Explain acute bronchitis in detail with treatment
Reading File
Finding Sources
Searching PubMed
"acute bronchitis" treatment management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have rich, comprehensive material from four authoritative textbooks. Let me compose the detailed answer.
Acute Bronchitis
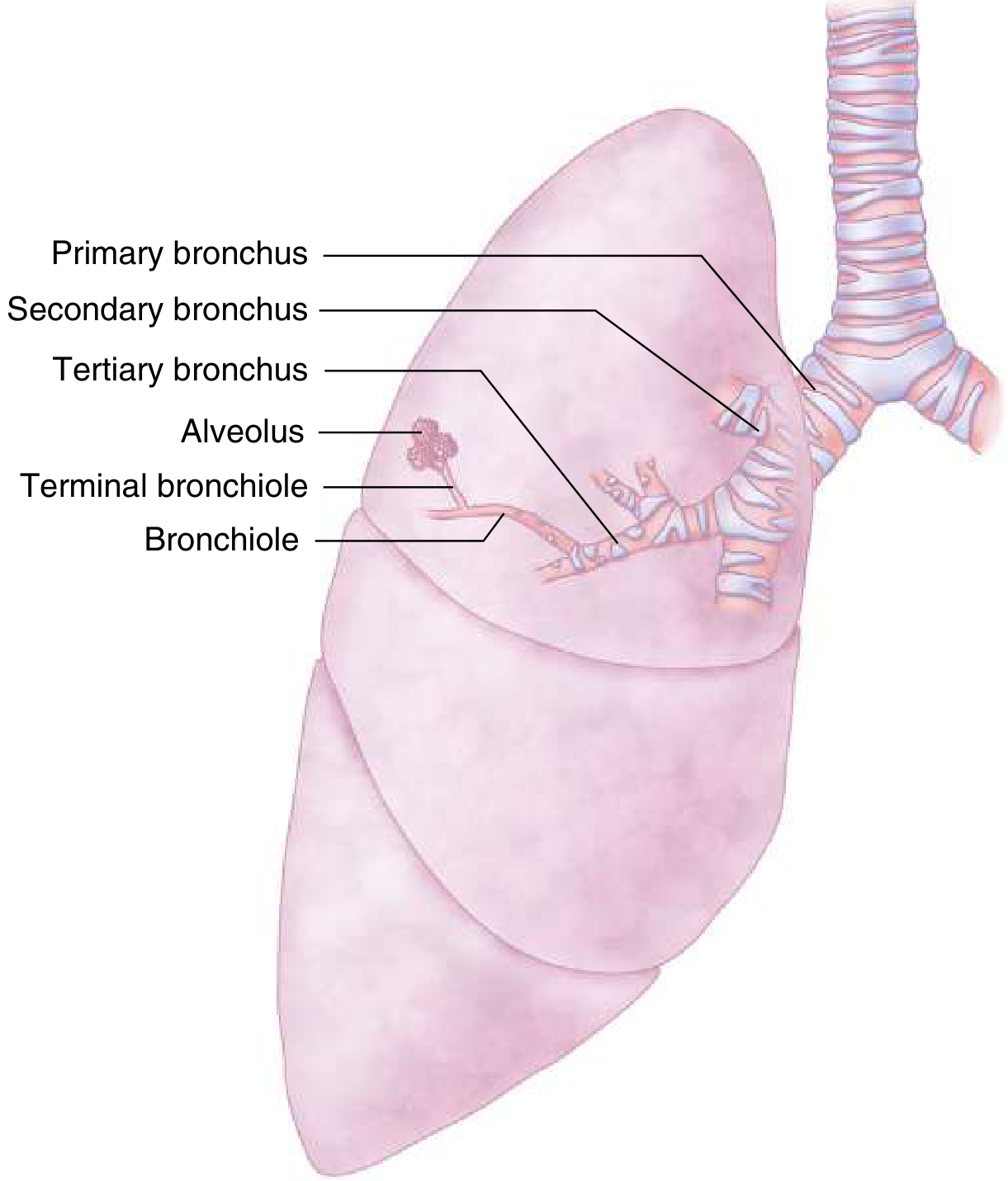
The image above shows the large airways (primary through tertiary bronchi) that are inflamed in acute bronchitis, extending down to the bronchioles - Goldman-Cecil Medicine.
