Treatment of malaria
Reading File
Finding Sources
Searching PubMed
"malaria"[MeSH Terms] AND "antimalarial"[MeSH Terms]
Searching the Web
WHO malaria treatment guidelines 2023 2024
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks. Here is the full structured answer:
Treatment of Malaria
Overview
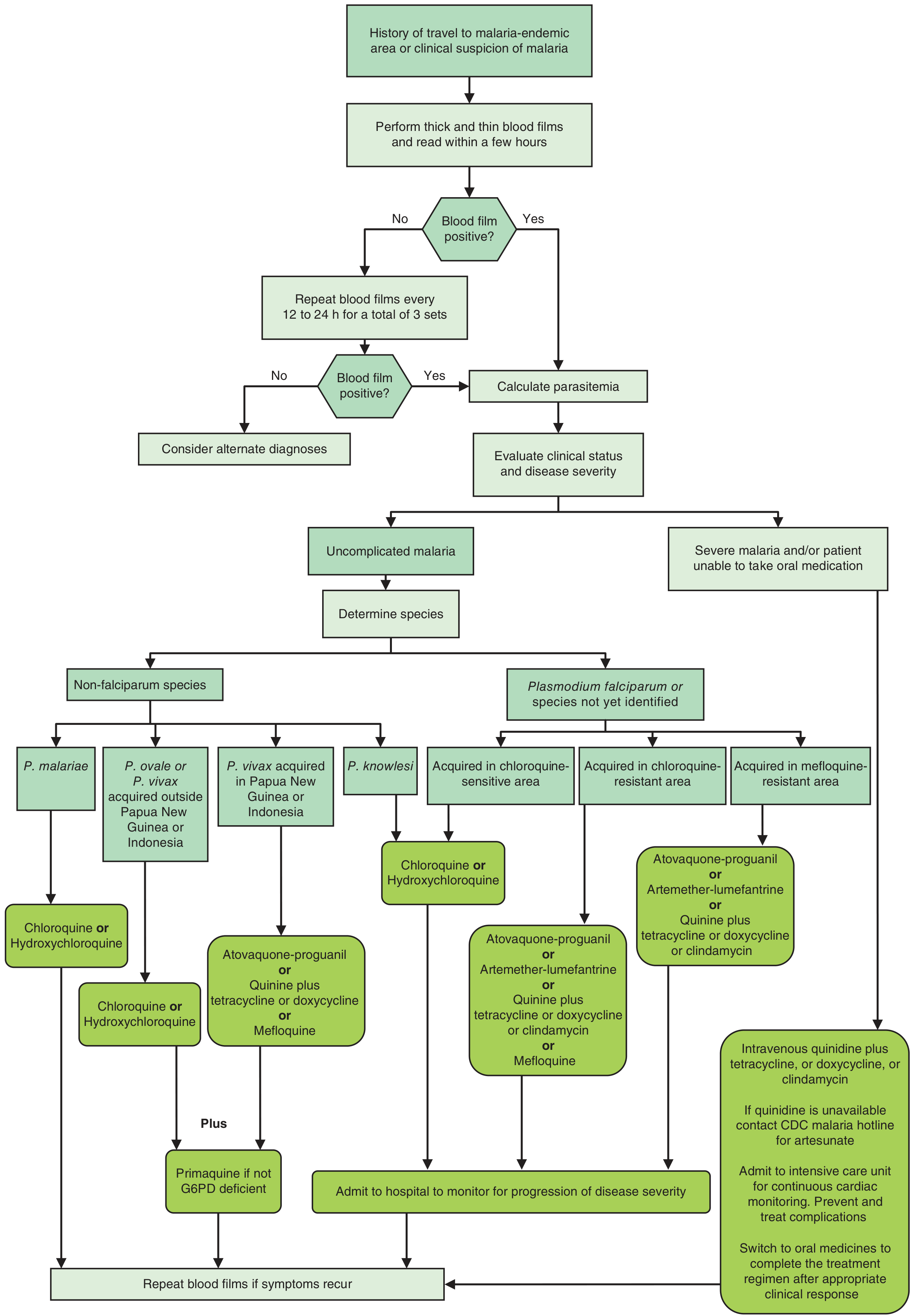
Treatment depends on three factors:
- Species - P. falciparum, P. vivax, P. ovale, P. malariae, or P. knowlesi
- Severity - uncomplicated vs. severe/complicated malaria
- Resistance pattern - chloroquine-sensitive vs. chloroquine/mefloquine-resistant area
All confirmed malaria cases (by microscopy or RDT) should receive prompt, effective treatment. - Park's Textbook of Preventive and Social Medicine, p. 307
1. Uncomplicated P. falciparum Malaria
A. Chloroquine-Sensitive Areas (rare globally)
| Drug | Dose |
|---|---|
| Chloroquine phosphate | 1 g, then 500 mg at 6, 24, and 48 hr |
B. Chloroquine-Resistant Areas (most of the world)
Artemisinin-based Combination Therapy (ACT) is the WHO-recommended first-line treatment. Artemisinin monotherapy alone is banned - it promotes resistance. - Park's, p. 307
Options (adult doses):
| Regimen | Dose |
|---|---|
| Artemether-lumefantrine (Coartem) | 4 tablets (artemether 20 mg + lumefantrine 120 mg) twice daily for 3 days |
| Atovaquone-proguanil (Malarone) | 4 tablets daily for 3 days |
