Brain anatomy
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I now have all the key images and content needed for a thorough brain anatomy overview. Here is the full response:
Brain Anatomy
The human brain weighs about 1.4 kg (3 pounds) and is the most complex structure in the known universe. It is divided into three major parts visible on gross inspection: the cerebrum, the brainstem, and the cerebellum.
1. Overall Lateral View
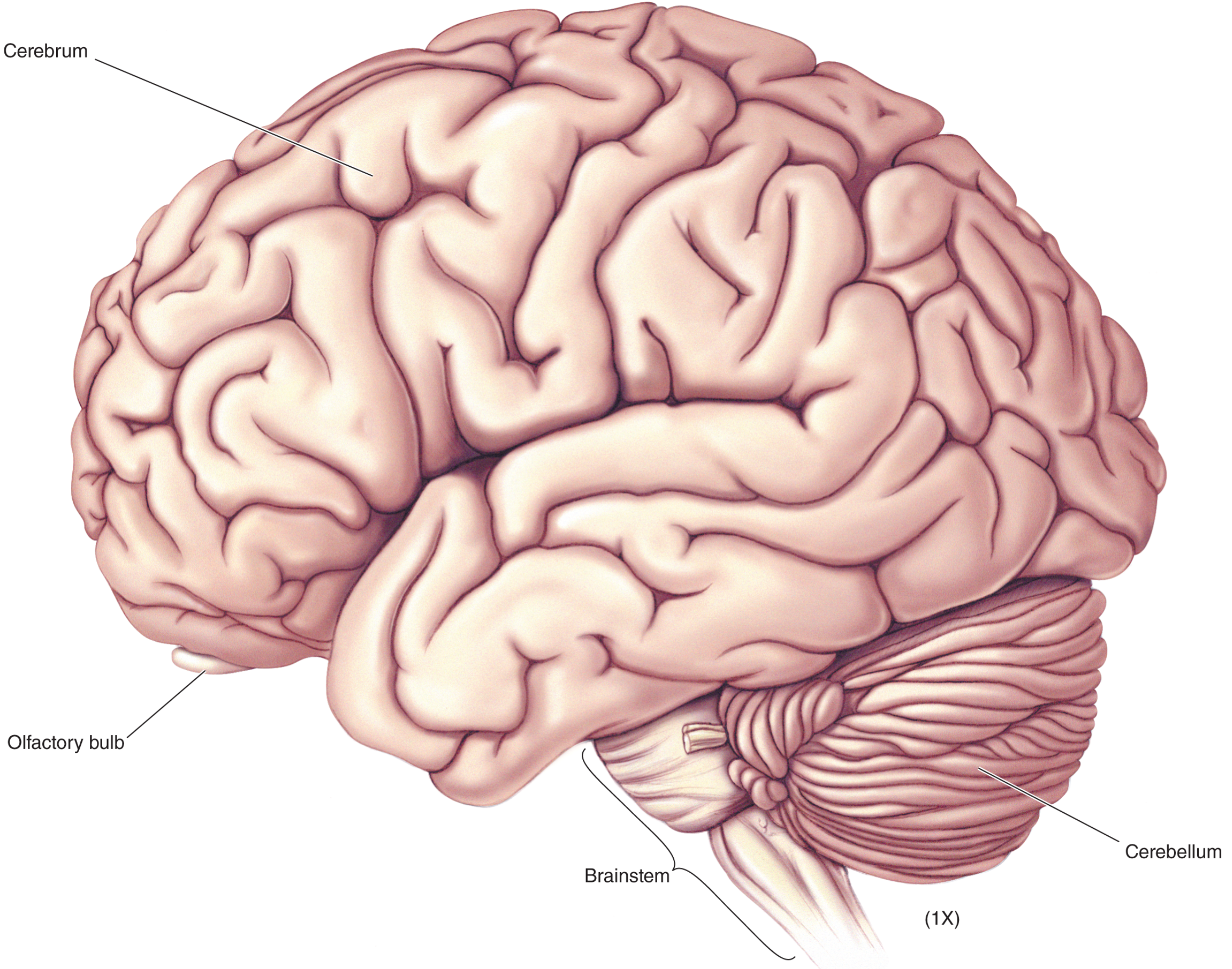
Lateral view (life-size). The three major divisions are immediately visible: the large convoluted cerebrum, the stalk-like brainstem, and the rippled cerebellum posteriorly. The small olfactory bulb is visible on the undersurface.
2. Surface Anatomy: Gyri, Sulci, and Key Landmarks
The cerebrum's surface is highly convoluted. The bumps are gyri, the grooves are sulci, and especially deep grooves are fissures.