Definition
Acute bronchitis (also called tracheobronchitis) is a self-limited inflammation of the large airways - from the trachea down to the tertiary bronchi - without evidence of pneumonia. The illness typically lasts 1 to 3 weeks. It is distinct from:
-
Bronchiolitis - involves the small airways
-
Chronic bronchitis - defined as productive cough for at least 3 months per year for 2 consecutive years
-
Bronchiectasis - associated with permanent bronchial dilation
-
Goldman-Cecil Medicine, p. 986
Epidemiology
-
Approximately 5% of adults develop acute bronchitis each year - a rate of 44 per 1000 adults annually
-
It is the 9th most common outpatient diagnosis in the United States and one of the 10 most common worldwide
-
Incidence is higher in fall and winter compared to spring and summer
-
In the US, consumers spend approximately $7 billion annually on cough management - the hallmark symptom
-
Despite being mostly viral, 60-90% of patients are given antibiotics - a major driver of antibiotic resistance
-
Fishman's Pulmonary Diseases, p. 1680; Tintinalli's Emergency Medicine, p. 478
Etiology and Pathogens
Viral (responsible for up to 90% of cases)
The following viruses are implicated, roughly in order of frequency:
| Virus | Notes |
|---|---|
| Influenza A and B | Most commonly identified; peaks in winter |
| Parainfluenza virus | Common in fall |
| Respiratory syncytial virus (RSV) | Common even during influenza season |
| Coronavirus (including SARS-CoV-2) | COVID-19 must be excluded |
| Adenovirus | Year-round |
| Human metapneumovirus | Increasingly recognized |
| Rhinovirus | Common cold pathogen, significant contributor |
Bacterial (6-25% of cases)
Bacteria are found much less often, and their pathogenic role is often unclear since bronchial biopsies do not show bacterial invasion:
Atypical bacteria (up to 25% of bacterial cases):
- Bordetella pertussis - important to recognize; causes characteristic paroxysmal cough
- Mycoplasma pneumoniae
- Chlamydia (Chlamydophila) pneumoniae
Typical bacteria (more common in COPD/smokers):
-
Haemophilus influenzae
-
Moraxella catarrhalis
-
Streptococcus pneumoniae
-
Goldman-Cecil Medicine, p. 987; Fishman's Pulmonary Diseases, p. 1682
Pathophysiology
Viral or bacterial infection of the bronchial and tracheal epithelium triggers an inflammatory response leading to:
- Microscopic thickening of bronchial and tracheal mucosa
- Airflow obstruction and bronchial hyperresponsiveness
- Decreased FEV1 (reversible) - a substantial proportion of patients show this during the acute illness
- Mucosal hypersecretion - sputum production (clear, white, yellow, or green - discoloration reflects cellular debris and microorganisms, not necessarily bacterial infection)
- Heightened cough reflex - due to inflammation of airway epithelium
These changes explain the persistent cough, wheezing, and dyspnea seen in many patients.
- Tintinalli's Emergency Medicine, p. 478
Clinical Features
Symptoms
- Cough (with or without sputum) - the cardinal symptom; persists 10-20 days on average, but can last over 1 month
- Low-grade fever (high fever is uncommon; if present, consider pneumonia)
- Mild dyspnea and wheezing
- Sputum production - up to half of patients have purulent sputum; this does not reliably indicate bacterial infection
- Headache, rhinorrhea, and mild constitutional symptoms (malaise, fatigue)
- Chest tightness or discomfort
Key Points on Sputum Color
Purulent (yellow/green) sputum is an unreliable marker of bacterial infection and should not alone trigger antibiotic prescribing. Discoloration is often due to cellular debris or dead neutrophils from a viral inflammatory process.
Pertussis - Special Features
Adults with B. pertussis infection may exhibit:
-
Paroxysms of coughing
-
Post-tussive vomiting
-
Inspiratory "whoop" (less common in adults than children)
-
Cough lasting weeks to months
-
Goldman-Cecil Medicine, p. 987; Washington Manual of Therapeutics, p. 538
Diagnosis
Diagnosis is clinical. There is no single definitive test.
Clinical Criteria
- Cough persisting >5 days (typically 1-3 weeks)
- No clinical or radiographic evidence of pneumonia
- Absence of systemic inflammatory response syndrome (SIRS) criteria makes pneumonia unlikely:
- Temp <36°C or >38°C
- Pulse >90 bpm
- Respiratory rate >20 breaths/min
- WBC <4,000 or >12,000 cells/µL or >10% bands
When to Get a Chest X-Ray
Indicated in febrile, systemically ill, or elderly patients with:
- Abnormal vital signs (tachycardia, tachypnea, hypoxia)
- Abnormalities on chest auscultation (crackles, absent breath sounds)
- Age >65 with comorbidities
Sputum Culture
Not recommended routinely.
