Prostate gland d
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive, authoritative content from 4 textbooks plus 3 images. Let me compile the full answer.
The Prostate Gland
Overview
The prostate gland is the largest accessory sex gland of the male reproductive system. It is a fibromuscular and glandular organ commonly compared in size and shape to a walnut, weighing approximately 20 g in an adult. It lies just inferior to the bladder and surrounds the prostatic urethra (about 2.5 cm of it). - Smith and Tanagho's General Urology, 19th Ed.
Gross Anatomy
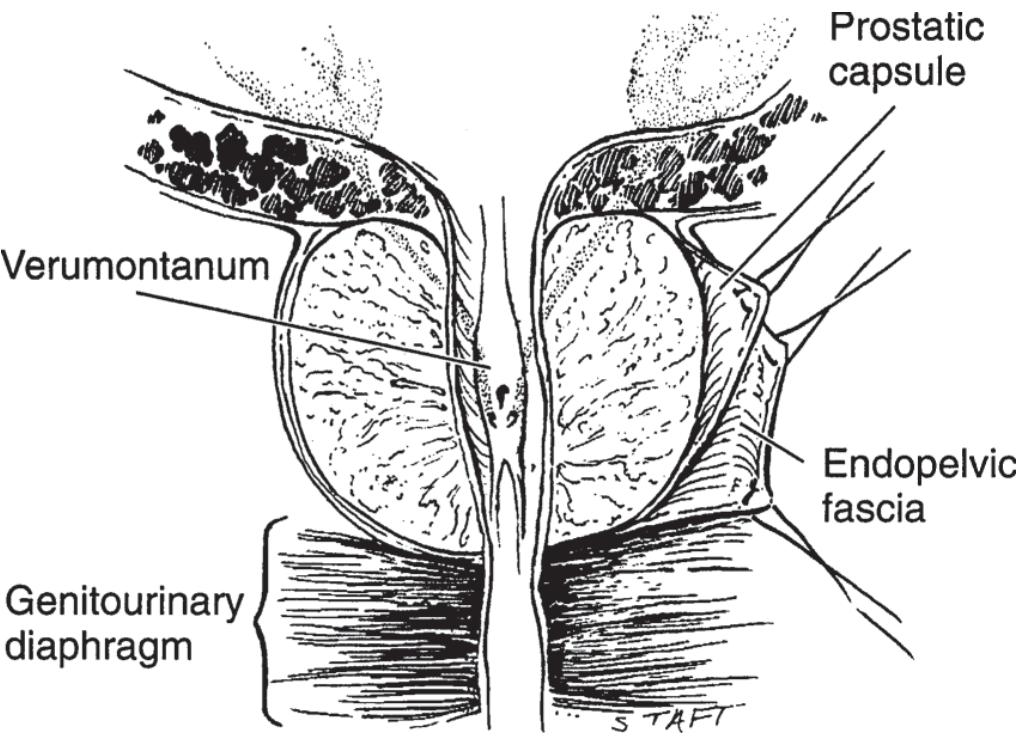
Position and supports:
- Lies behind the pubic symphysis
- Supported anteriorly by the puboprostatic ligaments
- Supported inferiorly by the urogenital diaphragm
- Posteriorly separated from the rectum by the two layers of Denonvilliers' fascia
- The posterosuperior surface is closely related to the vasa deferentia and seminal vesicles
Key landmark: The prostate is perforated posteriorly by the ejaculatory ducts, which empty through the verumontanum on the floor of the prostatic urethra just proximal to the striated external urinary sphincter.