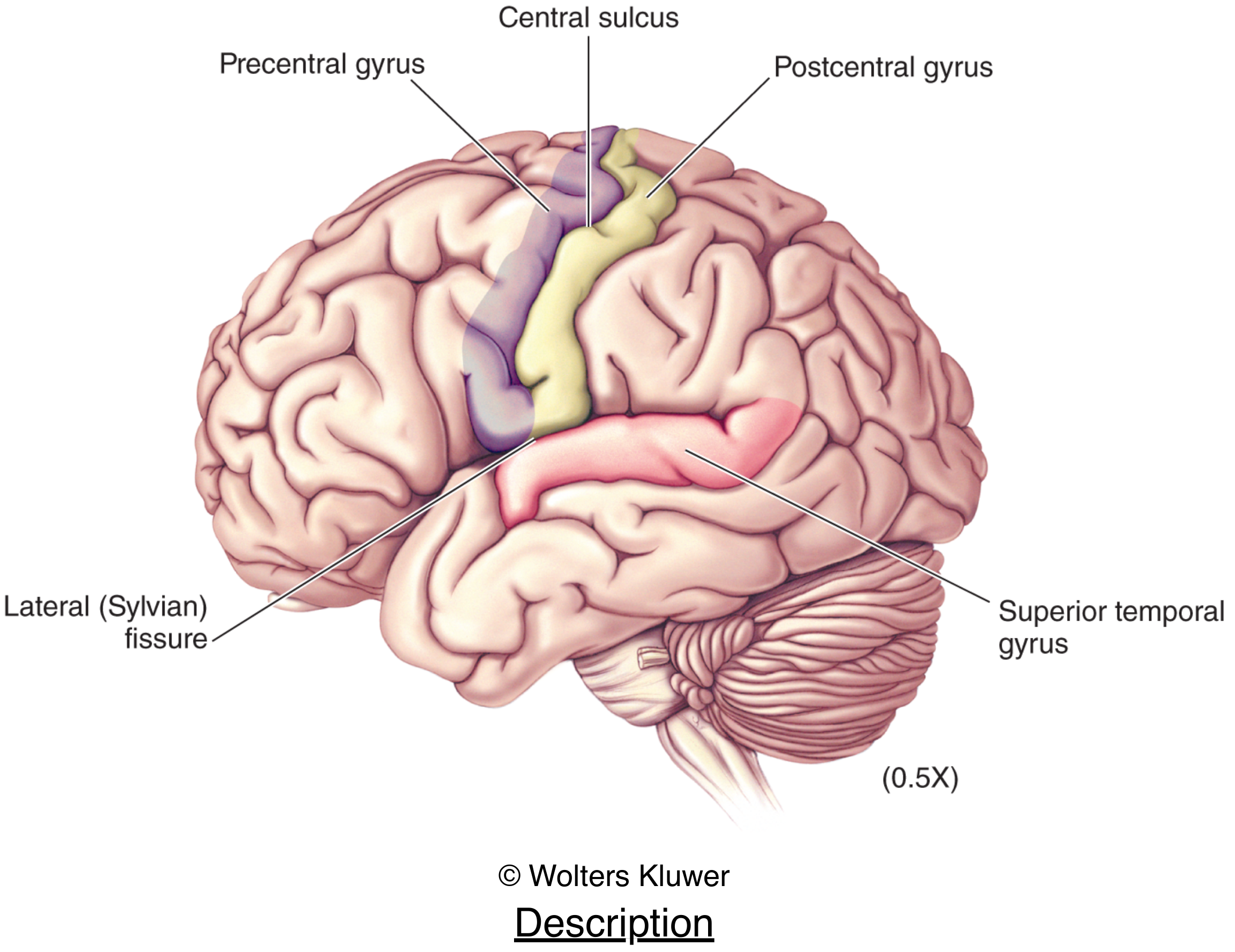
Key landmarks:
- Central sulcus - divides frontal from parietal lobe
- Precentral gyrus (anterior to central sulcus) - primary motor cortex
- Postcentral gyrus (posterior to central sulcus) - primary somatosensory cortex
- Lateral (Sylvian) fissure - separates frontal/parietal lobes from the temporal lobe
- Superior temporal gyrus - includes primary auditory cortex
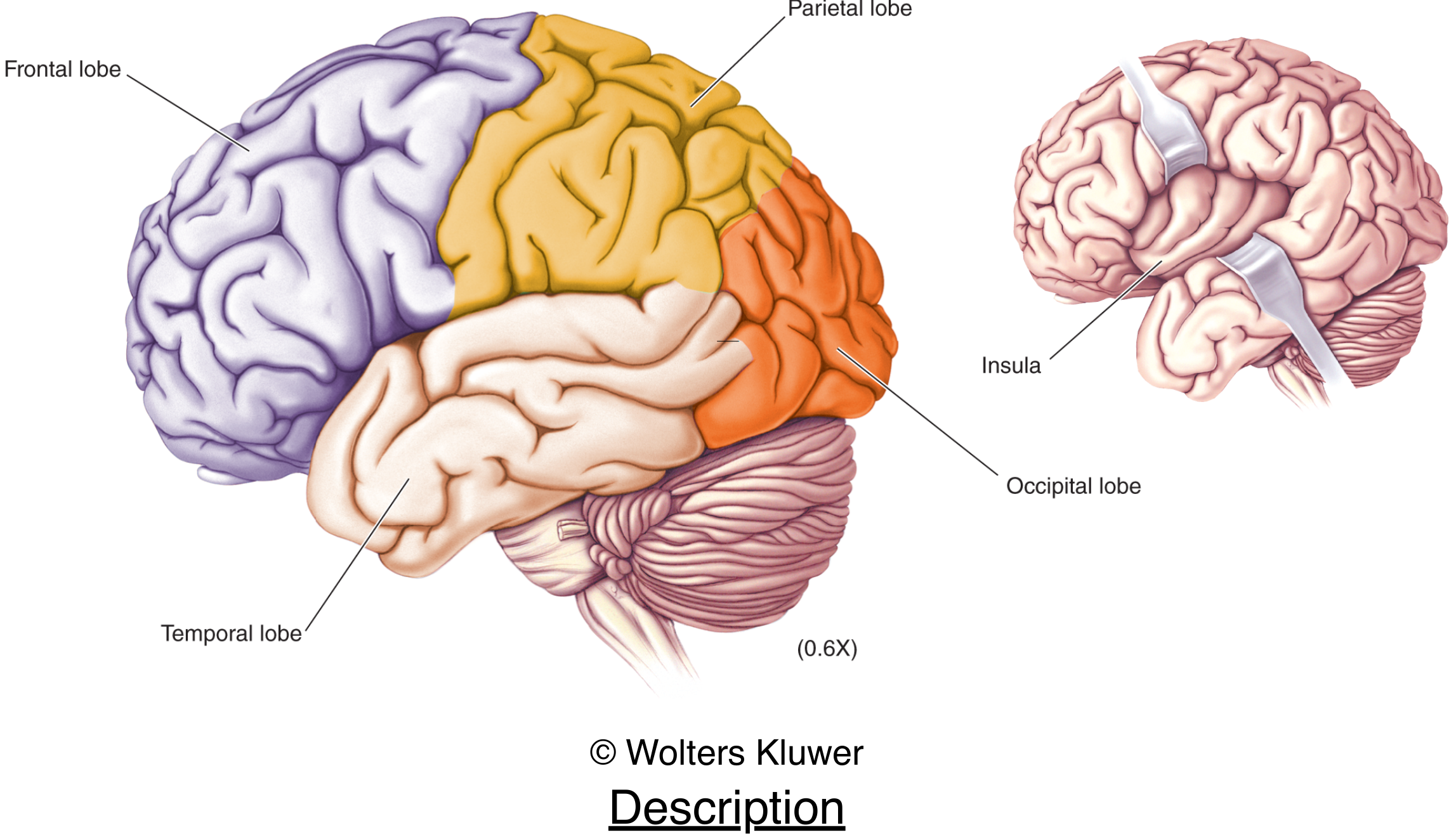
3. Cerebral Lobes
By convention the cerebrum is divided into lobes named after the overlying skull bones:
| Lobe | Location | Key functions |
|---|---|---|
| Frontal | Anterior; separated from parietal by central sulcus | Voluntary movement, executive function, language (Broca's area), personality |
| Parietal | Behind central sulcus | Somatic sensation, spatial processing, integration of sensory input |
| Temporal | Below Sylvian fissure | Hearing, memory, language comprehension (Wernicke's area) |