Procalcitonin
- Level <0.1 ng/mL makes bacterial infection highly unlikely
- Limiting antibiotics to patients with levels >0.25 ng/mL can reduce antibiotic use
- Note: large RCTs (ProAct trial) failed to show significant reduction in antibiotic prescribing using procalcitonin in US emergency departments
Testing for Specific Pathogens
-
Pertussis: Nasopharyngeal swab for PCR - the most sensitive method (use calcium alginate swabs, not cotton); consider if cough persists >2 weeks
-
Mycoplasma/Chlamydophila: PCR of nasopharyngeal aspirate; routine testing generally not recommended due to cost
-
COVID-19: Must be ruled out in all patients
-
Goldman-Cecil Medicine, p. 987-988; Washington Manual, p. 538; Tintinalli's, p. 478
Treatment
Overview
Management is primarily supportive, given the self-limited viral nature of most cases. The goal is symptom relief and exclusion of dangerous alternative diagnoses.
1. Symptomatic / Supportive Measures
| Intervention | Evidence/Notes |
|---|---|
| Rest and hydration | Standard supportive care |
| Air humidification | May ease airway irritation |
| Antipyretic/analgesics (paracetamol/NSAIDs) | For fever and discomfort |
| Dextromethorphan 15 mg PO q6h | Antitussive; may provide modest cough relief |
| Guaifenesin (expectorant) | May provide modest benefit |
| Benzonatate | May provide modest cough relief |
| Honey | Some evidence in adults and children for symptom relief |
2. Bronchodilators (Beta-2 Agonists)
- Routine use is NOT recommended for uncomplicated acute bronchitis
- Exception: In patients with evidence of airflow obstruction (audible wheezing on exam), short-acting beta-2 agonists (e.g., salbutamol/albuterol) are associated with lower symptom scores and faster cough resolution
- No benefit in the absence of measurable airway obstruction
3. Corticosteroids
- Oral corticosteroids are NOT recommended in patients without a history of COPD or asthma
- Recent evidence shows no benefit in uncomplicated acute bronchitis
4. Antihistamines, Mucolytics, Expectorants
- Limited quality evidence for these agents
- May be considered for symptom relief on a case-by-case basis
- Not routinely recommended by major guidelines
5. Antibiotics - When to Use and When NOT to Use
The most important principle: Antibiotics should NOT be routinely prescribed for acute uncomplicated bronchitis.
Guidelines from the CDC, IDSA (Infectious Diseases Society of America), and other major professional societies uniformly recommend against antibiotics for acute uncomplicated bronchitis. The IDSA includes this as one of their five "Choosing Wisely" statements.
Evidence summary:
- Antibiotics provide approximately half a day of benefit (shorter cough duration, less fever)
- Adverse effects of antibiotic therapy offset the mild clinical benefit in aggregate
- Sputum color does not predict who will benefit from antibiotics
- Despite this, >60-70% of patients still receive antibiotics in clinical practice
When antibiotics ARE indicated:
| Indication | Preferred Antibiotic |
|---|---|
| Confirmed or suspected B. pertussis | Azithromycin 500 mg on Day 1, then 250 mg/day for 4 more days (5-day course) OR Clarithromycin 500 mg PO q12h for 14 days |
| Productive cough persisting >10-14 days in a smoker or patient with underlying pulmonary disease | Antibiotics may be considered to treat bacterial co-infection |
| Atypical bacteria confirmed by PCR (Mycoplasma, Chlamydophila) | Macrolide or tetracycline (doxycycline) |
Pertussis note: Cases must be reported to the local health department for contact tracing, and post-exposure prophylaxis with azithromycin should be given to contacts when indicated.
Antibiotic choice: When antibiotics are used, the specific choice has little impact. Studies comparing azithromycin with amoxicillin or amoxicillin-clavulanate show no significant advantage for the macrolide.
