
Screenshot_20260624_154712_Xodo.jpg
Complain of orangish urine with AST ALT 2226 and 493
Reading File
analyse_media
Finding Sources
Finding Sources
Searching PubMed
rhabdomyolysis management acute kidney injury
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is a complete clinical analysis of this case.
Clinical Analysis: Mr. Aryan Pujari, 26-year-old Male
Critical Lab Values (from the report)
| Parameter | Value | Reference Range | Significance |
|---|---|---|---|
| CK (CPK) | >42,670 U/L (Critical High) | 30-200 U/L | >213x upper limit |
| AST | 2,226 U/L (from clinical history) | ~10-40 U/L | Grossly elevated |
| ALT | 493 U/L (from clinical history) | ~7-56 U/L | Markedly elevated |
Diagnosis: RHABDOMYOLYSIS with Myoglobinuria
The triad of findings in this 26-year-old male is essentially diagnostic:
-
Orangish/tea-colored urine - this is myoglobinuria. Myoglobin, released from lysed muscle cells, appears in urine when plasma myoglobin exceeds 100-300 mg/L, manifesting as tea-colored or brown-orange urine. A urine dipstick will test positive for blood with few or no RBCs on microscopy - this distinguishes myoglobinuria from hematuria.
-
Massively elevated CK >42,670 U/L - this is the most reliable diagnostic marker for rhabdomyolysis. The lab has flagged this as a Critical High value (>213x upper limit of normal).
-
Markedly elevated transaminases (AST 2226, ALT 493) - in rhabdomyolysis, AST rises disproportionately to ALT because AST is present in both liver AND skeletal muscle. The AST:ALT ratio of ~4.5:1 seen here is characteristic of muscle injury rather than primary liver disease. (In hepatocellular damage from hepatitis, AST:ALT is typically close to 1:1 or the ALT may exceed AST.)
Pathophysiology
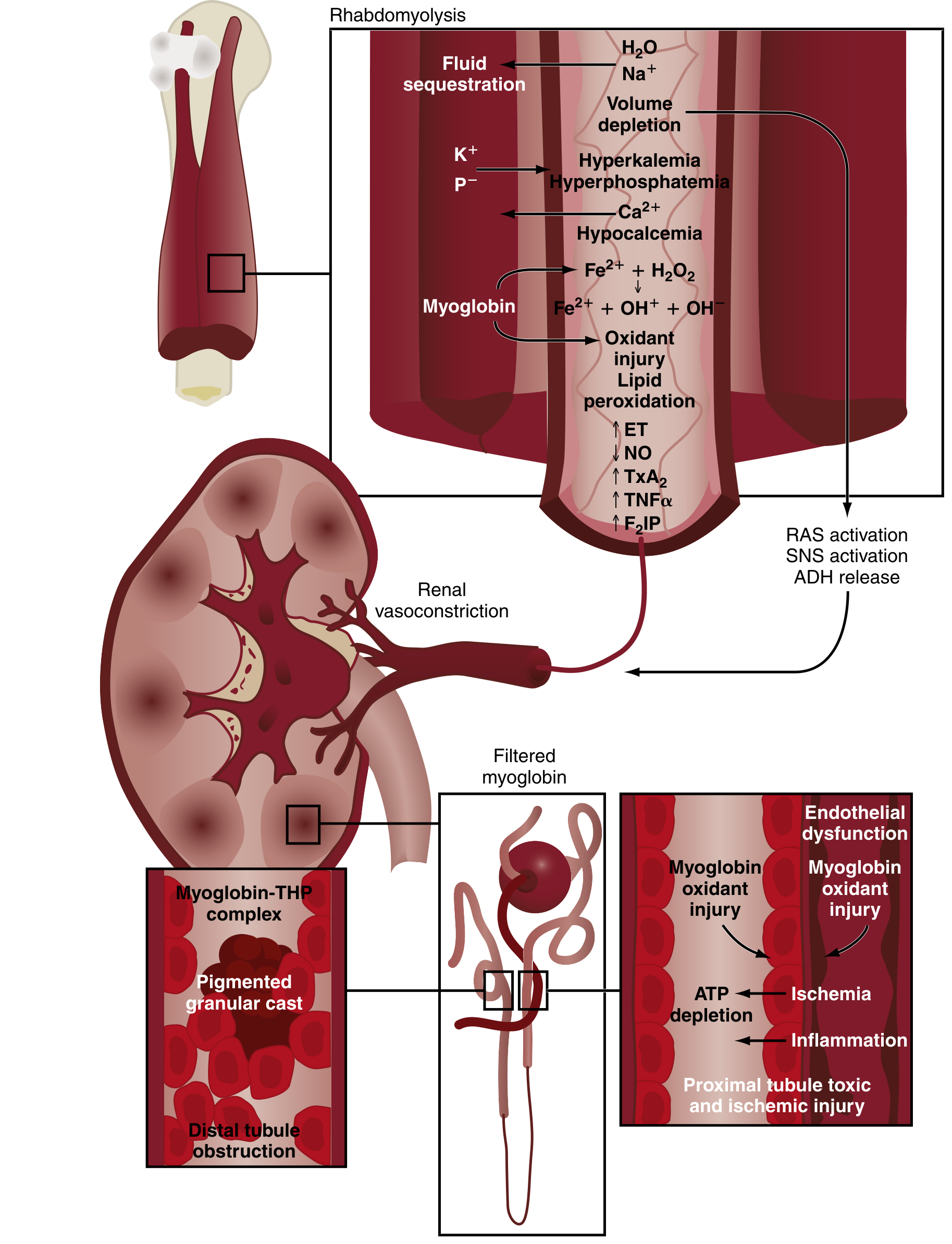
Muscle cell destruction releases myoglobin into circulation. Filtered myoglobin causes kidney injury via three mechanisms:
