Top ten cardiology disease with ecg changes
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching Images
ECG changes myocardial infarction ST elevation Q wave
Searching Images
atrial fibrillation ECG irregularly irregular
Reading File
Searching Images
pericarditis saddle shaped ST elevation ECG
Searching Images
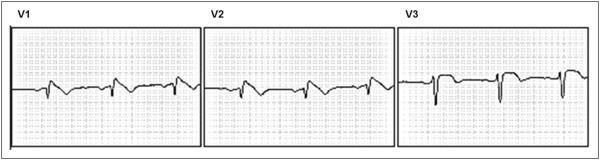
Brugada syndrome ECG pattern coved ST elevation V1 V2
Searching Images
pulmonary embolism ECG right heart strain S1Q3T3
Searching Images
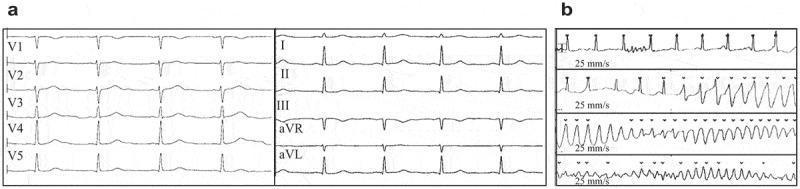
Wolff-Parkinson-White syndrome delta wave short PR interval ECG
Searching Images
hypertrophic cardiomyopathy ECG left ventricular hypertrophy deep Q waves
Searching Images
long QT syndrome torsades de pointes ECG QTc prolonged
Searching Images
complete heart block third degree AV block ECG P wave dissociation
I now have comprehensive material from multiple authoritative textbooks and high-quality ECG images. Let me compile the complete answer:
Top 10 Cardiology Diseases with ECG Changes
1. 🫀 Acute Myocardial Infarction (STEMI / NSTEMI)
The ECG is the cornerstone of AMI diagnosis. Three electrocardiographic phases characterize acute infarction:
| ECG Change | Timing | Leads |
|---|---|---|
| Hyperacute T waves (tall, peaked) | Minutes | Over infarct zone |
| ST elevation (convex/tombstone) | Minutes–hours | Over infarct zone |
| Reciprocal ST depression | Minutes–hours | Opposite leads |
| T-wave inversion | Hours–days | Evolving |
| Pathological Q waves (≥1 mm wide, ≥25% QRS height) | Hours–days | Necrosis zone |
Localization:
- Anterior (LAD): V1–V4, I, aVL
- Inferior (RCA): II, III, aVF
- Lateral (LCx): I, aVL, V5–V6
- Posterior (RCA/LCx): Reciprocal ST depression in V1–V3 (mirror image)
- Right ventricular (proximal RCA): ST elevation in V4R
Three major membrane abnormalities cause ECG changes in AMI: rapid repolarization, decreased resting membrane potential, and delayed depolarization — all producing ST elevation over the infarct. — Ganong's Review of Medical Physiology
NSTEMI: ST depression, T-wave inversions, or no ECG change — diagnosed by elevated biomarkers.
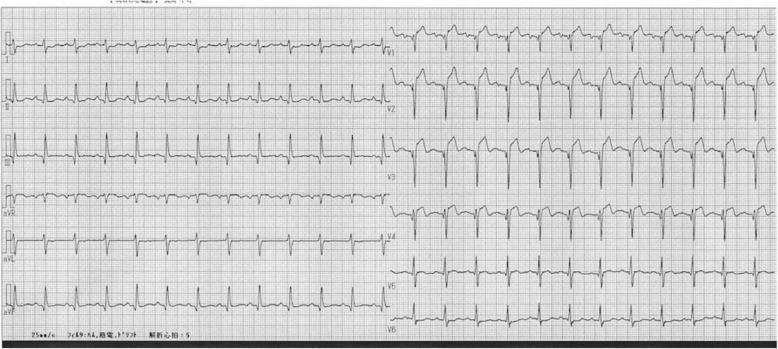
2. 🫀 Atrial Fibrillation (AF)
| ECG Feature | Description |
|---|---|
| No P waves | Replaced by chaotic fibrillatory (f) waves |
| Irregularly irregular ventricular rhythm | Variable R-R intervals |
| Narrow QRS (usually) | Unless aberrant conduction or pre-excitation |
| Fibrillatory baseline | Best seen in V1, II |
"The ECG hallmarks of atrial fibrillation include the absence of discernible P waves and an irregularly irregular ventricular rhythm." — Tintinalli's Emergency Medicine
With rapid ventricular response: rate >100 bpm. With slow ventricular response (e.g., AV nodal disease): rate <60 bpm.