| Occipital | Posterior pole | Vision (primary visual cortex at calcarine fissure) |
| Insula | Buried deep in Sylvian fissure | Gustatory cortex (taste), interoception, pain processing |
4. Cortical Functional Areas (Brodmann's Map)
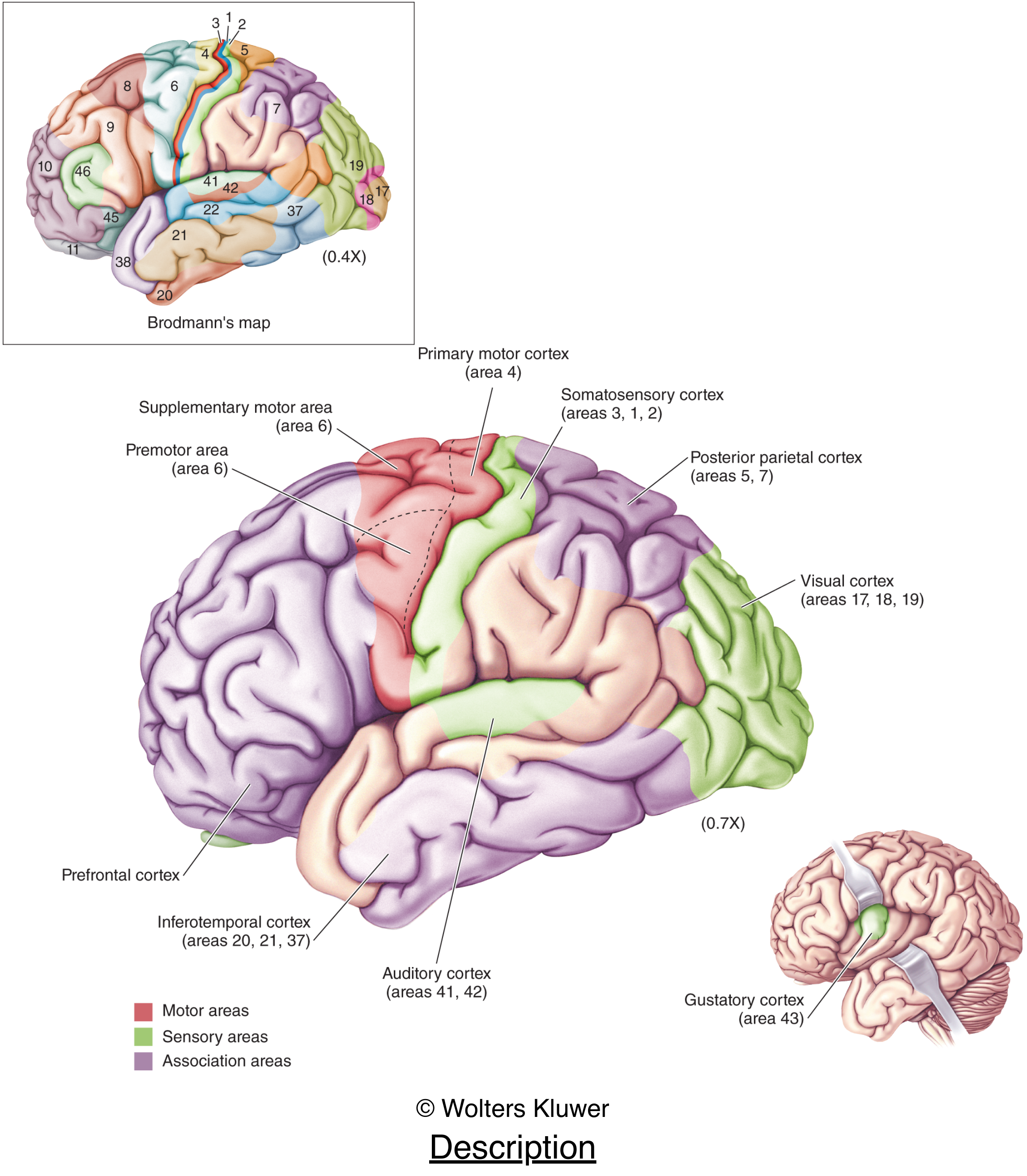
The cortex is organized into functional areas first mapped by Korbinian Brodmann using cytoarchitecture:
- Primary motor cortex - area 4 (precentral gyrus)
- Premotor / supplementary motor - area 6
- Primary somatosensory - areas 3, 1, 2 (postcentral gyrus)
- Posterior parietal cortex - areas 5, 7 (integration)
- Primary visual cortex - areas 17, 18, 19 (occipital)
- Primary auditory cortex - areas 41, 42 (superior temporal gyrus)
- Gustatory cortex - area 43 (operculum/insula)
- Prefrontal cortex - most of the frontal lobe anterior to motor areas
- Inferotemporal cortex - areas 20, 21, 37 (visual object recognition)
