Nitric oxide in pulmonary diseases for md exams 10 marks answer
Reading File
Finding Sources
Finding Sources
Searching PubMed
"nitric oxide" AND "pulmonary hypertension"
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have all the material needed for a comprehensive 10-mark MD exam answer. Here it is:
Nitric Oxide in Pulmonary Diseases
1. Introduction
Nitric oxide (NO) is a gaseous free radical originally identified as endothelium-derived relaxing factor (EDRF). In the pulmonary circulation, it plays a central role in maintaining vascular homeostasis, regulating ventilation-perfusion matching, and acting as a therapeutic agent in several pulmonary disorders. Its short half-life, unique selectivity for the pulmonary vasculature when inhaled, and powerful vasodilatory mechanism make it clinically relevant across a range of pulmonary diseases.
2. Synthesis and Mechanism of Action
Synthesis
NO is synthesized from L-arginine by the enzyme nitric oxide synthase (NOS) in an O2- and NADPH-dependent reaction, producing NO and L-citrulline. Cofactors include heme, tetrahydrobiopterin (BH4), and flavin adenine dinucleotide (FAD).
There are three NOS isoforms:
| Isoform | Other Name | Location | Regulation |
|---|---|---|---|
| NOS-1 | nNOS (neuronal) | Neurons, skeletal muscle | Constitutive, Ca²+-dependent |
| NOS-2 | iNOS (inducible) | Macrophages, smooth muscle | Induced by inflammatory mediators |
| NOS-3 | eNOS (endothelial) | Vascular endothelium, platelets | Constitutive; activated by shear stress via PIEZO1 mechanosensitive channel |
The eNOS isoform is the predominant source of physiological pulmonary NO. Shear forces from blood flow activate PIEZO1, phosphorylating and activating eNOS. The iNOS isoform, induced by inflammatory cytokines, generates large quantities of NO and is relevant in sepsis and ARDS.
Mechanism of Action
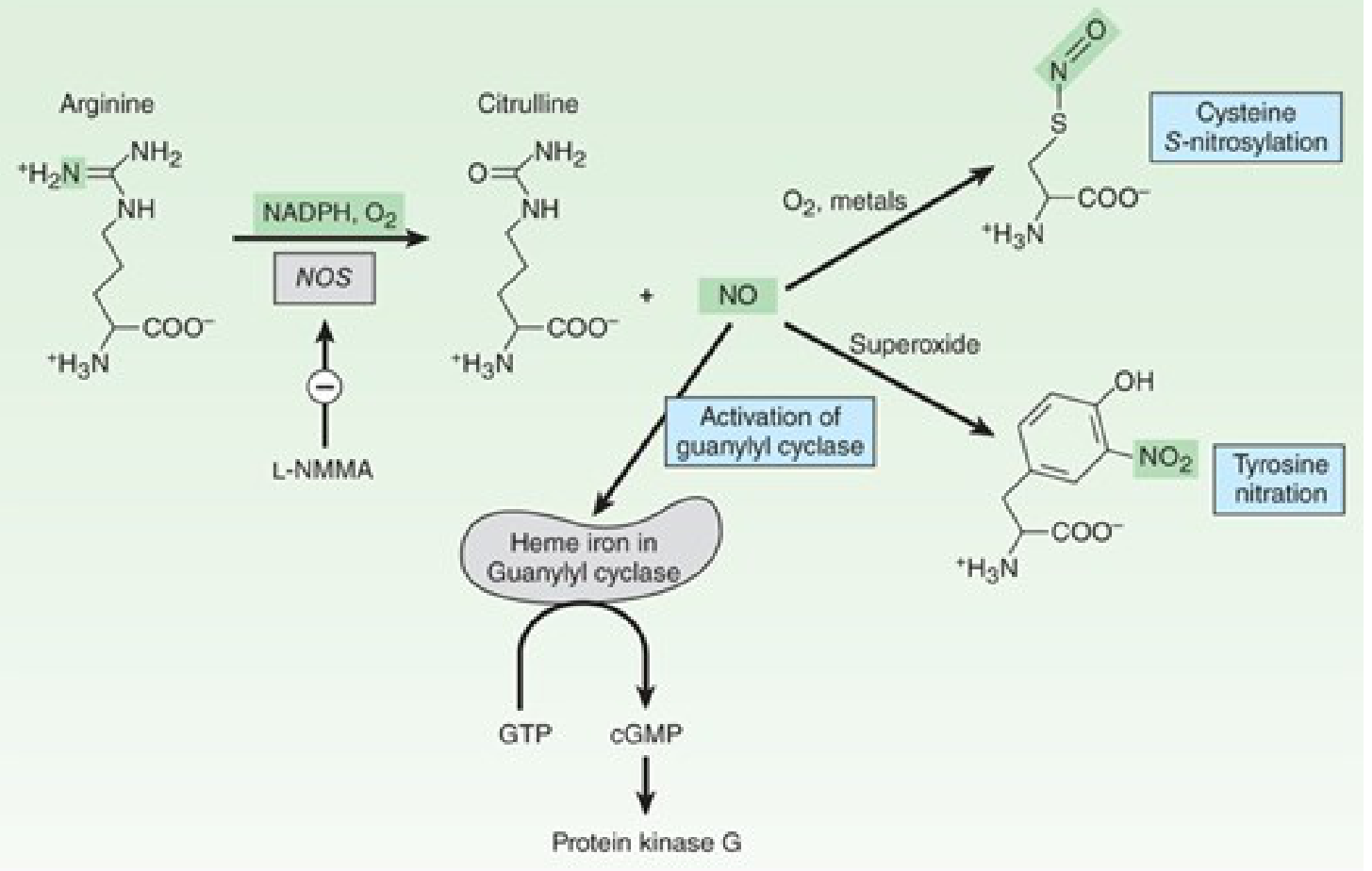
Fig: Synthesis and reactions of NO (Katzung's Basic and Clinical Pharmacology, 16e)
- NO diffuses from endothelial cells into vascular smooth muscle cells
- It binds to the heme iron of soluble guanylyl cyclase (sGC)
- This activates sGC, converting GTP to cyclic GMP (cGMP)
- cGMP activates Protein Kinase G (PKG), reducing intracellular Ca²+ and causing smooth muscle relaxation and vasodilation
- Under oxidative stress, NO reacts with superoxide to form peroxynitrite, leading to tyrosine nitration and cellular damage
Key feature: When inhaled, NO is rapidly inactivated by hemoglobin, preventing systemic vasodilation. This makes it a selective pulmonary vasodilator.
3. Physiological Role in the Pulmonary Circulation
- The pulmonary vascular endothelium produces NO, prostacyclin, and endothelin to control vasomotor tone
- NO and prostacyclin act as vasodilators and antiproliferative agents; endothelin acts as a vasoconstrictor
- In healthy lungs, NO maintains low pulmonary vascular resistance (PVR) and prevents smooth muscle cell proliferation and platelet aggregation