- Tubular obstruction - myoglobin complexes with Tamm-Horsfall protein forming pigmented granular casts that block distal tubules
- Direct tubular toxicity - myoglobin's iron (Fe²+) generates hydroxyl radicals via the Fenton reaction, causing lipid peroxidation and oxidant injury to proximal tubule cells
- Renal vasoconstriction - volume depletion from fluid sequestration into necrotic muscle activates RAS, SNS, and ADH, reducing GFR
(Rosen's Emergency Medicine, p. 2555)
Likely Causes to Investigate in a 26-Year-Old Male
Acquired causes (more likely at this age):
| Category | Examples |
|---|---|
| Exertional | Intense exercise, status epilepticus, prolonged immobilization |
| Drugs/toxins | Statins, cocaine, amphetamines, alcohol, synthetic cannabinoids, antipsychotics |
| Infections | Influenza A/B, EBV, HIV, COVID-19 |
| Metabolic | Hypokalemia, hypophosphatemia, hypernatremia, DKA, hypothyroidism |
| Crush/ischemia | Compartment syndrome, prolonged pressure (immobility/intoxication) |
| Inflammatory | Polymyositis, dermatomyositis |
| Heat-related | Exertional heatstroke, hyperthermia |
(Goldman-Cecil Medicine, Table 99-1)
Given his age and CK >40,000, exertional rhabdomyolysis, drug/substance use (cocaine, amphetamines, MDMA), or a viral illness are the highest-priority etiologies to explore.
Urgent Workup Needed
- Renal function: Serum creatinine, BUN, eGFR, electrolytes (look for hyperkalemia, hyperphosphatemia, hypocalcemia - the classic triad)
- Urine: Dipstick (positive for blood despite no/few RBCs), myoglobin casts, urinalysis
- Urine output monitoring - oliguria = early AKI
- ECG - for hyperkalemia-related arrhythmias
- LDH, uric acid, coagulation panel (DIC screen if severe)
- Blood glucose, TFTs, electrolyte panel
- History: Exercise, substance use, medications (statins, antipsychotics), trauma, fever, viral illness
Management (Emergency)
This patient needs URGENT HOSPITALIZATION.