5. Medial Surface - Forebrain Structures
Slicing the brain in the midsagittal plane reveals important structures not visible from outside:
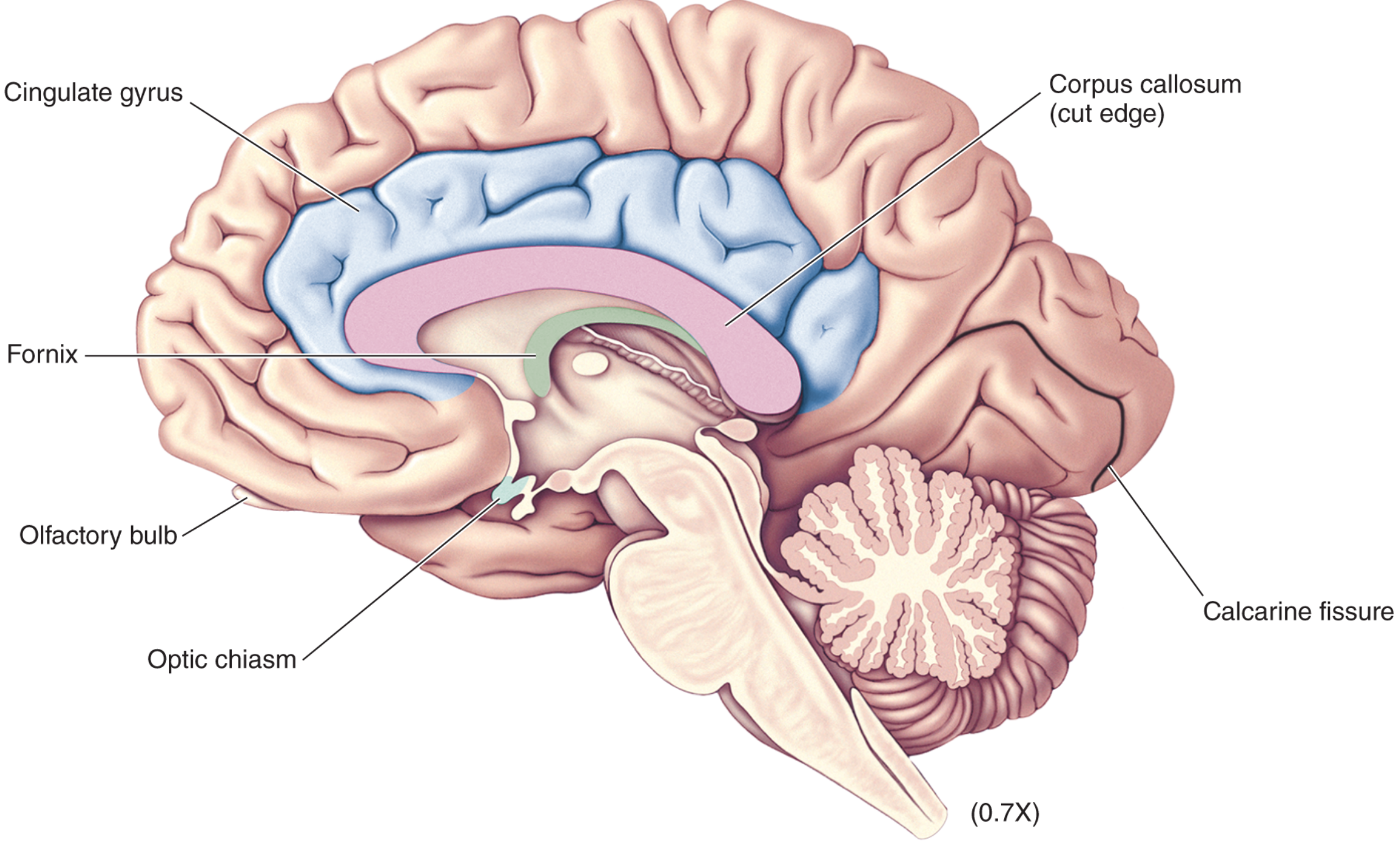
Key structures visible:
- Corpus callosum - the largest white-matter commissure; ~300 million axons connecting the two hemispheres
- Cingulate gyrus - part of the limbic system; involved in emotion and memory
- Fornix - fiber bundle connecting hippocampus to hypothalamus; critical for memory
- Optic chiasm - where nasal retinal fibers decussate
- Calcarine fissure - primary visual cortex lines its banks
6. Brainstem and Diencephalon (Medial View)
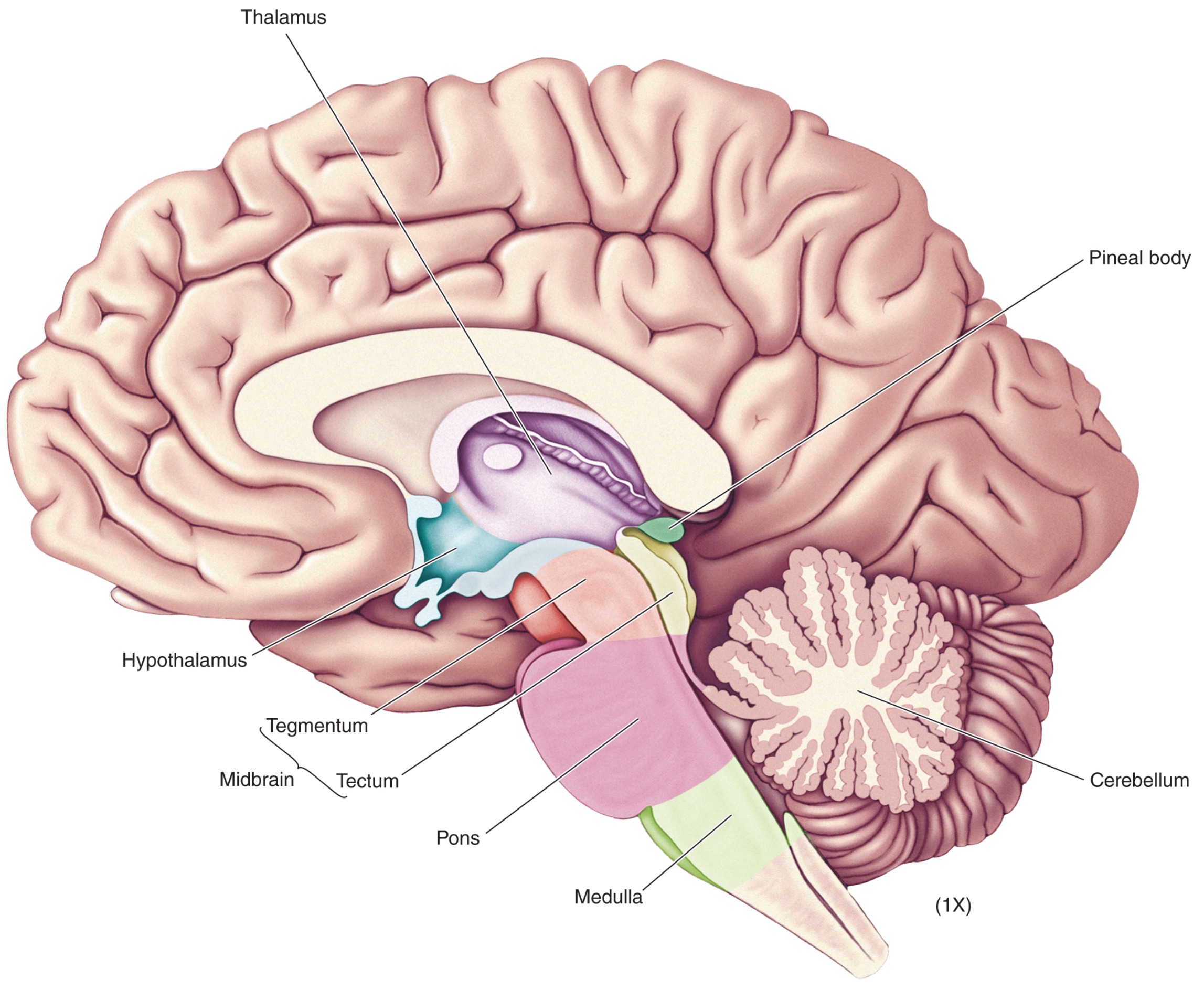
The brainstem (in the broad sense, including diencephalon) consists of:
Diencephalon
| Structure | Function |
|---|---|
| Thalamus | Relay station for nearly all sensory information en route to cortex; also involved in arousal/consciousness |