- NO also plays a role in hypoxic pulmonary vasoconstriction (HPV): inhibition of NOS enhances HPV, and inhaled NO reduces or offsets hypoxic vasoconstriction, redirecting blood flow toward ventilated lung segments - Costanzo Physiology, 7e
4. Nitric Oxide in Specific Pulmonary Diseases
A. Pulmonary Arterial Hypertension (PAH)
In PAH, there is:
- Reduced NO and prostacyclin production (potent vasodilators)
- Increased endothelin production (a vasoconstrictor and promoter of vascular remodeling)
- This imbalance leads to pulmonary vasculopathy, increased PVR, and right ventricular failure
The NO-cGMP pathway is a therapeutic target:
- Sildenafil (PDE-5 inhibitor): Inhibits phosphodiesterase-5, which breaks down cGMP in pulmonary vessels, thereby amplifying NO's vasodilatory effect. Approved for PAH; improves 6-minute walk distance, NYHA functional class, pulmonary artery pressure, and cardiac index
- Dipyridamole: Also has PDE-5 activity; used in combination with inhaled NO in a 2-year trial that showed improvements in exercise capacity and hemodynamics
- Inhaled NO (iNO): Used as vasodilator testing at cardiac catheterization; selected patients with reactive PAH respond and may benefit from calcium channel blockers
B. Persistent Pulmonary Hypertension of the Newborn (PPHN)
- At birth, the first breath raises alveolar PO2, which suppresses HPV, reduces PVR, and opens the pulmonary vasculature
- In PPHN, this transition fails; pulmonary vasculature remains constricted
- Inhaled NO is the treatment of choice for PPHN; it selectively dilates pulmonary vessels, improving V/Q matching and oxygenation
- It improves survival in neonates with reactive pulmonary hypertension and reduces the need for extracorporeal membrane oxygenation (ECMO) - Miller's Anesthesia, 10e
C. Acute Respiratory Distress Syndrome (ARDS)
- In ARDS, iNOS is upregulated; large quantities of NO contribute to endothelial injury, capillary leakage, and microvascular dysfunction
- An imbalance between vasodilation by NO and vasoconstriction leads to impaired gas exchange
- Inhaled NO as salvage therapy: Selectively vasodilates pulmonary vessels in well-ventilated alveoli (since it only reaches ventilated areas), improving V/Q matching and short-term oxygenation
- However, clinical trials have consistently shown no reduction in mortality or duration of mechanical ventilation with iNO in ARDS
- The 2025 Harrison's recommendations list NO as part of salvage strategies (along with prone positioning and ECMO) for refractory hypoxemia - Harrison's Principles of Internal Medicine, 22e
- A 2025 systematic review (PMID: 40031892) specifically examined iNO for bronchopulmonary dysplasia-associated pulmonary hypertension in neonates
D. Pulmonary Embolism (PE)
- Acute massive PE causes acute pulmonary hypertension; inhaled NO and epoprostenol decrease pulmonary vascular resistance and pulmonary arterial pressure
- Evidence is limited to case series; a clinical trial failed to show benefit of iNO in hemodynamically stable patients with PE and RV dysfunction - ROSEN's Emergency Medicine
- Not a standard treatment in PE; used as a bridge in refractory cases