- Washington Manual of Therapeutics, p. 538-540; Fishman's Pulmonary Diseases, p. 1688-1692; Textbook of Family Medicine, p. 313
6. Influenza-Specific Treatment
If influenza is confirmed (rapid antigen test, PCR, or DFA) during influenza season:
- Oseltamivir (Tamiflu) or other neuraminidase inhibitors should be initiated, particularly for high-risk patients (elderly, immunocompromised, severe disease)
"Red Flag" Symptoms Requiring Urgent Re-evaluation
The following symptoms should trigger immediate reassessment for a more serious diagnosis:
- Hemoptysis
- Worsening dyspnea or hypoxia
- Persistent high fever (suggests pneumonia)
- Weight loss (consider malignancy or tuberculosis)
- Difficulty swallowing
- Cough persisting >8 weeks (warrants evaluation for post-infectious cough, asthma, GERD, or malignancy)
Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Pneumonia | Fever, tachycardia, tachypnea, crackles, CXR infiltrate |
| Asthma exacerbation | Known asthma, reversible obstruction, eosinophilia |
| COPD exacerbation | History of smoking/COPD, chronic baseline symptoms |
| Congestive heart failure | Orthopnea, PND, edema, bilateral crackles |
| Pertussis | Paroxysmal cough >2 weeks, post-tussive vomiting, whoop |
| Sinusitis | Facial pain/pressure, nasal discharge, headache |
| GERD | Nocturnal cough, heartburn, no fever |
Prognosis and Patient Counseling
- Acute bronchitis is self-limiting in healthy individuals
- Cough resolves in 10-20 days in most cases but can persist for up to 6 weeks
- Patients should understand that antibiotics will not speed recovery meaningfully and carry risk of side effects and resistance
- Patients with underlying lung disease (COPD, asthma) or smokers may be at higher risk for secondary pneumonia or COPD exacerbation and warrant closer follow-up
- Clinical re-evaluation should be planned if symptoms are persistent or progressive
Summary Table
| Feature | Details |
|---|---|
| Cause | Viral (~90%): influenza, RSV, rhinovirus, coronavirus; Bacterial: B. pertussis, Mycoplasma, Chlamydia |
| Hallmark symptom | Cough (with or without sputum), lasting 10-20 days |
| Diagnosis | Clinical; CXR if pneumonia suspected |
| Treatment | Supportive (rest, hydration, antipyretics, cough suppressants) |
| Antibiotics | NOT routinely indicated; use for pertussis or selected high-risk cases |
| Bronchodilators | Only if wheezing/airflow obstruction present |
| Corticosteroids | Not recommended (absent COPD/asthma) |
| Prognosis | Self-limited; full recovery expected in most |
Sources: Goldman-Cecil Medicine (Int'l Ed., 2-Vol Set) | Fishman's Pulmonary Diseases and Disorders | Tintinalli's Emergency Medicine | Washington Manual of Medical Therapeutics | Textbook of Family Medicine 9e
Explain a step wise approach in diagnosing a patient with cough with sputum chest tightness and mild fever with differential diagnosis investigations and treatment with brand names
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive, authoritative material. I have everything needed to construct a thorough stepwise clinical approach. Let me now compose the full answer.
Stepwise Approach to a Patient with Cough + Sputum + Chest Tightness + Mild Fever
STEP 1 - Initial Clinical Assessment (History)
The triad of productive cough + chest tightness + mild fever is a very common presentation that can represent anything from self-limited viral bronchitis to life-threatening pneumonia. The history is the most powerful diagnostic tool.
Key Questions to Ask
About the cough:
- Duration - acute (<3 weeks), subacute (3-8 weeks), or chronic (>8 weeks)?