Zonal Anatomy (McNeal's Classification)
The most clinically important system divides the prostate into four zones:
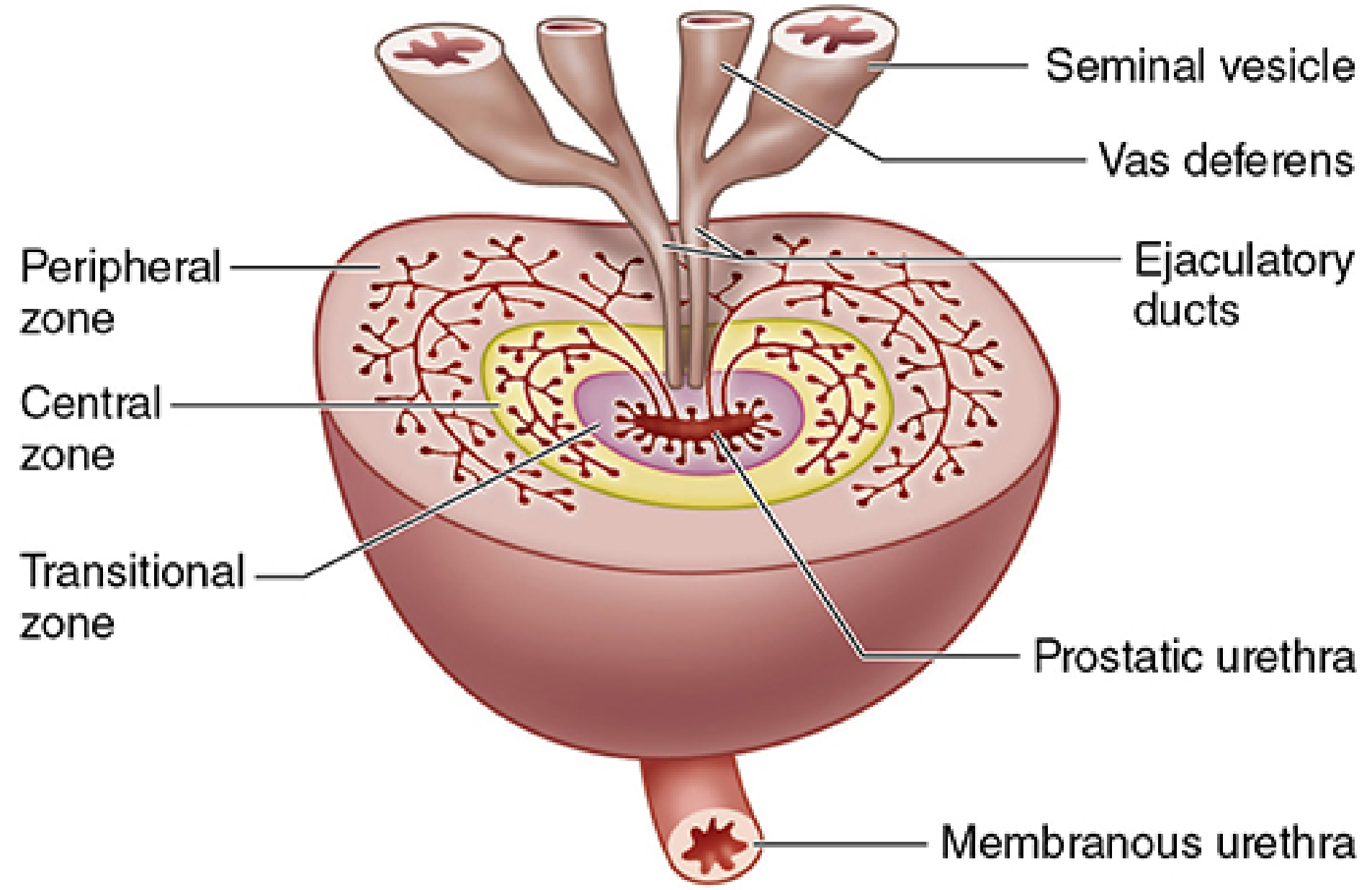
| Zone | % of gland | Contents | Clinical significance |
|---|---|---|---|
| Peripheral zone | ~70% | Main prostatic glands; longest ducts | Most prostatic carcinomas arise here; palpable on DRE; most susceptible to inflammation |
| Central zone | ~25% | Submucosal glands; surrounds ejaculatory ducts | Resistant to carcinoma and inflammation; possible mesonephric duct origin |
| Transitional zone | ~5% | Periurethral mucosal glands | Site of BPH - nodular hyperplasia compresses urethra |
| Anterior fibromuscular zone | - | Fibromuscular stroma | No glandular tissue |
- Smith and Tanagho's General Urology; Histology - A Text and Atlas, Wolters Kluwer
Histology
The prostate consists of 30-50 branched tubuloacinar (tubuloalveolar) glands embedded in a dense fibromuscular stroma. The smooth muscle in the stroma contracts at ejaculation.