| Hypothalamus | Homeostatic regulation (temperature, hunger, thirst, circadian rhythm, autonomic control, pituitary hormone release) |
| Pineal body | Melatonin secretion; circadian rhythms |
Brainstem proper (midbrain, pons, medulla)
| Structure | Location | Key roles |
|---|---|---|
| Midbrain | Superior; includes tectum (superior/inferior colliculi) and tegmentum | Visual/auditory reflexes, eye movement (CN III, IV), dopamine (substantia nigra, VTA) |
| Pons | Middle; bulge on ventral surface | Contains nuclei for CN V, VI, VII, VIII; breathing rhythm; sleep regulation |
| Medulla oblongata | Inferior; merges with spinal cord | Vital autonomic centers (cardiovascular, respiratory); CN IX–XII; pyramidal decussation |
7. Cerebellum
Attached posteriorly to the brainstem via three peduncles:
- Superior cerebellar peduncle - output to thalamus and red nucleus
- Middle cerebellar peduncle - input from pontine nuclei (corticopontocerebellar tract)
- Inferior cerebellar peduncle - input/output to spinal cord and medulla
Functions: coordination of voluntary movement, balance, fine motor tuning, and motor learning. The cerebellar cortex has a characteristic three-layer structure (molecular, Purkinje, granular layers).
8. Ventricular System
The brain's CSF-filled cavities form a connected system:
| Ventricle | Location |
|---|---|
| Lateral ventricles (x2) | Deep in each cerebral hemisphere; bordered by thalamus and basal ganglia medially |
| 3rd ventricle | Midline; flanked by thalami on both sides |
| Cerebral aqueduct | Through the midbrain; connects 3rd and 4th ventricles |
| 4th ventricle | Between pons/medulla anteriorly and cerebellum posteriorly |
CSF exits the 4th ventricle via the foramina of Luschka (lateral) and Magendie (medial) into the subarachnoid space.
