ansa cervicalis
Reading File
Finding Sources
Searching Images
ansa cervicalis anatomy nerve loop
Reading File
Reading File
Loading Image
Loading Image
Ansa Cervicalis
The ansa cervicalis is a nerve loop derived from the cervical plexus (C1–C3) that provides motor innervation to three of the four infrahyoid (strap) muscles of the neck.
Formation
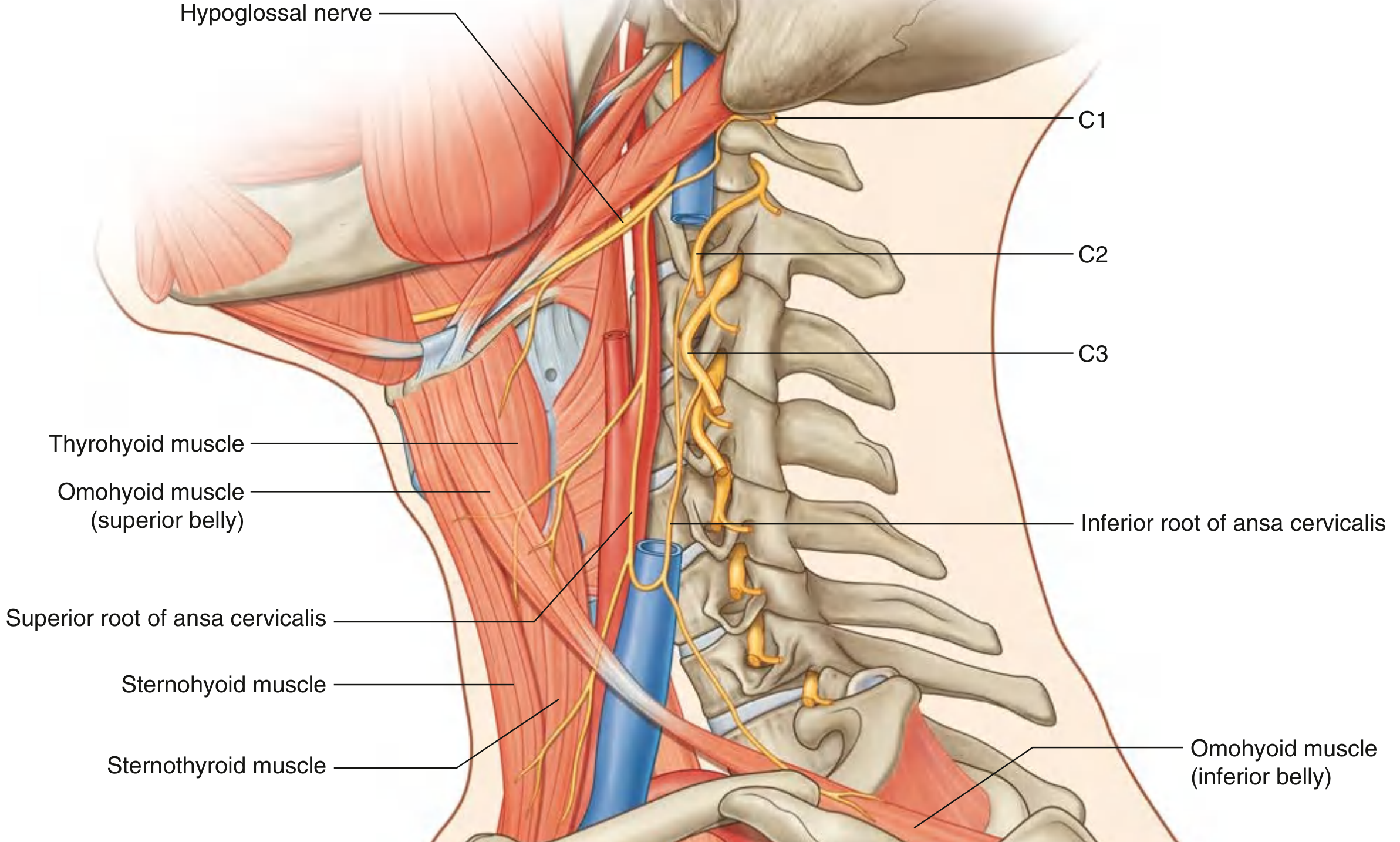
The loop is formed by two roots:
Superior Root (descendens hypoglossi)
- Originates from C1 fibers that hitch a ride with the hypoglossal nerve [XII] after it exits the skull
- As CN XII curves forward across the internal/external carotid arteries, the C1 fibers peel off and descend between the internal jugular vein and the carotid arteries
- Innervates:
- Superior belly of omohyoid
- Upper parts of sternohyoid and sternothyroid
Inferior Root (descendens cervicalis)
- Direct branch from the cervical plexus carrying fibers from C2 and C3
- Descends medial or lateral to the internal jugular vein, then turns medially to join the superior root, completing the loop
- Innervates:
- Inferior belly of omohyoid
- Lower parts of sternohyoid and sternothyroid
Note: The thyrohyoid muscle is the one strap muscle not innervated by the ansa cervicalis — it is innervated directly by C1 fibers traveling with the hypoglossal nerve.