3. 🫀 Acute Pericarditis
Distinctive 4-stage ECG evolution:
| Stage | ECG Finding |
|---|---|
| Stage 1 (days 1–2) | Diffuse concave ("saddle-shaped") ST elevation in nearly all leads + PR depression (especially II, V4–V6); aVR shows reciprocal ST depression + PR elevation |
| Stage 2 (days 3–7) | ST returns to baseline; PR remains depressed |
| Stage 3 (week 2) | T-wave inversions develop |
| Stage 4 (weeks–months) | ECG normalizes |
Key differentiator from STEMI: Diffuse distribution (not single coronary territory), saddle-shaped (concave) morphology, PR depression, no Q waves.
Spodick's sign: Downward sloping TP segment — highly specific for pericarditis.

4. 🫀 Complete (Third-Degree) AV Heart Block
| ECG Feature | Description |
|---|---|
| Complete AV dissociation | P waves and QRS complexes fire independently |
| Atrial rate > ventricular rate | Atria controlled by SA node; ventricles by escape pacemaker |
| Narrow escape QRS | Junctional escape (above His bifurcation) ~40–60 bpm |
| Wide escape QRS | Ventricular escape (infra-Hisian) ~20–40 bpm — more dangerous |
P waves "march through" QRS complexes with no fixed PR interval.

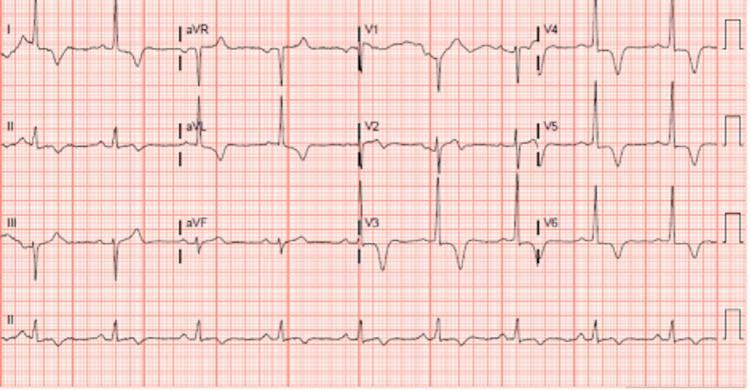
5. 🫀 Pulmonary Embolism (PE)
Most common ECG finding is sinus tachycardia. Classic but non-specific sign:
| ECG Feature | Description |
|---|---|
| S1Q3T3 | Deep S in lead I + Q wave in lead III + T-wave inversion in lead III (McGinn-White sign) |
| Sinus tachycardia | Most common finding |
| Right axis deviation | Due to acute RV strain |
| Incomplete/complete RBBB | Acute right heart pressure overload |
| T-wave inversions V1–V4 | Right ventricular strain pattern |
| P pulmonale | Tall peaked P waves in II (>2.5 mm) |
| Atrial fibrillation | Can occur with massive PE |
S1Q3T3 reflects the pathophysiological stress of the right ventricle against increased pulmonary vascular resistance. Only ~20% of PE patients show this pattern — its absence does not exclude PE.

