What is osteoporosis
Reading File
Finding Sources
Searching PubMed
osteoporosis
Finding Sources
Searching Images
osteoporosis bone loss trabecular structure
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Here is a comprehensive overview of osteoporosis based on authoritative medical textbooks:
Osteoporosis
Definition
Osteoporosis is the most prevalent metabolic bone disease, characterized by reduced bone mass and microarchitectural deterioration of bone tissue, leading to increased bone fragility and fracture risk. It is defined by a T-score ≤ −2.5 standard deviations below peak bone mass on dual-energy X-ray absorptiometry (DXA).
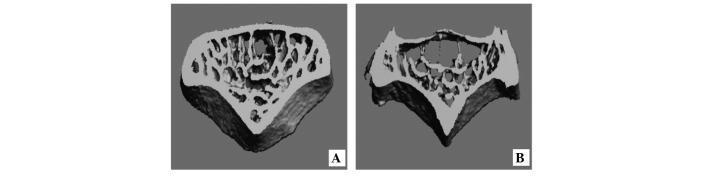
Bone Structure: Normal vs. Osteoporotic
The image below shows micro-CT scans of vertebral bone: (A) healthy bone with a dense, interconnected trabecular network, versus (B) osteoporotic bone with sparse trabeculae, enlarged marrow spaces, and loss of connectivity.
Epidemiology & Impact
- Causes 1.5 million fractures per year in the United States
- At age 50, women have a ~40% lifetime risk of fracture (vertebra, hip, or distal forearm); men ~one-third of that
- Hip fracture carries up to 20% mortality within 6 months; 25% of survivors require long-term nursing home care
- Annual US medical costs approach $20 billion
- One-third of women over 65 suffer vertebral crush fractures; up to 50% of mild vertebral fractures are clinically silent
Pathophysiology
Bone mass normally peaks around age 30, then slowly declines after age 40 in both sexes. The key imbalance is:
- Normal: bone formation (osteoblasts) coupled with bone resorption (osteoclasts) → stable mass
- After age 40: resorption slightly exceeds formation → ~0.5% skeletal mass lost per year
- Postmenopause: estrogen loss dramatically accelerates bone loss to 2–3% per year
Because trabecular bone (found in vertebrae, distal forearm) turns over at 5–7× the rate of cortical bone, fractures of these sites occur earlier in life. Hip fractures (predominantly cortical bone) occur later.
Risk Factors
Primary (non-modifiable):
- Advanced age
- Female sex
- Postmenopausal estrogen deficiency
- Family history of osteoporosis
Secondary causes (modifiable or treatable):
| Category | Examples |
|---|---|
| Endocrine | Cushing syndrome, hyperthyroidism, hyperparathyroidism, hypogonadism, diabetes |
| Bone marrow disorders | Multiple myeloma, leukemia, mastocytosis |
| Immobilization | Long-term bed rest, paraplegia, cerebral palsy |
| Malabsorption | Celiac disease, postgastrectomy, gastric bypass, chronic liver disease |
| Collagen defects | Osteogenesis imperfecta, Marfan syndrome |
| Inflammatory | Rheumatoid arthritis, inflammatory bowel disease |
| Drugs | Glucocorticoids (most common), aromatase inhibitors, androgen deprivation, anticonvulsants, heparin, SSRIs, PPIs, thiazolidinediones, alcohol |
Diagnosis
Bone Mineral Density (BMD)
- DXA scan is the gold standard
- T-score: compares BMD to young healthy adult peak
- ≥ −1.0 → Normal
- −1.0 to −2.5 → Osteopenia
- ≤ −2.5 → Osteoporosis
Laboratory Workup
Performed when osteoporosis is inconsistent with age/sex (e.g., middle-aged man, premenopausal woman) to exclude secondary causes:
- Thyroid function (TSH)
- Cortisol (rule out Cushing syndrome)
- PTH and calcium (hyperparathyroidism)
- Testosterone (hypogonadism in men)
- Protein electrophoresis (myeloma)
Bone Turnover Markers
- Formation: Serum P1NP (procollagen type I N-terminal propeptide), osteocalcin
- Resorption: Plasma CTX (C-terminal telopeptide)
- The International Osteoporosis Foundation recommends serum P1NP and plasma CTX as reference markers for monitoring therapy
Treatment
Non-pharmacological
- High calcium intake: 1000–1500 mg/day
- Adequate vitamin D: 400–800 IU/day
- Regular weight-bearing exercise
- Fall prevention strategies
Pharmacological
Antiresorptive agents (reduce osteoclast activity):
- Bisphosphonates: alendronate, risedronate, ibandronate, zoledronate (FDA-approved first-line)
- Denosumab: humanized monoclonal antibody against RANKL
- Raloxifene: selective estrogen receptor modulator (SERM)
- Estrogen: slows early postmenopausal bone loss (used primarily for menopausal symptoms)
Anabolic agents (stimulate bone formation):
- Teriparatide (recombinant PTH 1–34): stimulates osteoblasts
- Abaloparatide: PTHrP analog with anabolic action
- Romosozumab: humanized sclerostin antibody — increases bone formation (↑P1NP, ↑ALP) while decreasing resorption (↓CTX); FDA and EMA approved
Prevention
Prevention begins at puberty and continues throughout life:
- Adequate calcium and vitamin D intake
- Regular exercise
- Avoiding smoking and excess alcohol
- Managing medications that accelerate bone loss (especially glucocorticoids)
Key Takeaway
Osteoporosis is a silent disease until a fracture occurs. It results from an imbalance between bone resorption and formation, accelerated by estrogen deficiency, aging, and numerous secondary causes. Early screening with DXA, lifestyle modification, and targeted pharmacotherapy can significantly reduce fracture risk and associated morbidity.
Sources: Tietz Textbook of Laboratory Medicine, 7th Ed., p. 2194–2195 | Goldman-Cecil Medicine, p. 2567
Recent evidence update: A 2024 meta-analysis (PMID 39312040) confirmed that teriparatide and denosumab are superior to bisphosphonates for treatment-naive osteoporosis patients. A 2025 systematic review (PMID 39487940) further supports romosozumab as an effective emerging option for high-fracture-risk patients.
This is a shared conversation. Sign in to Orris to start your own chat.