35 yr old male came with hyperpigmentation at lateral canthal fold of right eye since 2 days . History of irritation and burning sensation present.Mild swelling of upper eyelid.No history of watering or Redness.Whats the management and diagnosis?
Reading File
Checking Date & Time
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Now I have all the information needed for a comprehensive clinical response.
Diagnosis: Herpes Zoster Ophthalmicus (HZO) — Prodromal/Early Stage
This presentation is classic for the prodromal phase of HZO — reactivation of Varicella-Zoster Virus (VZV) in the ophthalmic division (V1) of the trigeminal nerve.
Why this diagnosis fits
| Feature | Significance |
|---|---|
| Unilateral hyperpigmentation at lateral canthus | Early maculopapular/pigmented rash in V1 dermatome |
| Burning and irritation | Hallmark prodromal neuropathic symptom |
| Mild upper eyelid swelling | Boggy periorbital edema typical of early HZO |
| No watering, no redness | Suggests no conjunctival/corneal involvement yet |
| 2-day history | Consistent with prodrome before full vesiculation |
| 35-year-old male | Young adult — should prompt screening for immunodeficiency (HIV) |
"A prodromal phase precedes the appearance of the rash. It lasts 3–5 days and is characterized by tiredness, fever, malaise and headache. Symptoms involving the affected dermatome vary from a superficial itching, tingling or burning sensation to a severe boring or lancing pain." — Kanski's Clinical Ophthalmology, 10th ed.
"Painful erythematous areas with a maculopapular rash develop and may be confused with cellulitis or contact dermatitis. The rash respects the midline." — Kanski's Clinical Ophthalmology, 10th ed.
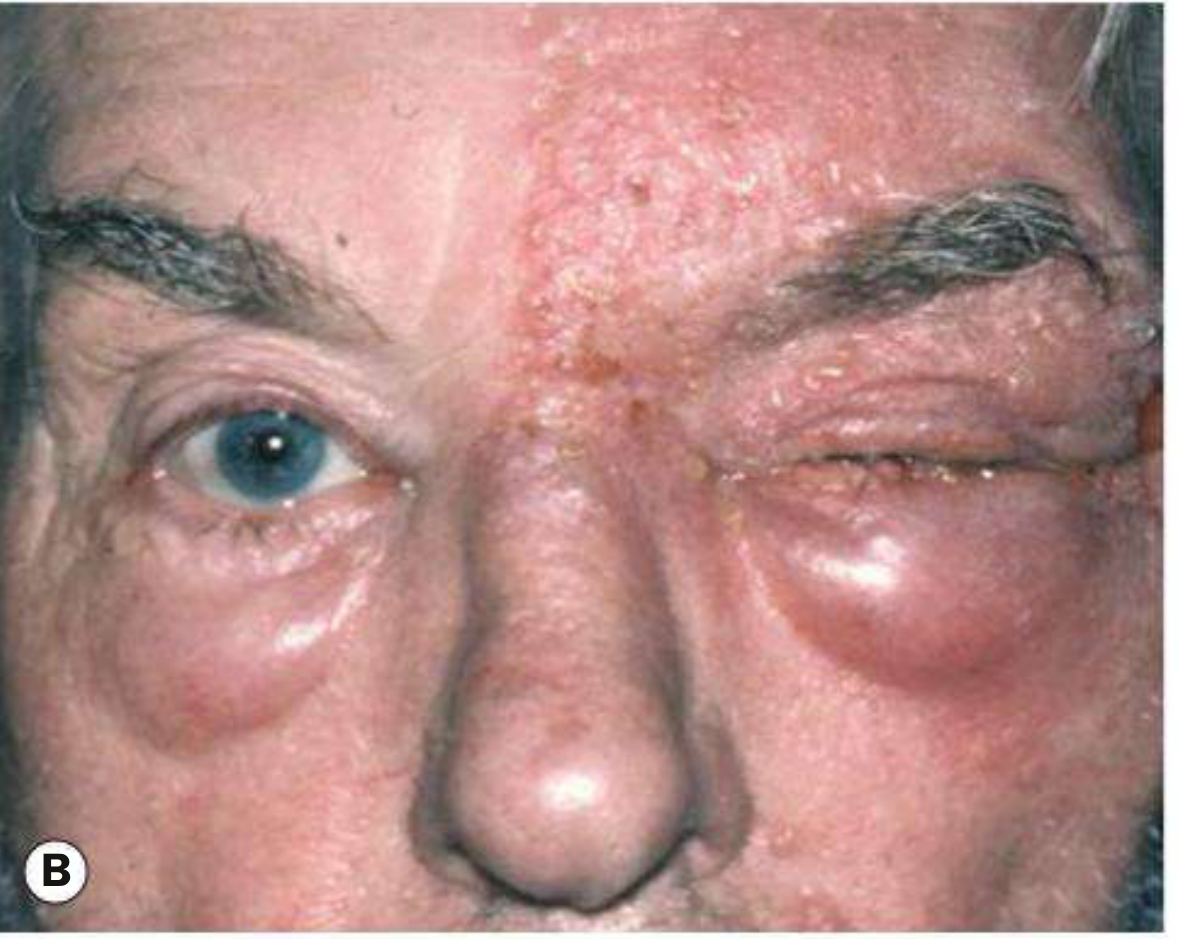
Clinical images of HZO — early skin lesions (A) and periorbital edema with skin involvement (B):

Important Red Flag in a 35-Year-Old
"The development of shingles in children or young adults has classically prompted a search for immunodeficiency or malignancy... A lower threshold for HIV testing should be adopted in populations at particular risk." — Kanski's Clinical Ophthalmology, 10th ed.
Screen for HIV / underlying immunosuppression in this patient.
Workup
- Full ocular examination — slit lamp with fluorescein staining, IOP, dilated fundus exam (rule out early keratitis, uveitis, acute retinal necrosis)
- Check for Hutchinson's sign — vesicles at the tip/side of nose indicating nasociliary branch involvement → high risk of corneal involvement
