Hernia
Reading File
Asking for Preferences
Finding Sources
Searching the Web
hernia types overview classification 2024
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have all the content needed for a comprehensive overview. Here is the full answer:
Hernia - Overview & Types
Definition
A hernia is the protrusion of any viscus (organ or tissue) from its normal cavity through an abnormal opening. In the abdomen - the most common site - intraabdominal contents (usually bowel or omentum) protrude through a defect or weakness in the abdominal wall musculature.
- Hernias develop either along a congenital tract that fails to close (e.g., indirect inguinal, umbilical) or along an acquired area of weakness (e.g., direct inguinal, incisional)
- Estimated to affect 5% of men and 2% of women
- About 75% occur in the groin
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
Classification by Reducibility (Clinical Priority)
The first priority in assessing any hernia is to classify it by reducibility:
| Type | Description | Clinical Implication |
|---|---|---|
| Reducible | Contents return through the defect without surgery | Can be managed electively |
| Incarcerated | Contents are NOT reducible without surgery; often with swelling of sac contents | Not necessarily an emergency unless obstruction is present |
| Strangulated | Incarcerated + blood supply to herniated content is compromised | Surgical emergency - tissue ischemia and necrosis will result |
Hernias with a small neck are most prone to incarceration and strangulation.
Major Types by Location
1. Ventral Hernias (Abdominal Wall)
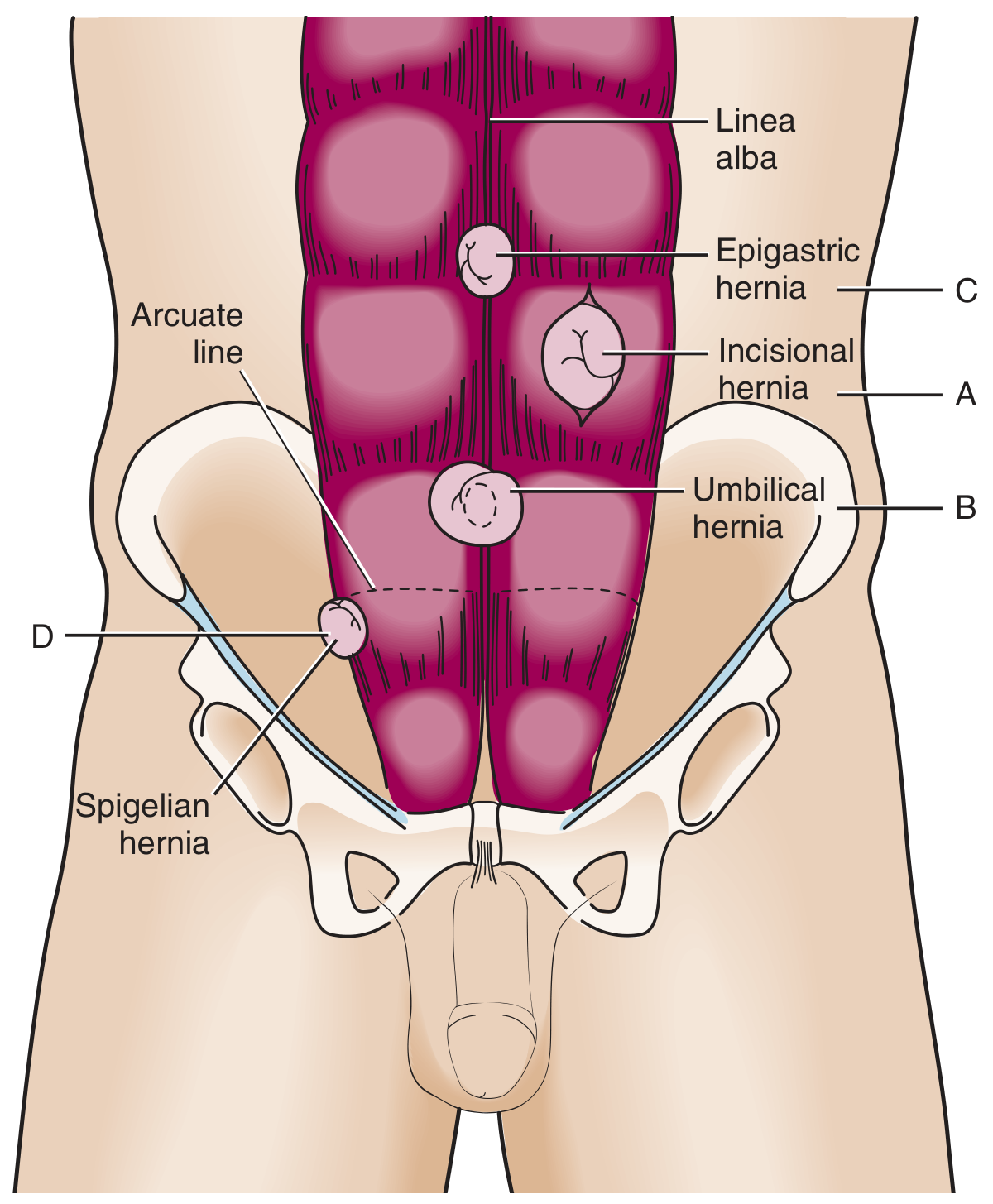
A. Umbilical Hernia
- Traverses the fibromuscular ring of the umbilicus
- Most common in infants/children; congenital in origin; often resolves by age 5
- If >2 cm, persists beyond age 5, or becomes incarcerated - surgical repair is indicated
- In adults, acquired form is associated with obesity, ascites, and pregnancy
B. Epigastric Hernia
- Occurs through the linea alba between the xiphoid and umbilicus
- Usually contains preperitoneal fat
- Often small and may present with localized pain without obvious bulge
C. Incisional Hernia
- Occurs through or near a previous surgical scar
- Affects up to 1 in 5 patients following abdominal surgery
- Poor wound healing (e.g., infection) increases risk
- Carries a recurrence rate of 20-50% after repair
- Larger defects have a lower incarceration risk (paradoxically, wide necks allow free movement)
D. Spigelian Hernia (Lateral Ventral Hernia)
- Located in the abdominal wall just lateral to the rectus abdominis muscle, along the Spigelian fascia
- Often difficult to diagnose clinically as it is interparietal (between layers of abdominal wall)
- High risk of incarceration due to small, rigid defect
2. Groin Hernias
A. Indirect Inguinal Hernia
- Most common type of hernia overall
- Passes through the internal (deep) inguinal ring and into the inguinal canal
- Located lateral to the inferior epigastric vessels
- Follows the path of testicular descent - caused by failure of the processus vaginalis to close
- More frequent in males; commonly diagnosed in children and young adults
- About 5% of full-term infants and 30% of preterm infants are affected
- Incarceration risk is especially high in infants <1 year old (30% incarcerate in children <3 months)
B. Direct Inguinal Hernia
- Protrudes directly through the posterior wall of the inguinal canal
- Located medial to the inferior epigastric vessels, within the inguinal (Hesselbach's) triangle
- Does NOT travel along the inguinal canal
