A child, 10 years old, complaints of headache, an increase in body temperature 10 36.8 "C. hemorrhagic rashes on the shins, thighs, buttocks, swelling of the knee and ankle joints. soreness when moving. It is known from the history of the disease that 3 weeks ago he was ill with ARVI, his mother gave paracetamol to reduce the temperature. Against the background of taking medications, a fine-spotted rash appeared on the skin of the shins, swelling of the knee joints, soreness in them when moving. A pediatrician called from the polyclinic regarded the symptoms as an allergic reaction to drug therapy. The patient was advised to stop taking anti-inflammatory drugs. Antihistamines are prescribed. After 2-3 days, the rashes and swelling of the joints disappeared, arthralgia stopped. In dynamics, the condition worsened again: hemorrhagic rashes appeared on the lower extremities, thighs, buttocks, swelling and soreness in the knee and ankle joints when moving. headache and weakness increased. Objectively: the patient's condition is moderate, the body temperature is 36,8 °C. The skin is pale, dry. On the skin of the extensor surfaces of the feet, shins, thighs, hemorrhagic rashes, sometimes having a drain character. The knee and ankle joints are enlarged in volume, movements in them are painful. Acute cramping pain in the abdomen every 5-7 minutes, during which the patient rushes and moans. In the lungs, respiration is vesicular, BH-20 per minute. The boundaries of the heart are within the normal range, the tones are muted, tachycardia is 100 per minute, the rhythm is correct, blood pressure is 100/60 mm Hg. Data from laboratory research methods. Clinical blood test: Hb-90 g/l, leukocytes-12.6 x109/1, rod-shaped 12%, 3.23. ESR-34 mm/h, platelets-180x109/1. Clinical analysis of urine: relative density-1015, protein-0.33 mg/l, red blood cells-0-1 in the field of vision.
Henoch-Schonlein purpura children treatment
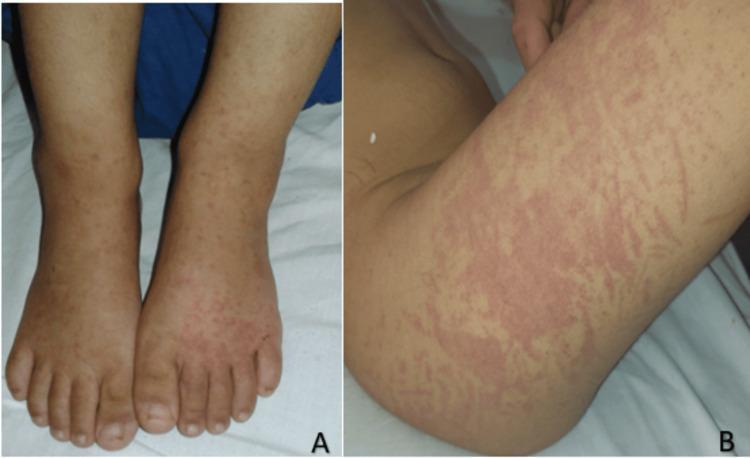
Henoch-Schonlein purpura rash legs child
Clinical Analysis: IgA Vasculitis (Henoch-Schönlein Purpura)
Diagnosis
- Acute cramping abdominal pain
- Acute arthralgia/arthritis (knees and ankles)
- Proteinuria + microscopic hematuria (renal involvement)
Pathophysiology
Clinical Features — Correlation with This Case
| Feature | This Patient | Typical IgAV |
|---|---|---|
| Age | 10 years | Peak 2–8 yrs; 75% in children |
| Triggering event | ARVI 3 weeks ago | Viral/streptococcal infection |
| Hemorrhagic purpura on shins, thighs, buttocks | ✓ | Present in >95% |
| Joint swelling (knee + ankle) | ✓ | 63–85% of patients |
| Cramping abdominal pain (q 5–7 min) | ✓ | ~65% |
| Low-grade fever, headache | ✓ | Common prodrome |
| Relapsing course | ✓ | ~30% have recurrent disease |
Laboratory Interpretation
| Test | Result | Interpretation |
|---|---|---|
| Hb 90 g/L | Low | Mild anemia — likely from GI blood loss and/or inflammation |
| Leukocytes 12.6 × 10⁹/L, rods 12% | Elevated with left shift | Active inflammatory response |
| ESR 34 mm/h | Elevated | Ongoing systemic inflammation |
| Platelets 180 × 10⁹/L | Normal | Key finding: rules out ITP and TTP/HUS |
| Urine protein 0.33 mg/L | Mild proteinuria | Early renal involvement |
| Urine RBC 0–1/hpf | Near normal | Microscopic hematuria |
Critical point: Normal platelet count distinguishes IgAV from immune thrombocytopenic purpura (ITP), thrombotic thrombocytopenic purpura (TTP), and hemolytic-uremic syndrome (HUS) — all of which cause thrombocytopenia with purpura.
Typical Rash

Differential Diagnosis to Exclude
| Condition | Reason to Exclude |
|---|---|
| ITP | Platelet count normal (180 × 10⁹/L) |
| Septic arthritis | Bilateral joint involvement, no extreme fever |
| Meningococcemia | No septic shock, non-blanching pattern on dependent areas |
| Drug reaction (initial misdiagnosis) | Relapsing course, classic tetrad present |
| HUS | No thrombocytopenia, no microangiopathic hemolytic anemia |
Management
- Severe cramping abdominal pain (risk of intussusception, GI bleeding)
- Moderate condition with tachycardia and anemia
- Renal involvement (proteinuria)
- An H2 blocker (ranitidine/famotidine) may be co-administered for GI symptoms.
Prognosis
- Overall favorable; most children recover fully within 6–16 weeks
- Relapses occur in ~30% — this child is already on his second episode
- Long-term renal insufficiency develops in <8% of children
- Risk factors for worse renal outcome: persistent proteinuria >1 g/day, gross hematuria, hypertension
- Regular follow-up urinalysis essential for 6–12 months
Recent Evidence (PubMed, 2024–2025)
- A 2024 meta-analysis (PMID: 39058868) compared mycophenolate mofetil vs. cyclophosphamide in IgAV nephritis — both options for steroid-refractory nephritis
- A 2024 systematic review (PMID: 39249581) examined rituximab for IgAV nephritis in refractory disease