- HIV serology (given age <40)
- CBC, blood glucose — rule out diabetes/other immunocompromise
- If clinically uncertain: VZV PCR from skin lesion fluid or plasma
Management
1. Systemic Antivirals (start immediately — within 72 hours of rash onset for best effect)
| Drug | Dose | Duration |
|---|---|---|
| Valacyclovir (preferred) | 1 g orally three times daily | 7–10 days |
| Famciclovir | 500 mg orally three times daily | 7–10 days |
| Acyclovir | 800 mg orally five times daily | 7–10 days |
"Oral antiviral treatment, optimally given within 72 hours of rash onset, reduces the severity and duration of the acute episode and the risk of post-herpetic neuralgia. The incidence of late ophthalmic complications is also reduced by about 50%." — Kanski's Clinical Ophthalmology, 10th ed.
2. Local Skin Care
- Warm compresses to periocular skin three times daily
- Topical antibiotic ointment (bacitracin or erythromycin ophthalmic ointment) to skin lesions twice daily — to prevent secondary bacterial infection
3. Pain Management
- NSAIDs or paracetamol for mild pain
- Neuropathic agents (gabapentin, pregabalin) if pain is severe or PHN develops
4. Ophthalmology Referral
- Mandatory — even without current ocular signs, corneal and uveal involvement can follow skin rash by days to weeks
- Repeat slit lamp exam at follow-up
5. Systemic Steroids (conditional)
- Consider prednisolone (60 mg tapering over 12 days) for moderate-severe disease only in conjunction with antivirals and only if immunocompetent
- Avoid in immunocompromised patients
6. Hospitalization / IV Acyclovir
- Indicated if: orbital involvement, optic nerve/cranial nerve involvement, systemic illness, or immunocompromised state
- IV Acyclovir 5–10 mg/kg q8h
Differential Diagnoses to Exclude
| Condition | Distinguishing Feature |
|---|---|
| HSV periocular infection | Not dermatomal, less severe pain, younger onset |
| Preseptal cellulitis | Bilateral spread possible, fever, systemic signs |
| Contact dermatitis | Bilateral, itching > burning, no dermatomal pattern |
| Allergic reaction | History of exposure, bilateral, urticarial |
Summary: This is most likely early/prodromal HZO. Start oral antivirals immediately, refer to ophthalmology, screen for HIV given the patient's young age, and monitor closely for ocular complications (keratitis, uveitis) which may develop over the coming days even if currently absent.
Sources: Kanski's Clinical Ophthalmology 10th Ed.; The Wills Eye Manual; Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.