- Glandular epithelium: simple or pseudostratified columnar epithelium
- Surrounded by a fibroelastic capsule with septa dividing the gland into indistinct lobes
- About 25 major excretory ducts open chiefly on the floor of the prostatic urethra between the verumontanum and the vesical neck
Corpora amylacea: Small spherical concretions (up to 2 mm), often partially calcified, normally present in gland lumina. They contain glycoproteins and keratan sulfate. They become more numerous with age but are clinically insignificant.
Below is the histological appearance of the prostate - epithelial glands embedded in connective/elastic tissue and smooth muscle:
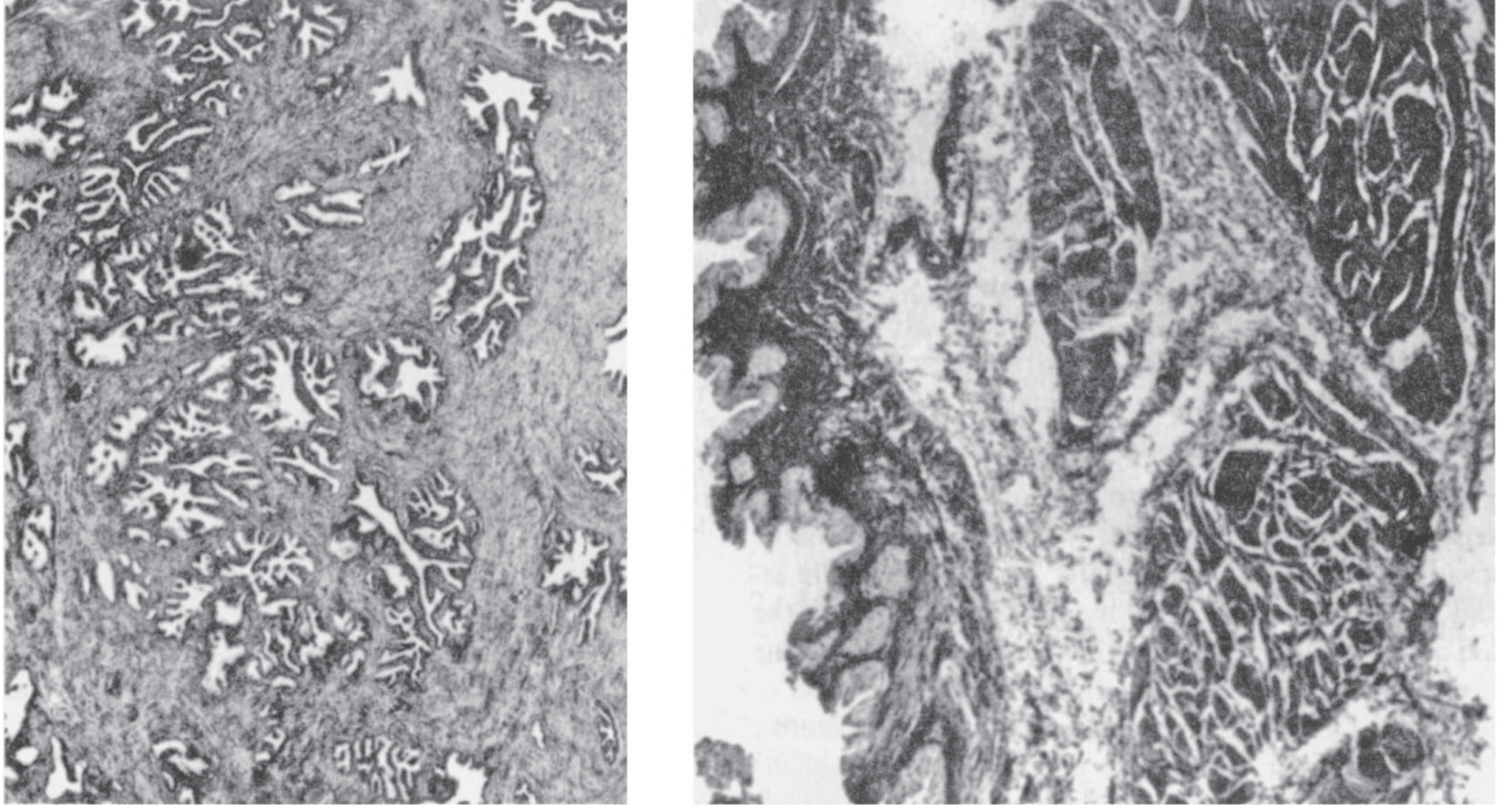
The prostate structure and function depend on testosterone levels. - Junqueira's Basic Histology, 17e
Prostatic Urethra and Sphincters
The segment of urethra traversing the prostate is lined by an inner longitudinal muscle layer (continuous with the vesical wall). The prostate contains an abundant smooth musculature derived from the external longitudinal bladder musculature - this forms the involuntary smooth muscle sphincter of the posterior urethra.