E. COPD-Associated Pulmonary Hypertension and Cor Pulmonale
- In COPD, intimal thickening and vascular remodeling are associated with reduced NO and prostacyclin production
- This endothelial dysfunction promotes pulmonary vasculopathy and contributes to the development of pulmonary hypertension and cor pulmonale
- Pulmonary endothelial dysfunction is observed even in mild-to-moderate COPD - Fuster and Hurst's The Heart, 15e
F. High-Altitude Pulmonary Edema (HAPE)
- HAPE-prone individuals have reduced levels of exhaled NO
- This impairs the ability to offset hypoxic pulmonary vasoconstriction at altitude
- Phosphodiesterase-5 inhibitors (which augment the NO-cGMP pathway) alleviate altitude-induced pulmonary hypertension and hypoxemia - Harrison's Principles of Internal Medicine, 22e
5. Clinical Use of Inhaled Nitric Oxide (iNO)
| Parameter | Details |
|---|---|
| Dose | 5-80 ppm; clinical use typically 5-20 ppm |
| Route | Delivered via inhalation through ventilator circuit |
| Selectivity | Rapidly inactivated by hemoglobin; no systemic vasodilation at standard doses |
| Monitoring | Methemoglobin levels (rare but clinically significant at higher doses) |
| Weaning | Must be weaned gradually; abrupt discontinuation causes rebound pulmonary hypertension |
Indications:
- PPHN (most established - reduces ECMO need)
- Post-operative pulmonary hypertensive crises (cardiac surgery, congenital heart disease repair)
- Refractory hypoxemia in ARDS (salvage)
- Vasodilator testing in PAH workup
Limitations:
- Expensive
- Requires specialized delivery systems
- Does not improve mortality in ARDS
- Rebound pulmonary hypertension on discontinuation
6. Endothelial Dysfunction and NO Deficiency
Reduced NO production in the pulmonary endothelium is a common pathway in multiple pulmonary vascular diseases:
- eNOS expression is notably reduced in inflammatory disease and diabetes, leading to reduced NO and increased vascular tone
- This creates a prothrombotic, vasoconstrictive, and profibrotic milieu
- Therapeutic strategies targeting the NO pathway (PDE-5 inhibitors, soluble guanylate cyclase stimulators like riociguat) are central to PAH management
7. Summary Table
| Disease | NO Status | Role of iNO Therapy | Evidence |
|---|---|---|---|
| PPHN | Deficient | Treatment of choice | Strong (Class I) |
| PAH | Deficient (eNOS↓) | Vasodilator testing; PDE-5 inhibitors preferred | Strong |
| ARDS | Excess (iNOS↑) + dysfunction | Salvage for oxygenation only | Improves O2; no mortality benefit |
| COPD-PH/Cor pulmonale | Deficient | Not established | Pathophysiological only |
| HAPE | Deficient | PDE-5 inhibitors benefit | Moderate |
| Acute PE | - | Reduces PVR in case series; no RCT benefit | Limited |
Sources: Katzung's Basic and Clinical Pharmacology 16e | Miller's Anesthesia 10e | Costanzo Physiology 7e | Fuster and Hurst's The Heart 15e | Harrison's Principles of Internal Medicine 22e | ROSEN's Emergency Medicine | Current Surgical Therapy 14e | Textbook of Family Medicine 9e
This is a shared conversation. Sign in to Orris to start your own chat.