| Artesunate + sulfadoxine-pyrimethamine (ACT-SP) | Artesunate x 3 days + SP single dose on Day 1; primaquine single dose 0.75 mg/kg on Day 2 |
| Artesunate-amodiaquine (ASAQ) | First-line in many African countries |
| Dihydroartemisinin-piperaquine | Highly effective; resistance seen in parts of Southeast Asia |
| Quinine sulfate 650 mg TID x 3-7 days | + doxycycline 100 mg BD x 7 days (or clindamycin 600 mg BD x 7 days for children/pregnant) |
| Mefloquine | 750 mg then 500 mg after 6-8 hr (or 1250 mg single dose) |
- Goldman-Cecil Medicine, Table 316-1 & 316-2, p. 3397
C. Mefloquine-Resistant Areas (parts of Southeast Asia)
- Atovaquone-proguanil, or
- Quinine + tetracycline/doxycycline/clindamycin
2. Uncomplicated P. vivax / P. ovale Malaria
- Chloroquine 25 mg/kg divided over 3 days (blood schizonticide) - Park's, p. 307
- PLUS Primaquine 0.25 mg/kg/day for 14 days (to eliminate hypnozoites and prevent relapse)
- Alternatively: Tafenoquine 300 mg single dose (anti-relapse)
- Relapse rate for vivax in India is ~30%; primaquine is essential to prevent it
Important: Primaquine/tafenoquine must ONLY be given after confirming normal G6PD levels - they cause haemolytic anaemia in G6PD-deficient patients. Contraindicated in pregnancy and infants. - Goldman-Cecil Medicine, p. 3397; Park's, p. 307
For P. vivax from Papua New Guinea or Indonesia (chloroquine resistance common): use atovaquone-proguanil or quinine + doxycycline/mefloquine.