- Acquired - caused by weakening of the myofascial wall due to aging and repetitive increased abdominal pressure
- Lower risk of incarceration because the orifice is typically wide
- Second most common groin hernia; more common with advancing age
C. Femoral Hernia
- Occurs inferior to the inguinal ligament, through a defect in the transversalis fascia
- Abdominal contents protrude into the femoral canal (medial to the femoral vein, lateral to the lacunar ligament)
- Presents as a medial thigh mass below where inguinal hernias are found
- Relatively uncommon; occurs more frequently in women
- Small fascial defect leads to incarceration in up to 45% of cases - highest incarceration risk of all groin hernias
D. Pantaloon Hernia
- A combination of both direct and indirect inguinal hernias occurring simultaneously (like trouser legs straddling the inferior epigastric vessels)
- Difficult to diagnose clinically in the ED; often discovered during surgical exploration
3. Internal Hernias
These occur within the abdominal cavity, through mesenteric defects or peritoneal recesses (e.g., foramen of Winslow, paraduodenal fossae). They are rare but can cause closed-loop bowel obstruction.
4. Diaphragmatic / Hiatal Hernias
- Hiatal hernia: Upper stomach (or intestine) protrudes into the chest through the oesophageal hiatus in the diaphragm
- Sliding type (Type I, ~95%): Gastro-oesophageal junction slides above the diaphragm - associated with GORD
- Rolling/Para-oesophageal type (Type II-IV): Fundus or other stomach structures herniate alongside a normally positioned GEJ - risk of volvulus and strangulation
Risk Factors
- Male sex (inguinal hernias particularly)
- Increased intraabdominal pressure: obesity, pregnancy, chronic cough, constipation, heavy lifting, ascites
- Aging (loss of tissue elasticity)
- Previous abdominal surgery (incisional hernia)
- Connective tissue disorders
- Prematurity (indirect inguinal hernia)
Key Anatomical Landmark: The Inguinal (Hesselbach's) Triangle
The inguinal triangle is bounded by:
- Inferiorly: Inguinal ligament
- Superolaterally: Inferior epigastric artery
- Medially: Lateral edge of rectus abdominis
Direct hernias occur within this triangle; indirect hernias occur lateral to it (through the deep ring). Femoral hernias are below the inguinal ligament.
Summary Table
| Hernia | Location | Common in | Incarceration Risk | Key Feature |
|---|---|---|---|---|
| Indirect inguinal | Through deep inguinal ring, lateral to epigastric vessels | Males, children | Moderate-high (infants) | Most common overall |
| Direct inguinal | Through posterior inguinal wall, medial to epigastric vessels | Older males | Low | Acquired; wide neck |
| Femoral | Below inguinal ligament, femoral canal | Women | Very high (~45%) | Rare but dangerous |
| Pantaloon | Both sides of epigastric vessels | Adults | Variable | Direct + indirect combined |
| Umbilical | Through umbilical ring | Infants, obese adults | Moderate | Congenital; may self-resolve |
| Epigastric | Linea alba above umbilicus | Adults | Low | Often small fat-only |
| Incisional | Through surgical scar | Post-op patients | Size-dependent | 20% of abdominal surgeries |
| Spigelian | Lateral border of rectus abdominis | Middle-aged adults | High | Interparietal; easy to miss |
| Hiatal | Stomach through oesophageal hiatus | Adults, obese | Low (sliding); higher (rolling) | GORD association |
Sources: Roberts and Hedges' Clinical Procedures in Emergency Medicine; Fischer's Mastery of Surgery, 8th ed.; Maingot's Abdominal Operations
This is a shared conversation. Sign in to Orris to start your own chat.