1. Aggressive IV fluid resuscitation (most important intervention)
- Normal saline (0.9% NaCl) initially: 1-1.5 L/hour until urine output reaches 200-300 mL/hr
- Target urine output: 200-300 mL/hour
- Volume expansion increases renal blood flow, GFR, and dilutes myoglobin in tubules
2. Treat the underlying cause (identify and eliminate)
3. Electrolyte correction
- Hyperkalemia: treat aggressively (calcium gluconate for cardiac protection, insulin/dextrose, sodium bicarbonate, Kayexalate, dialysis if refractory)
- Hypocalcemia: treat only if symptomatic (do NOT give empiric calcium - can worsen muscle calcification)
4. Urinary alkalinization (controversial, consider if pH <6.5)
- Sodium bicarbonate to raise urine pH >6.5 may reduce myoglobin cast formation and tubular toxicity, but evidence is mixed
5. Renal replacement therapy (RRT/dialysis) - needed in up to 20% if:
- Uncorrectable metabolic acidosis
- Life-threatening hyperkalemia refractory to medical management
- Uremia with oliguria/anuria despite fluid expansion
Red Flags Requiring ICU Admission
- Hemodynamic instability
- Hyperkalemia (K+ >6.5 mEq/L) with ECG changes
- Oliguria/anuria despite fluids
- Evidence of DIC
- CK not trending down with treatment
Prognosis
With early recognition and aggressive fluid resuscitation, rhabdomyolysis carries an excellent prognosis. Most patients with AKI fully recover renal function. Mortality is rare in isolated rhabdomyolysis without severe comorbidities. (Rosen's Emergency Medicine, p. 2557)
Bottom line: This is a critical alert - the patient must be admitted immediately. The orangish urine + sky-high CK + elevated AST >> ALT together confirm rhabdomyolysis with myoglobinuria. The AST elevation is from muscle (not liver), and ALT elevation is secondary. Aggressive IV hydration must begin at once to prevent acute kidney injury. A recent 2026 narrative review in Chest (PMID 41619932) provides updated management guidance.
which specialist to consult for this cas3
Based on the clinical picture (rhabdomyolysis with CK >42,670, myoglobinuria, and elevated transaminases), here are the specialists to consult, in order of priority:
Specialist Consultations for This Case
🔴 Primary / Most Urgent
1. Nephrologist (Kidney Specialist)
- Highest priority - AKI from myoglobinuria is the most life-threatening complication
- Will guide aggressive fluid management, monitor renal function trajectory, and decide if dialysis/RRT is needed
- CK >40,000 in a 26-year-old with orangish urine = nephrology consult should happen within hours
🟠 Essential Secondary Consults
2. Internal Medicine / Hospitalist
- Coordinates overall care and admission
- Manages electrolyte abnormalities (hyperkalemia, hypocalcemia, hyperphosphatemia)
- Oversees fluid resuscitation protocol
- If not already in a hospital, this is the team that admits and manages the case
3. Emergency Medicine (if presenting to ER)
- First point of contact for stabilization
- Initiates IV fluids, ECG monitoring, and urgent labs before specialist handover
🟡 Situational Consults (Based on Etiology Found)
| If suspected cause | Consult |
|---|---|
| Drug/substance use (cocaine, amphetamines) | Toxicology |
| Inflammatory myopathy (polymyositis) | Rheumatologist |
| Viral illness (influenza, EBV, HIV) | Infectious Disease |
| Inherited metabolic myopathy (e.g., McArdle disease) | Neurologist / Neuromuscular specialist |
| Exertional + recurrent episodes | Sports Medicine + Neurologist |
| Statin-induced | Cardiologist (to re-evaluate statin need) |
| Elevated ALT 493 persisting after muscle injury resolves | Gastroenterologist/Hepatologist (to rule out concurrent liver disease) |
🔵 Regarding the AST/ALT
The AST 2226 and ALT 493 are very likely muscle-origin (AST:ALT ratio ~4.5:1 is typical of rhabdomyolysis). However, if the ALT remains persistently elevated after CK normalizes, a Gastroenterologist or Hepatologist consult is warranted to exclude concurrent hepatic pathology.