Muscles Innervated (Summary)
| Muscle | Root |
|---|---|
| Sternohyoid (upper) | Superior root |
| Sternothyroid (upper) | Superior root |
| Omohyoid – superior belly | Superior root |
| Sternohyoid (lower) | Inferior root |
| Sternothyroid (lower) | Inferior root |
| Omohyoid – inferior belly | Inferior root |
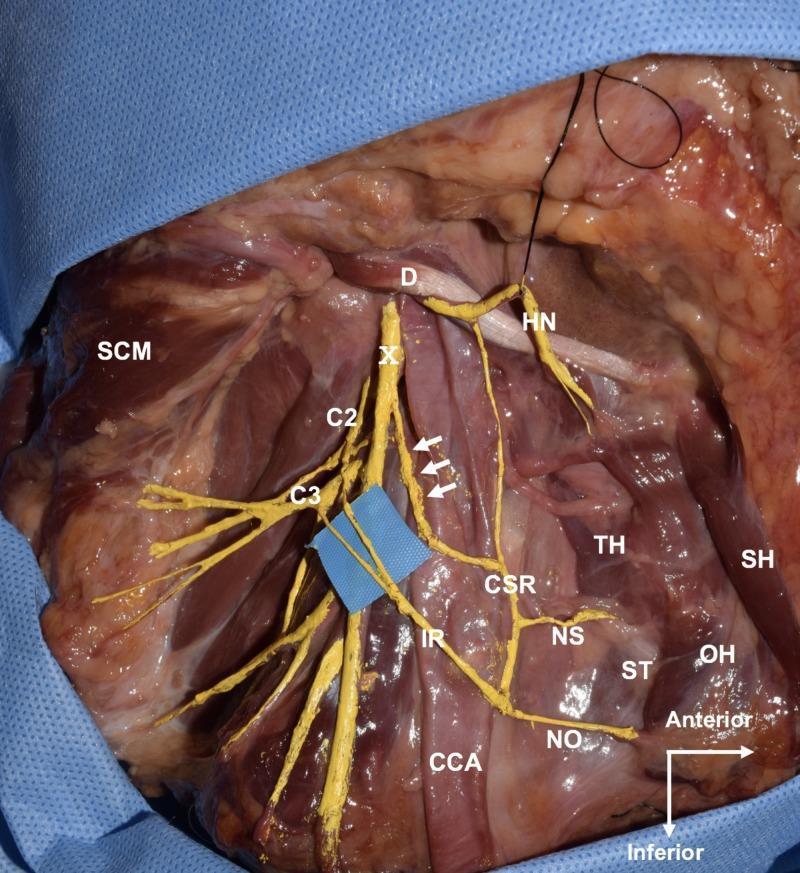
Relations
The ansa loop lies on (or within) the carotid sheath, overlying the common carotid artery — a key landmark during neck surgery.
Clinical Significance
1. Surgical injury
The ansa cervicalis lies close to the internal jugular vein and carotid artery. It can be inadvertently cut during carotid endarterectomy, neck dissection, or thyroidectomy, resulting in weakness of the strap muscles (usually clinically silent since these muscles are small).
2. Ansa cervicalis–Recurrent Laryngeal Nerve (RLN) transfer
A well-established reinnervation procedure for unilateral vocal fold paralysis:
- End-to-end anastomosis of the proximal ansa cervicalis to the distal stump of the RLN
- Restores muscle tone, bulk, and position to the paralyzed hemilarynx
- No return of active vocal fold motion is expected, but voice quality improves significantly
- First reported by Frazier et al. (1924); current use popularized since 1986
- Preferred over hypoglossal–RLN transfer due to lower morbidity from sacrificing this nerve
- — Cummings Otolaryngology, p. 1177
3. Anatomical variations
The superior root may receive contributions from both the hypoglossal nerve and the vagus nerve (a variation documented in cadaveric studies). The loop position can also vary (e.g., "short ansa" variant), which is surgically relevant for facial nerve reconstruction procedures.
Sources: Gray's Anatomy for Students, p. 1156; Cummings Otolaryngology Head and Neck Surgery, p. 1177
This is a shared conversation. Sign in to Orris to start your own chat.