- Productive or dry? What is the color, consistency, and volume of sputum?
- Hemoptysis?
- Time of day (nocturnal cough suggests asthma or GERD)
- Precipitating or relieving factors
About the chest tightness:
- Is it pleuritic (sharp, worse on inspiration) - suggests pneumonia/pleuritis/PE
- Is it tight/squeezing - suggests asthma or bronchitis
- Any associated chest pain or palpitations
About the fever:
- Degree and duration (mild low-grade vs. high spiking fever)
- Night sweats (suggests TB or lymphoma)
- Chills/rigors (suggests bacterial infection, bacteremia)
Red flag symptoms to ask about:
- Weight loss (TB, malignancy)
- Hemoptysis (TB, cancer, pulmonary embolism)
- Worsening dyspnea at rest
- Orthopnea/PND (heart failure)
- Difficulty swallowing (aspiration risk)
Past medical/social history:
-
Smoking history (COPD, lung cancer risk)
-
Known asthma or COPD
-
HIV/immunosuppression
-
TB contact or travel to endemic areas
-
Occupation (bird exposure = psittacosis; cooling towers = Legionella)
-
ACE inhibitor use (causes dry cough but not fever)
-
Recent hospitalization (HAP/HCAP risk)
-
Vaccination status (influenza, pneumococcal)
-
Alcohol use disorder (aspiration, Klebsiella)
-
Textbook of Family Medicine 9e, p. 310
STEP 2 - Physical Examination
Vital Signs First
| Parameter | Significance |
|---|---|
| Temperature >38°C | Suggests infection - bacterial more likely if high |
| HR >100 bpm | SIRS criterion, consider pneumonia |
| RR ≥20 breaths/min | SIRS criterion; ≥30 = severe pneumonia |
| SpO2 <92% on room air | Indication for hospitalization |
| BP (systolic ≤90 or diastolic ≤60) | CURB-65 criterion; may indicate severity |
Respiratory Examination
| Finding | Suggests |
|---|---|
| Bronchial breath sounds, dullness to percussion, increased vocal fremitus, egophony | Pneumonia (consolidation) |
| Diffuse wheeze, prolonged expiration | Asthma or COPD exacerbation |
| Diffuse rhonchi (clearing with cough) | Bronchitis |
| Bilateral fine basal crackles | Heart failure |
| Absent breath sounds unilaterally | Pleural effusion or pneumothorax |
| Pleural rub | Pleuritis/pleuropneumonia |
General Examination
- Level of consciousness/confusion (CURB-65 criterion)
- Cyanosis
- Use of accessory muscles (severe obstruction or respiratory failure)
- Signs of fluid overload (JVD, peripheral edema - heart failure)
- Lymphadenopathy (TB, lymphoma)
STEP 3 - Immediate Bedside Investigations
| Test | Purpose |
|---|---|
| Pulse oximetry | Immediate severity assessment; SpO2 <92% = admit |
| Peak flow rate (if wheezing) | Assess for asthma - reversible obstruction |
| Rapid COVID-19 antigen test | Rule out SARS-CoV-2 |
| Rapid influenza test | Rule out influenza (seasonal) |
STEP 4 - Differential Diagnosis
For cough + purulent sputum + chest tightness + mild fever, the major differentials are:
Primary Differentials
| Condition | Key Features |
|---|---|
| Acute Bronchitis | Viral, self-limited, normal SpO2, no consolidation on CXR, cough 10-20 days |
| Community-Acquired Pneumonia (CAP) | High fever, productive cough, pleuritic chest pain, crackles, CXR infiltrate |
| Acute Exacerbation of COPD | Known COPD/smoker, worsening dyspnea, change in sputum character |
| Acute Asthma Exacerbation | Chest tightness, diffuse wheeze, reversible obstruction, personal/family history |
| Influenza | Systemic myalgia, sudden-onset high fever, malaise, headache |
Secondary Differentials (must not miss)
| Condition | Key Features |
|---|---|
| Pulmonary Tuberculosis | Prolonged cough, night sweats, weight loss, hemoptysis, TB exposure |