Summary Priority Order
1. Nephrology (urgent - AKI prevention/management)
2. Internal Medicine (admission, overall coordination)
3. Etiology-directed specialist (once cause identified)
This is a medical emergency - the patient should not be managed outpatient. Hospital admission with nephrology involvement from day one is the standard of care for CK values at this level.
Urine color normalised after hydration and kft is normal
This is excellent news and very reassuring. Here is what it means clinically:
Clinical Interpretation: Urine Normalized + KFT Normal
What This Tells You
| Finding | Meaning |
|---|---|
| Urine color normalized | Myoglobin successfully cleared from circulation and urine - kidneys are filtering effectively |
| KFT (kidney function) normal | Renal tubules were NOT significantly injured - AKI was avoided |
| Both together | The most feared complication of rhabdomyolysis has been successfully prevented |
The fluid resuscitation worked exactly as intended - it diluted myoglobin, maintained GFR, and flushed the tubules before irreversible damage occurred.
What to Do Now
Continue Monitoring (Do NOT discharge yet)
1. Serial CK every 12-24 hours
- CK should trend downward with each reading
- If CK is still rising, muscle injury is ongoing - investigate further
- Target: CK trending down toward <5,000 U/L before considering discharge
2. Repeat KFT in 24-48 hours
- A single normal KFT is reassuring but not sufficient
- Myoglobin can continue to be released for days if cause is not eliminated
- Renal function can deteriorate even after initial normalization
3. Electrolytes (daily)
- Potassium (K+) - watch for late hyperkalemia
- Phosphate, calcium - monitor for shifts
4. Urine output - maintain >0.5 mL/kg/hour
Shift Focus: Find the Cause
Now that the acute crisis is stabilized, identifying the underlying etiology becomes the priority - especially important in a 26-year-old because:
- Recurrent rhabdomyolysis can cause cumulative renal damage
- An inherited metabolic myopathy (McArdle disease, CPT-II deficiency) could be missed if not investigated
- A reversible/treatable cause (drug, infection, inflammatory) must be identified and eliminated
Ask specifically:
- Any intense exercise or physical activity in the 24-72 hours before?
- Any drugs - prescription, OTC, recreational (cocaine, MDMA, amphetamines, alcohol)?
- Any fever, viral illness, muscle pain in the days before?
- Any family history of similar episodes or muscle disease?
- Any medications started recently (statins, antipsychotics)?
- Was this a first episode or has it happened before?
Discharge Criteria (when safe to discharge)
- CK trending clearly downward (does not need to be normal, but falling)
- KFT consistently normal on repeat testing
- Urine remains clear
- Electrolytes stable
- Underlying cause identified and addressed
- No muscle compartment syndrome signs (limb swelling, pain out of proportion)
Bottom Line
The patient is doing well - normal KFT and cleared urine after hydration is the best possible early response. This is now a stable but monitored situation rather than a crisis. The priority shifts to:
- Serial CK trending to confirm ongoing improvement
- Identifying the cause to prevent recurrence
- Outpatient follow-up with nephrology or internal medicine once safely discharged
Dietary recommendation for this patient
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Here are the dietary recommendations tailored specifically for this patient - a 26-year-old male recovering from rhabdomyolysis with normalized KFT and clearing urine. Since his kidneys have been spared, the diet is less restrictive than it would be with established AKI, but still requires care during recovery.
Dietary Recommendations: Rhabdomyolysis Recovery
Phase 1 - Acute Recovery (While Still Admitted / First 3-5 Days)
🥤 Fluids - Most Important Component
| Recommendation | Detail |
|---|---|
| High oral fluid intake | 2.5 - 3.5 litres per day minimum (oral + IV combined) |
| Best fluids | Water, diluted fruit juices, oral rehydration solutions, coconut water (in moderation) |
| Urine color target | Pale yellow - the patient's own urine color is the best guide |
| Avoid | Alcohol (direct myotoxin, worsens dehydration), energy drinks (caffeine causes vasoconstriction), carbonated sugary drinks |
The goal is to keep urine dilute and flowing to prevent myoglobin from re-precipitating in tubules.