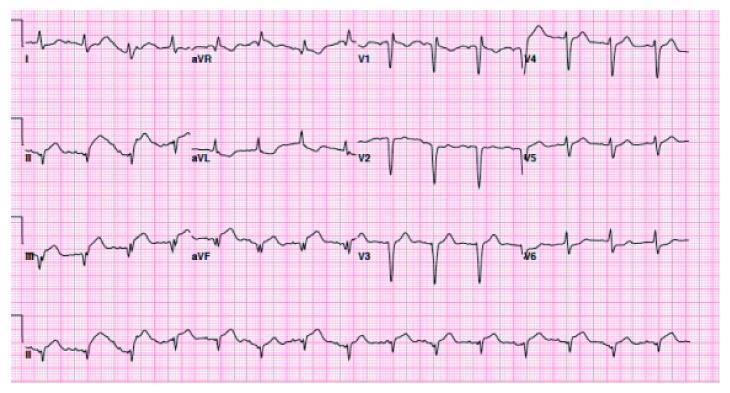
6. 🫀 Hypertrophic Cardiomyopathy (HCM)
| ECG Feature | Description |
|---|---|
| LVH voltage criteria | Sokolow-Lyon: S in V1 + R in V5/V6 ≥35 mm |
| Deep, narrow Q waves | In I, aVL, V5–V6 (septal hypertrophy) |
| Giant T-wave inversions (apical variant) | Leads V2–V6, >10 mm (Yamaguchi syndrome) |
| ST depression | Lateral leads — "strain pattern" |
| Atrial enlargement | Broad notched P waves |
| Left axis deviation | Common |
HCM is the most common cause of sudden cardiac death in young athletes. ECG screening identifies this condition.
7. 🫀 Wolff-Parkinson-White (WPW) Syndrome
The classic triad of pre-excitation:
| ECG Feature | Description |
|---|---|
| Short PR interval | <120 ms (bypass of AV node) |
| Delta wave | Slurred upstroke of QRS (slow initial depolarization via accessory pathway) |
| Wide QRS | Prolonged (≥120 ms) due to fusion of normal + accessory conduction |
| Secondary ST-T changes | Discordant to delta wave |
| Pseudo-infarction pattern | Negative delta waves can mimic Q waves |
Accessory pathway localization from delta wave polarity. Risk: if AF develops with rapid conduction down the accessory pathway → ventricular fibrillation.
"WPW is an ECG pattern characterized by a short PR interval followed by a delta wave and a prolonged QRS duration." — Pfenninger and Fowler's Procedures for Primary Care

8. 🫀 Long QT Syndrome (LQTS)
| ECG Feature | Description |
|---|---|
| Prolonged QTc | ≥440 ms (males), ≥460 ms (females) — calculated using Bazett's formula: QTc = QTm / √R-R |
| Broad/notched T waves | LQT1 pattern |
| Biphasic T waves | LQT2 pattern |
| Late-onset T wave after pause | LQT3 (SCN5A mutation) |
| T-wave alternans | Beat-to-beat amplitude/polarity variation — marker of high arrhythmic risk |
| Torsades de Pointes | Polymorphic VT with "twisting" QRS complexes around isoelectric line |
Congenital subtypes: Romano-Ward (autosomal dominant, no deafness) and Jervell-Lange-Nielsen (autosomal recessive, with sensorineural deafness).
"The long QT syndrome is characterized by prolongation of the corrected QT interval, syncope, and sudden death caused by torsades de pointes and ventricular fibrillation." — Tintinalli's Emergency Medicine
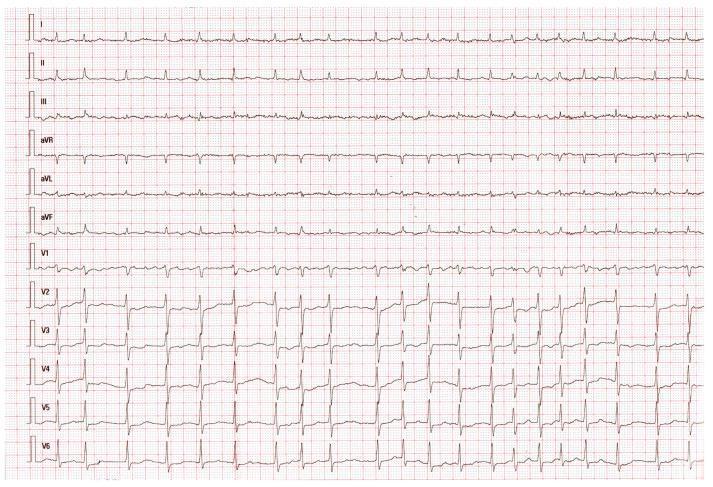
9. 🫀 Brugada Syndrome
A sodium channelopathy (SCN5A mutation) causing potentially fatal ventricular arrhythmias, predominantly in young men.