| COVID-19 | Loss of smell/taste, positive rapid test, clusters |
| Pulmonary Embolism | Pleuritic chest pain, risk factors (DVT, recent surgery), tachycardia |
| Congestive Heart Failure | Bilateral crackles, orthopnea, edema, cardiomegaly on CXR |
| Bronchiectasis | Chronic productive (copious, foul) cough, recurrent infections |
| Lung Abscess | Foul-smelling sputum, aspiration risk, cavitation on imaging |
| Lung Cancer | Hemoptysis, weight loss, smoker, mass on CXR |
- Textbook of Family Medicine 9e, p. 310; Goldman-Cecil Medicine, p. 987
STEP 5 - Investigations
Tier 1 - Always Order
| Investigation | Interpretation |
|---|---|
| Chest X-Ray (PA + lateral) | Consolidation = pneumonia; hyperinflation = asthma/COPD; mass = cancer; cardiomegaly = CHF; clear = bronchitis |
| CBC with differential | WBC >12,000 or <4,000 = SIRS; neutrophilia = bacterial; lymphocytosis = viral; eosinophilia = asthma/allergy |
| C-Reactive Protein (CRP) | Elevated in bacterial infection; helps guide antibiotic use |
| SpO2 / ABG (if severe) | SpO2 <92% on room air = hospitalize; assess type of respiratory failure |
| Blood Urea Nitrogen (BUN)/Urea | CURB-65 criterion; BUN ≥20 mg/dL = 1 point |
Tier 2 - Order Based on Clinical Suspicion
| Investigation | When to Order |
|---|---|
| Sputum Gram stain + Culture | Admitted patients with CAP; not needed for outpatient bronchitis |
| Blood cultures x2 | Hospitalized CAP patients; prior to antibiotics |
| Procalcitonin | To distinguish bacterial vs. viral; <0.1 ng/mL = very unlikely bacterial; >0.25 ng/mL = guide antibiotic initiation |
| Urinary Legionella antigen | If Legionella suspected (recent travel, cooling tower exposure, cluster cases) |
| Urinary pneumococcal antigen | Hospitalized CAP patients |
| Rapid influenza PCR / antigen | Seasonal, within 48h of symptom onset |
| COVID-19 PCR | All respiratory presentations |
| Nasopharyngeal swab PCR for pertussis | If cough >2 weeks with paroxysms |
| Spirometry / Peak Flow | If wheezing/asthma suspected |
| LDH, ferritin, D-dimer | If PE or COVID-related pneumonitis suspected |
Tier 3 - Specialist/Second-Line
| Investigation | When to Order |
|---|---|
| CT Chest (HRCT) | Negative CXR but high clinical suspicion; evaluate for bronchiectasis, interstitial disease, pulmonary embolism (CT-PA) |
| Bronchoscopy + BAL | Immunocompromised patients; cavitary disease; failed empiric therapy; suspected malignancy |
| AFB smear + sputum for TB culture | Night sweats, weight loss, upper lobe infiltrate, high TB prevalence area |
| Echocardiogram | Suspected heart failure |
| HIV test | Recurrent infections, immunosuppressed appearance |
- Fishman's Pulmonary Diseases, p. 2202; Harrison's Principles, p. 446; Goldman-Cecil Medicine, p. 992
STEP 6 - Severity Scoring (for CAP)
Before deciding treatment site, apply a validated severity score:
CURB-65 Score (simple, bedside)
| Criterion | Score |
|---|---|
| C - Confusion (new onset) | 1 |
| U - Urea >7 mmol/L (BUN >20 mg/dL) | 1 |
| R - Respiratory rate ≥30/min | 1 |
| B - Blood pressure (systolic ≤90 or diastolic ≤60 mmHg) | 1 |
| 65 - Age ≥65 years | 1 |
Score interpretation:
- 0 - 30-day mortality 1.5% → Treat as outpatient
- 1-2 - Consider outpatient or short-stay/observation (especially if age alone drives the score)
- ≥3 - Mortality ~22% → Hospitalize; consider ICU
Additional ICU Admission Criteria (ATS/IDSA)
-
Septic shock requiring vasopressors
-
Acute respiratory failure requiring mechanical ventilation
-