9. Deep Structures: Basal Ganglia and Limbic System
Basal ganglia (subcortical nuclei):
- Caudate nucleus, putamen (together = striatum), globus pallidus, subthalamic nucleus, substantia nigra
- Function: modulation of voluntary movement, habit learning, reward
Limbic system:
- Hippocampus - declarative memory formation (long-term memory)
- Amygdala - emotional processing (fear, threat detection)
- Cingulate gyrus, entorhinal cortex, parahippocampal gyrus
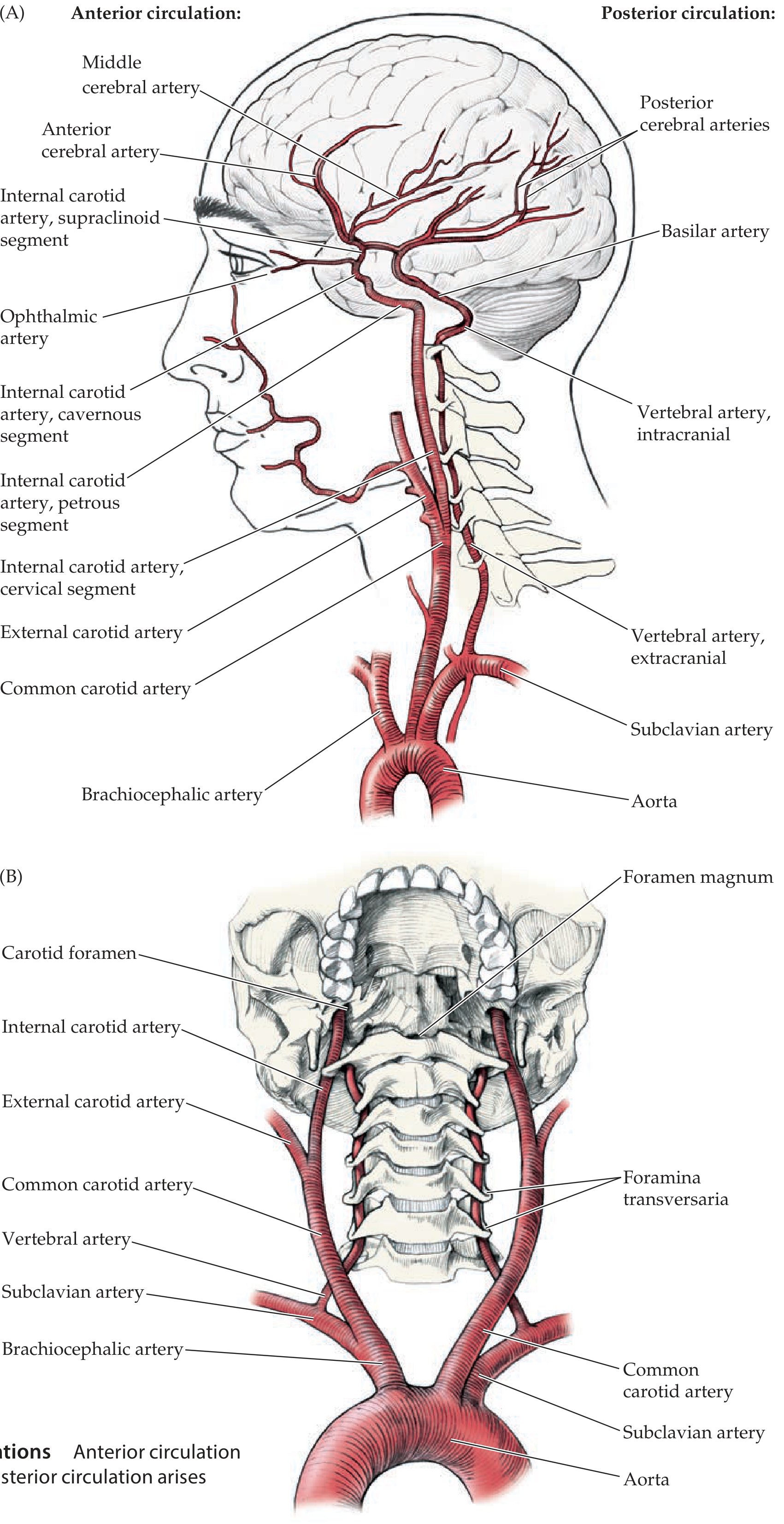
10. Blood Supply (Quick Summary)
The brain is supplied by two systems:
- Anterior circulation (internal carotid arteries) - anterior cerebral artery (ACA) and middle cerebral artery (MCA): supply the frontal, parietal, and temporal lobes
- Posterior circulation (vertebral arteries joining to form basilar artery) - posterior cerebral artery (PCA): supplies occipital lobe, inferior temporal lobe, thalamus, brainstem, and cerebellum
- These two systems anastomose at the Circle of Willis at the base of the brain
Sources: Neuroscience: Exploring the Brain, 5th Edition; Neuroanatomy through Clinical Cases, 3rd Edition; Gray's Anatomy for Students
Motor vs sensory cortex UMN vs LMN Cranial nerves (overview)
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
I now have everything needed. Here is the full, image-rich response:
Motor vs Sensory Cortex | UMN vs LMN | Cranial Nerves
Part 1: Motor Cortex vs Sensory Cortex
Location
Both the primary motor and primary somatosensory cortex flank the central sulcus:
| Cortex | Location | Brodmann Areas |
|---|---|---|
| Primary motor cortex | Precentral gyrus (anterior to central sulcus) | Area 4 |
| Primary somatosensory cortex | Postcentral gyrus (posterior to central sulcus) | Areas 3, 1, 2 |
The two are adjacent and heavily interconnected - somatosensory feedback from area 3a (muscle spindle input) projects directly to motor cortex and helps regulate precision of muscle contraction.