| Type | ECG Pattern (V1–V2) |
|---|---|
| Type 1 (Diagnostic) | Coved ST elevation ≥2 mm → descending to inverted T wave. Spontaneous or drug-induced. |
| Type 2 | Saddleback ST elevation ≥2 mm → upright or biphasic T wave |
| Type 3 | Saddleback or coved ST elevation <2 mm |
Only Type 1 is diagnostic. Type 2/3 can convert to Type 1 with sodium channel blocker challenge (ajmaline/flecainide).
"Type 1 Brugada pattern: characteristic coved ST-segment elevation in V1–V2, associated with polymorphic VT and sudden cardiac death." — Harrison's Principles of Internal Medicine 22E (2025)
10. 🫀 Left Bundle Branch Block (LBBB) / Ventricular Hypertrophy
Left Bundle Branch Block (LBBB)
| ECG Feature | Description |
|---|---|
| QRS ≥120 ms | Broad, notched ("M-shaped") in I, V5–V6 |
| No septal Q waves in I, V5–V6 | Loss of normal septal activation |
| RS or rS in V1 | Deep S wave |
| Discordant ST-T waves | Opposite direction to QRS deflection |
| New LBBB + ischemia | Equivalent to ST elevation — warrants acute reperfusion |
Left Ventricular Hypertrophy (LVH)
| Criteria | Values |
|---|---|
| Sokolow-Lyon | SV1 + RV5 or RV6 ≥35 mm |
| Cornell voltage | RaVL + SV3 >28 mm (men), >20 mm (women) |
| Strain pattern | ST depression + T-wave inversion in I, aVL, V5–V6 |
| Left axis deviation | QRS axis more negative than −30° |
"Left anterior fascicular block (QRS axis more negative than −45°) is probably the most common cause of marked left axis deviation in adults." — Harrison's Principles of Internal Medicine 22E
Summary Table
| # | Disease | Hallmark ECG Change |
|---|---|---|
| 1 | STEMI | ST elevation (convex) → Q waves; territory-specific |
| 2 | Atrial Fibrillation | No P waves + irregularly irregular rhythm |
| 3 | Acute Pericarditis | Diffuse saddle-shaped ST elevation + PR depression |
| 4 | Complete AV Block | P-QRS dissociation + ventricular escape rhythm |
| 5 | Pulmonary Embolism | S1Q3T3 + sinus tachycardia + RV strain |
| 6 | Hypertrophic Cardiomyopathy | LVH + deep Q waves (septal) / giant T inversions (apical) |
| 7 | WPW Syndrome | Short PR + delta wave + wide QRS |
| 8 | Long QT Syndrome | QTc ≥440–460 ms → Torsades de Pointes |
| 9 | Brugada Syndrome | Type 1 coved ST elevation in V1–V2 |
| 10 | LBBB / LVH | QRS ≥120 ms, notched R in I/V6; or high voltage + strain |
Sources: Harrison's Principles of Internal Medicine 22E (2025), Ganong's Review of Medical Physiology, Tintinalli's Emergency Medicine, Braunwald's Heart Disease, Fuster and Hurst's The Heart 15E, Pfenninger and Fowler's Procedures for Primary Care
This is a shared conversation. Sign in to Orris to start your own chat.