Or ≥3 minor criteria: RR ≥30, PaO2/FiO2 ≤250, multilobar infiltrates, confusion, BUN ≥20, WBC <4000, platelets <100,000, hypothermia, hypotension needing fluids
-
Harrison's Principles of Internal Medicine 22E, p. 448
STEP 7 - Treatment
A. Acute Bronchitis (No Pneumonia on CXR, Normal Vital Signs)
Treatment is supportive - NO routine antibiotics.
| Drug | Brand Name | Dose | Role |
|---|---|---|---|
| Dextromethorphan | Robitussin DM, Delsym | 15-30 mg PO q6h | Antitussive |
| Guaifenesin | Mucinex, Robitussin | 200-400 mg PO q4h | Expectorant (thins mucus) |
| Benzonatate | Tessalon Perles | 100-200 mg PO TID | Antitussive |
| Paracetamol/Acetaminophen | Tylenol, Calpol | 500-1000 mg q6h PRN | Antipyretic/analgesic |
| Ibuprofen | Advil, Brufen | 400 mg q8h with food | Anti-inflammatory/antipyretic |
| Salbutamol inhaler (if wheezing) | Ventolin, ProAir | 2 puffs q4-6h PRN | Bronchodilator - only if airflow obstruction |
Pertussis exception (if confirmed/suspected):
- Azithromycin (Zithromax, Azee) - 500 mg on Day 1, then 250 mg/day for 4 more days
- OR Clarithromycin (Biaxin, Clarbact) - 500 mg q12h for 14 days
- Report to public health; give contacts post-exposure prophylaxis with azithromycin
B. Community-Acquired Pneumonia (CAP)
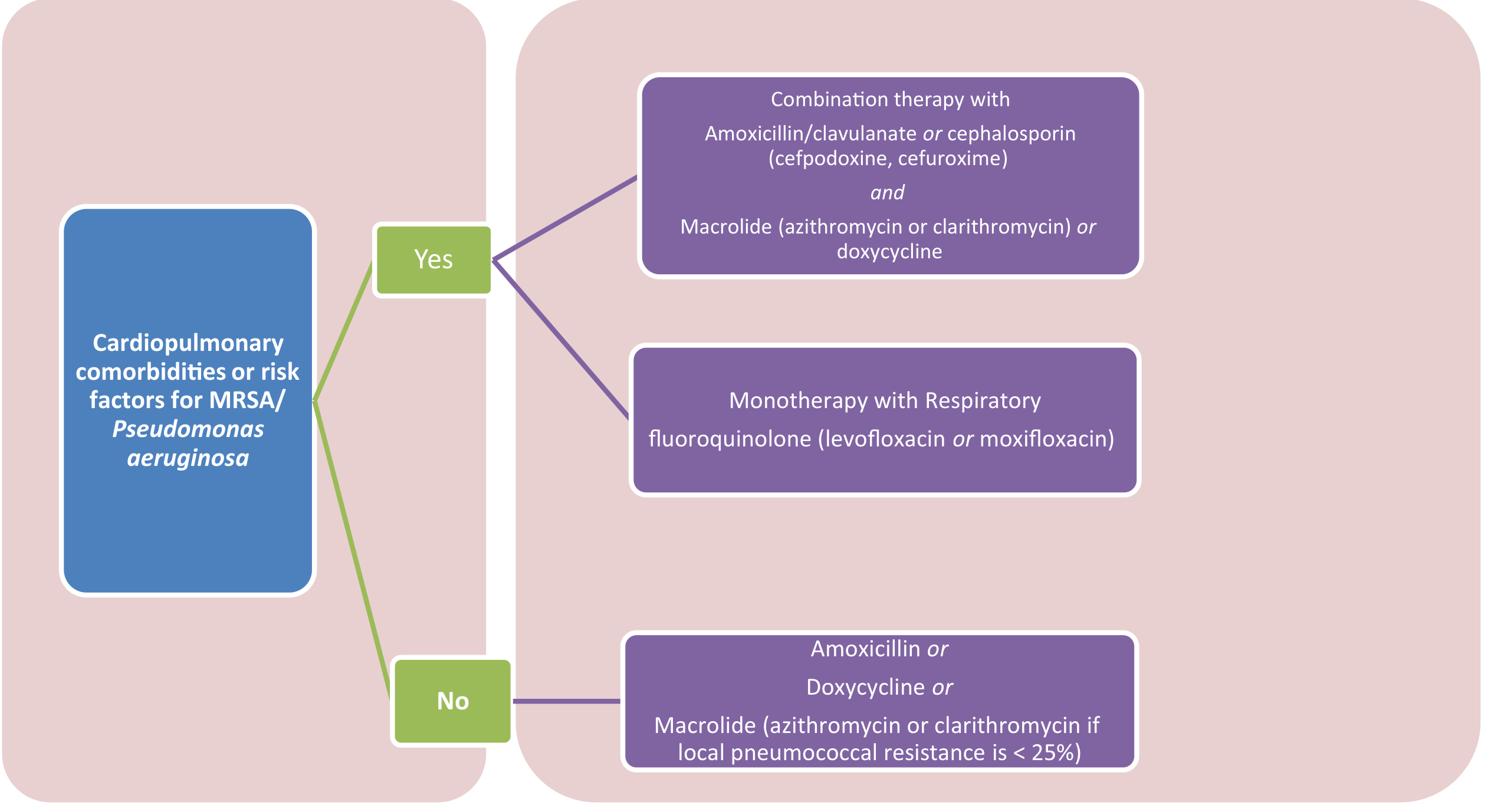
IDSA/ATS-guided antibiotic selection for outpatient CAP - Fishman's Pulmonary Diseases.
Outpatient CAP Treatment (CURB-65 score 0-1)
Healthy patient, no comorbidities, local macrolide resistance <25%:
| Drug | Brand Name | Dose | Duration |
|---|---|---|---|
| Amoxicillin | Amoxil, Trimox | 1 g PO TID | 5 days |
| Doxycycline | Vibramycin, Doryx | 100 mg PO q12h | 5 days |
| Azithromycin | Zithromax, Z-Pack | 500 mg Day 1, then 250 mg/day | 5 days |
| Clarithromycin | Biaxin, Clarbact | 500 mg PO q12h | 5-7 days |
| Clarithromycin ER | Biaxin XL | 1000 mg PO OD | 7 days |
With cardiopulmonary comorbidity (COPD, heart disease, diabetes, renal/hepatic disease, malignancy):
| Regimen | Drugs | Brand Names | Dose |
|---|---|---|---|
| Option 1 (Combination) | Amoxicillin-clavulanate + Macrolide | Augmentin + Azithromycin | 875/125 mg PO BD + 500 mg Day 1 then 250 mg/day |
| Option 1 alt | Cefpodoxime + Macrolide | Vantin + Azithromycin | 200 mg BD + macrolide |
| Option 1 alt | Cefuroxime + Macrolide | Ceftin, Zinnat + Azithromycin | 500 mg BD + macrolide |
| Option 2 (Monotherapy) | Levofloxacin | Levaquin, Levotas | 750 mg PO OD for 5 days |
| Option 2 alt | Moxifloxacin | Avelox, Moxiget | 400 mg PO OD for 5 days |
Inpatient (Non-ICU) CAP Treatment (CURB-65 score 2-3)
Standard regimen (no MRSA/Pseudomonas risk):
| Component | Drug | Brand Name | Dose |
|---|---|---|---|
| Beta-lactam | Ceftriaxone | Rocephin, Cefaxone | 1-2 g IV OD |
| OR | Cefotaxime | Claforan | 1-2 g IV q8h |
| OR | Ampicillin-sulbactam | Unasyn | 1.5-3 g IV q6h |
| PLUS macrolide | Azithromycin | Zithromax | 500 mg IV/PO OD |
| PLUS | Clarithromycin | Biaxin | 500 mg PO q12h |
| OR instead of combo | Levofloxacin | Levaquin | 750 mg IV/PO OD |
| OR | Moxifloxacin | Avelox | 400 mg IV/PO OD |
ICU/Severe CAP Treatment (CURB-65 ≥3 + organ dysfunction)
All patients must receive combination therapy:
-
Beta-lactam (ceftriaxone, cefotaxime, or ceftaroline) PLUS respiratory fluoroquinolone (levofloxacin or moxifloxacin)
-
If MRSA suspected: Add Vancomycin (Vancocin) 15-20 mg/kg IV q8-12h, OR substitute with Linezolid (Zyvox) 600 mg IV q12h
-
If Pseudomonas suspected: Use Piperacillin-tazobactam (Zosyn, Tazact) 4.5 g IV q6h + ciprofloxacin/aminoglycoside
-
Fishman's Pulmonary Diseases, p. 2203-2204