3. P. malariae and P. knowlesi
- Treat with chloroquine (chloroquine-sensitive)
- No primaquine needed for P. malariae (no hypnozoite stage)
4. Severe / Complicated Malaria
Features Defining Severe Malaria
- Impaired consciousness/coma
- Repeated convulsions
- Renal failure (creatinine >3 mg/dL)
- Severe anaemia (Hb <5 g/dL)
- Pulmonary oedema/ARDS
- Hypoglycaemia (glucose <40 mg/dL)
- Circulatory collapse (systolic BP <80 mmHg)
- Haemoglobinuria
- Hyperparasitaemia (>5% parasitized RBCs)
- Park's, p. 308
Treatment of Severe Malaria (Parenteral First)
| Drug | Dose |
|---|---|
| IV Artesunate (preferred) | 2.4 mg/kg IV at 0, 12, 24 hr, then daily for 2 more days |
| IV Quinine dihydrochloride (if artesunate unavailable) | Loading dose 20 mg/kg over 4 hr; then 10 mg/kg every 8 hr (with cardiac monitoring) |
| IM Artemether | 3.2 mg/kg IM initially; then 1.6 mg/kg/day |
- IV artesunate is now clearly preferred over IV quinine for severe malaria - more efficacious and better tolerated. - Katzung's Basic and Clinical Pharmacology; Goldman-Cecil
- IV regimens should be maintained until oral therapy can be tolerated, then transitioned to a full oral ACT course (+ doxycycline or clindamycin)
- Admit to ICU with cardiac monitoring (especially if using quinine)
- Treat complications: hypoglycaemia, fluid balance, anaemia, seizures
5. Treatment in Pregnancy
| Trimester | P. falciparum | P. vivax |
|---|---|---|
| 1st trimester | Quinine + clindamycin (ACTs avoided) | Chloroquine |
| 2nd and 3rd trimester | ACT (artemether-lumefantrine preferred) | Chloroquine |
- Primaquine is contraindicated throughout pregnancy (risk of haemolysis in foetus)
- Severe malaria in pregnancy: IV artesunate following general severe malaria guidelines
- In lactating mothers, chloroquine/hydroxychloroquine are preferred; atovaquone-proguanil only if infant >5 kg with normal G6PD
- Goodman & Gilman's, p. 1322; Park's, p. 307
6. Treatment in Children
- Same regimens as adults (paediatric weight-based dosing; dose should never exceed adult dose)
- Tetracyclines contraindicated in children <8 years; use clindamycin instead
- Atovaquone-proguanil approved only for children >5 kg
- Goodman & Gilman's, p. 1322
7. Mixed Infections
- Treat as P. falciparum malaria (most aggressive species takes priority). - Park's, p. 307
8. Key Drugs - Quick Reference
| Drug | Class | Main Use | Key Toxicity |
|---|---|---|---|
| Artesunate / Artemether | Sesquiterpene lactone | Blood schizonticide; first-line severe disease | Generally well tolerated |
| Lumefantrine / Amodiaquine | ACT partner | Combined with artemisinin | GI side effects |
| Chloroquine | 4-aminoquinoline | Vivax/malariae/sensitive falciparum | Retinopathy (chronic); QTc prolongation |
| Primaquine | 8-aminoquinoline | Hypnozoite elimination (vivax/ovale) | Haemolysis in G6PD deficiency |
| Tafenoquine | 8-aminoquinoline | Relapse prevention (single dose) | Same as primaquine; contraindicated in G6PD deficiency |
| Quinine | Cinchona alkaloid | Severe disease; 1st trimester pregnancy | Cinchonism (tinnitus, nausea, dizziness); hypoglycaemia |
| Atovaquone-proguanil | Mixed | Resistant falciparum | GI intolerance; not in pregnancy |
| Mefloquine | 4-methanolquinoline | Resistant falciparum; prophylaxis | Neuropsychiatric effects; GI intolerance |
| Doxycycline | Tetracycline | Partner drug to quinine | Photosensitivity; contraindicated <8 yr, pregnancy |
9. Treatment Failure
Suspect if no clinical/parasitological response within 72 hours of full treatment with no vomiting. Treat with oral quinine + tetracycline/doxycycline. Report to the concerned malaria officer for therapeutic efficacy studies. - Park's, p. 307
10. WHO 2024 Update
The WHO Guidelines for Malaria (November 2024) are the most current consolidated guidance, including updated recommendations on:
- Malaria vaccines (RTS,S/AS01 and R21/Matrix-M)
- Use of near-patient G6PD tests to guide anti-relapse treatment
- Indoor residual spraying and spatial repellents (vector control)
The CDC Treatment Guidelines (June 2024) for uncomplicated and severe malaria are also available for US-specific practice.
Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics, p. 1322 | Goldman-Cecil Medicine, Tables 316-1 & 316-2 | Katzung's Basic and Clinical Pharmacology, 16th Ed. | Park's Textbook of Preventive and Social Medicine, pp. 307-308
This is a shared conversation. Sign in to Orris to start your own chat.