinned patients
- ≥3 hypopigmented macules ≥5 mm = major diagnostic criterion
- Associated: angiofibromas ("adenoma sebaceum"), shagreen patches, ungual fibromas, seizures, intellectual disability, CNS hamartomas, renal angiomyolipomas
6. Postinflammatory Hypopigmentation
- Follows any inflammatory skin disease: eczema, psoriasis, lichen planus, discoid lupus, impetigo, pityriasis rosea, chemical burns, laser therapy
- Distribution follows that of the primary disease
- Usually temporary and reversible
7. Idiopathic Guttate Hypomelanosis
- Most common cause of guttate (drop-like) hypopigmentation
- Well-demarcated white macules, 2-4 mm on sun-exposed skin (shins, forearms)
- Seen in adults >40 years, increases with age and UV exposure
- Benign, no treatment usually required
8. Progressive Macular Hypomelanosis
- Young adults, especially darker skin tones
- Non-scaly, ill-defined coalescing hypopigmented macules on trunk (centrifugally spreading)
- Associated with Cutibacterium acnes follicular colonization
- Wood's lamp: follicular red fluorescence
9. Nevus Depigmentosus
- Stable, congenital, well-circumscribed hypomelanotic patch (usually single)
- Present at birth; does NOT enlarge proportionally with age
- Normal melanocyte number, but abnormal melanosomes/transfer
- Multiple lesions → rule out tuberous sclerosis
10. Piebaldism
- Autosomal dominant; c-KIT mutation → defective melanoblast migration
- Congenital, stable white patches + white forelock (poliosis)
- Characteristic distribution: anterior scalp/forehead, mid-trunk, mid-limbs
- Associated with Waardenburg syndrome (+ sensorineural deafness, dystopia canthorum)
11. Oculocutaneous Albinism (OCA)
- Autosomal recessive; mutations in tyrosinase (Type I) or OCA2/P protein (Type II)
- Generalized diffuse hypopigmentation of skin, hair, and eyes
- Complications: ↓ visual acuity, nystagmus, photophobia, ↑ risk of squamous cell carcinoma
12. Systemic Sclerosis (Scleroderma)
- "Salt-and-pepper" pattern - hypopigmentation with retention of perifollicular pigment
- Distinguishes it from vitiligo
13. Hypopigmented Mycosis Fungoides (CTCL)
- Variant of cutaneous T-cell lymphoma - more common in darker-skinned individuals
- Hypopigmented, slightly atrophic patches; can mimic pityriasis versicolor or vitiligo
- Biopsy with epidermotropic atypical T-cell infiltrate confirms diagnosis
14. Vogt-Koyanagi-Harada (VKH) Syndrome
- Granulomatous uveitis + cutaneous/hair depigmentation (vitiligo-like) + neurological and auditory features
- Poliosis (white patches of hair), perilimbal vitiligo (Sugiura sign)
QUICK DIFFERENTIATOR TABLE
| Condition | Sensation | Scale | Margins | Special Feature |
|---|---|---|---|---|
| Vitiligo | Normal | None | Well-defined, chalk-white | Periorificial; autoimmune associations |
| Leprosy (tuberculoid) | Absent (anesthetic) | None | Raised/well-defined | Anhidrosis, nerve thickening |
| Tinea versicolor | Normal | Fine | Ill-defined | KOH: spaghetti & meatballs |
| Pityriasis alba | Normal | Fine | Ill-defined | Children, face, atopy |
| Ash-leaf (tuberous sclerosis) | Normal | None | Well-defined | Present at birth; lance-ovate |
| Nevus depigmentosus | Normal | None | Well-defined | Stable, congenital |
| Postinflammatory | Normal | Variable | Follows prior lesion | History of inflammation |
| Piebaldism | Normal | None | Well-defined | White forelock, congenital |
| IGH (idiopathic guttate) | Normal | None | Well-defined, 2-4 mm | Elderly, sun-exposed sites |
| Scleroderma | Variable | None | Perifollicular pigment retained | Sclerosis, Raynaud's |
Sources: Harrison's Principles of Internal Medicine 22E | Andrews' Diseases of the Skin | Goldman-Cecil Medicine | Fitzpatrick's Dermatology Vol 1-2
This is a shared conversation. Sign in to Orris to start your own chat.