C. Acute Exacerbation of COPD/Asthma
| Drug | Brand Name | Dose |
|---|---|---|
| Salbutamol (SABA) | Ventolin, ProAir | 2.5 mg nebulized q20min x3, then q1-4h |
| Ipratropium bromide | Atrovent | 0.5 mg nebulized q6h |
| Salbutamol + Ipratropium combo | Combivent, Duolin | Nebulized q4-6h |
| Prednisolone | Prelone, Omnacortil | 40-60 mg PO OD x 5 days (COPD exacerbation) |
| Methylprednisolone | Medrol, Depo-Medrol | 40-125 mg IV if unable to take orally |
| Budesonide (nebulized) | Pulmicort | 1-2 mg nebulized q4-6h |
| Antibiotics (if bacterial exacerbation signs: increased sputum, change in color) | ||
| Amoxicillin-clavulanate | Augmentin | 875/125 mg PO BD for 5-7 days |
| Azithromycin | Zithromax | 500 mg OD for 5 days |
| Doxycycline | Vibramycin | 100 mg BD for 7-10 days |
| Levofloxacin | Levaquin | 750 mg OD for 5 days |
D. Influenza
| Drug | Brand Name | Dose | Duration |
|---|---|---|---|
| Oseltamivir | Tamiflu | 75 mg PO q12h | 5 days |
| Zanamivir (inhaled) | Relenza | 2 inhalations (10 mg) q12h | 5 days |
| Baloxavir | Xofluza | 40-80 mg PO single dose | Single dose |
Start within 48 hours of symptom onset for maximum benefit. High-risk patients (age >65, immunocompromised, pregnant) should be treated regardless of duration.
E. Supportive Measures for All Patients
| Measure | Detail |
|---|---|
| Oxygen therapy | Target SpO2 94-98% (88-92% in COPD); use nasal cannula, Venturi mask, or non-rebreather mask as needed |
| IV fluids | If unable to maintain oral intake; correct dehydration |
| Bronchodilators | Only if wheeze/obstruction present |
| DVT prophylaxis | Enoxaparin (Clexane) 40 mg SC OD for hospitalized patients |
| Patient education | Hydration, rest, return precautions, smoking cessation |
| Follow-up CXR | In 4-8 weeks for patients over 50 to confirm resolution and exclude underlying malignancy |
STEP 8 - Treatment Response and Review
| Timeframe | Expected Response |
|---|---|
| 24-48 hours | Fever should start to resolve; dyspnea improving |
| 3-5 days | Temperature normalization, reduced purulent sputum |
| 5-7 days | Consider step-down from IV to oral antibiotics |
| 2-4 weeks | Cough should resolve in bronchitis; CXR clears in CAP |
When to escalate:
- Persistent or worsening fever at 48-72 hours despite appropriate antibiotics - consider resistant organism, unusual pathogen (Legionella, TB, fungus), empyema, or non-infectious diagnosis
- Worsening SpO2 or respiratory distress - escalate to ICU, consider non-invasive ventilation (BiPAP) or intubation
Summary Algorithm
Cough + Sputum + Chest Tightness + Mild Fever
|
↓
STEP 1: History → Duration? Severity? Red flags? Risk factors?
|
↓
STEP 2: Exam → Vital signs + Auscultation
|
↓
STEP 3: SpO2, COVID/flu rapid test
|
↓
STEP 4: Differential → Bronchitis? Pneumonia? COPD? Asthma? PE? TB?
|
↓
STEP 5: CXR + CBC + CRP + Procalcitonin ± Blood cultures ± Sputum culture
|
↓
STEP 6: CURB-65 Score (for CAP)
0-1 → Outpatient | 2-3 → Admit | ≥3 + organ dysfunction → ICU
|
↓
STEP 7: Targeted Treatment
- Normal CXR + normal vitals → Supportive (Bronchitis)
- CXR infiltrate → Antibiotics based on CURB-65 + comorbidities
- Wheeze + reversible obstruction → Bronchodilators ± steroids
- Influenza positive → Oseltamivir (Tamiflu)
|
↓
STEP 8: Review at 48-72h → Escalate or de-escalate
Sources: Fishman's Pulmonary Diseases and Disorders (2-Vol Set) | Harrison's Principles of Internal Medicine 22E | Goldman-Cecil Medicine (Int'l Ed.) | Textbook of Family Medicine 9e | Washington Manual of Medical Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.