🥩 Protein - Moderate, Not High
- Do NOT push high protein during acute phase - even with normal KFT, the kidneys are under metabolic stress
- Aim for 0.8-1.0 g/kg/day (normal maintenance level) - approximately 60-80g protein/day for a typical adult male
- Best sources: eggs, lean chicken, fish, low-fat dairy, lentils, tofu
- Avoid: protein supplements, whey shakes, creatine supplements - these increase nitrogen load on kidneys and can worsen uric acid production
CK elevation releases large amounts of purines from muscle nucleic acids, leading to hyperuricemia. High-protein/purine foods worsen this.
🫀 Potassium - Moderate Caution
Even with normal KFT now, muscle breakdown releases large amounts of intracellular potassium. Until CK is trending down clearly:
Temporarily limit high-potassium foods:
- Bananas, oranges, kiwi, avocado
- Potatoes, tomatoes, spinach, beans
- Salt substitutes (contain KCl)
- Coconut water in excess (high K+)
Safe choices: white rice, pasta, bread, apples, pears, cucumber, carrots
🦴 Phosphate - Mild Restriction
Muscle lysis also dumps phosphate into blood (hyperphosphatemia). Limit temporarily:
- Processed foods, cola drinks, packaged snacks (contain phosphate additives)
- Red meat in large amounts
- Nuts and seeds in excess
🧂 Sodium - Normal to Slightly Liberal
Since the patient is recovering and KFT is normal, sodium restriction is NOT needed. In fact, adequate sodium intake supports continued good urine output. IV normal saline used for hydration reflects this principle.
Phase 2 - Recovery at Home (After Discharge, Weeks 1-4)
✅ Encourage
| Food Group | Examples | Reason |
|---|---|---|
| Hydrating foods | Cucumber, watermelon, soups, broths | Maintain urine dilution |
| Antioxidant-rich | Berries, leafy greens, tomatoes, bell peppers | Counter oxidative muscle damage |
| Complex carbohydrates | Rice, oats, sweet potato, whole wheat | Provide muscle glycogen fuel |
| Lean protein (moderate) | Chicken, fish, eggs, dal, paneer | Muscle tissue repair |
| Magnesium-rich | Dark leafy greens, nuts (in moderation), whole grains | Supports muscle function and enzyme activity |
| Anti-inflammatory foods | Turmeric, ginger, omega-3 from fish | Reduce ongoing muscle inflammation |
❌ Avoid / Restrict Long-Term
| Avoid | Reason |
|---|---|
| Alcohol | Direct myotoxin - can trigger recurrence of rhabdomyolysis |
| Creatine / protein supplements | Increases kidney workload; creatine directly raises serum creatinine |
| Statins (if applicable) | Known rhabdomyolysis trigger |
| Excessive caffeine | Vasoconstriction, dehydration |
| Energy drinks | Combination of caffeine + stimulants - reported rhabdomyolysis trigger |
| Fasting / crash dieting | Causes metabolic stress that can precipitate muscle breakdown |
Special Consideration: If Cause Was Exertional
If this was exercise-induced rhabdomyolysis (very common in young males who exercise intensely):
- No exercise at all for at least 2-4 weeks until CK normalizes
- When returning to exercise: gradual progressive loading only - no sudden intense sessions
- Pre-exercise hydration is essential going forward
- Avoid exercising in hot weather or while unwell
Summary Card
DRINK: 3+ litres of water daily - pale urine is the goal
EAT: Moderate lean protein, complex carbs, antioxidant vegetables
LIMIT: High-potassium and high-phosphate foods (short-term)
AVOID: Alcohol, energy drinks, protein supplements, creatine
STOP: All intense exercise until CK normalized
FOLLOW: Repeat CK and KFT in 1-2 weeks after discharge
A formal dietitian referral is worth considering at discharge, particularly if an inherited metabolic myopathy (like McArdle disease) is suspected - those patients need very specific dietary strategies tailored to their enzyme deficiency.
This is a shared conversation. Sign in to Orris to start your own chat.