Blood Supply, Venous Drainage & Lymphatics
| Component | Details |
|---|---|
| Arterial supply | Inferior vesical artery, internal pudendal artery, middle rectal (hemorrhoidal) artery |
| Venous drainage | Periprostatic plexus → connects with deep dorsal vein of penis + internal iliac (hypogastric) veins |
| Lymphatics | Internal iliac (hypogastric), sacral, vesical, and external iliac lymph nodes |
| Nerve supply | Sympathetic + parasympathetic nerves from the inferior hypogastric plexus |
Smith and Tanagho's General Urology, 19th Ed.
Function
The prostate secretes a thin, milky, slightly alkaline fluid (~30% of total semen volume) containing:
- Calcium, citrate ion, phosphate ion
- A clotting enzyme (which causes fibrinogen from seminal vesicles to form a fibrin coagulum)
- Profibrinolysin (which dissolves the coagulum 15-30 min post-ejaculation, releasing sperm)
- PSA (Prostate-Specific Antigen) - a 34 kDa serine protease that liquefies coagulated semen
The slightly alkaline prostatic fluid neutralizes acidity of the vas deferens fluid and of vaginal secretions (pH 3.5-4.0), raising pH to ~6.0-6.5 to optimize sperm motility and fertility. - Guyton & Hall Textbook of Medical Physiology
Development and Hormonal Dependence
- Remains small throughout childhood
- Begins to grow at puberty under testosterone stimulation
- Reaches near-adult size by age 20
- Remains stable until ~age 50, then may involute as testosterone declines
- Structure and function depend on continuous testosterone stimulation
Clinical Diseases
1. Benign Prostatic Hyperplasia (BPH)
- Occurs almost exclusively in the transitional and periurethral zones
- Parenchymal cells undergo nodular hyperplasia, compressing the prostatic urethra
- Causes lower urinary tract symptoms (LUTS): hesitancy, weak stream, nocturia, incomplete emptying
- A benign prostatic fibroadenoma frequently develops in many older men
2. Prostate Cancer
- Arises most commonly from the peripheral zone (~70% of cases)
- Occurs in about 12% of men during their lifetime, usually after age 65
- Accounts for 2-3% of male deaths
- Testosterone stimulates cancer cell growth; estrogens/androgen deprivation inhibits it
- Serum PSA is the key biomarker - elevated PSA indicates abnormal glandular mucosa from carcinoma or inflammation
- Treatment: prostatectomy (localized disease), androgen deprivation therapy (advanced/metastatic disease)
3. Prostatitis
- The peripheral zone is the most susceptible to inflammation
Key Clinical-Anatomical Correlations
| Feature | Zone | Disease |
|---|---|---|
| BPH | Transitional zone | Urethral compression → LUTS |
| Cancer | Peripheral zone | Palpable on DRE, elevated PSA |
| Cancer spread | Via periprostatic/internal iliac nodes | Lymphatic metastasis |
| Cancer spread | Via Batson's plexus (periprostatic veins) | Bone metastasis (especially lumbar vertebrae) |
Sources: Smith and Tanagho's General Urology (19th Ed.) | Junqueira's Basic Histology (17th Ed.) | Histology: A Text and Atlas, Wolters Kluwer | Guyton & Hall Textbook of Medical Physiology
This is a shared conversation. Sign in to Orris to start your own chat.