The Homunculus
Both cortices are somatotopically organized - adjacent body parts are represented by adjacent cortical regions. This is depicted by the famous homunculus ("little man"):
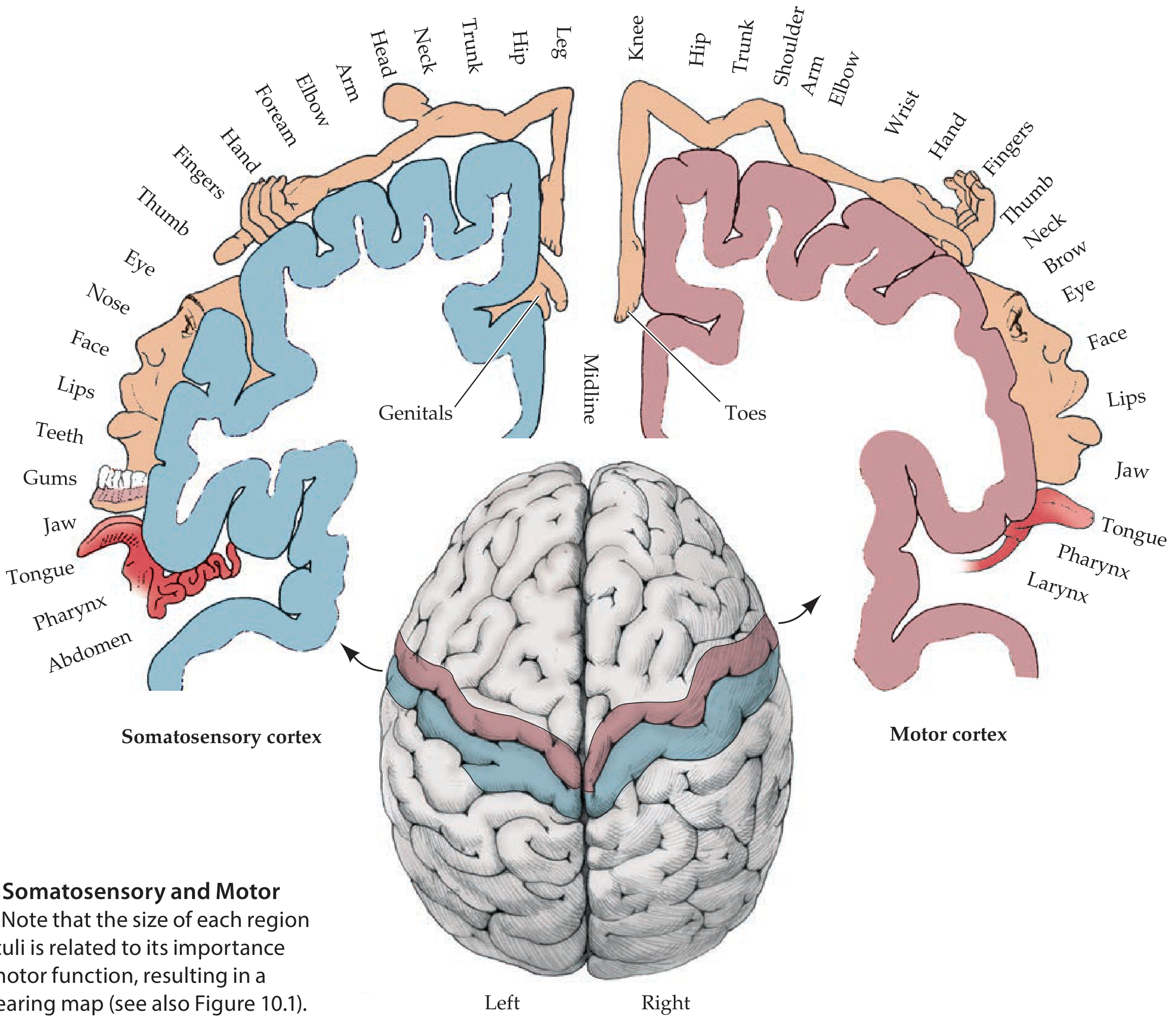
Key somatotopic rule: legs are represented medially (near the midline, tucking into the interhemispheric fissure), while face and hands are represented laterally on the convexity. The area of cortex devoted to a body part reflects its functional importance - hands, lips, and tongue have disproportionately large representations.
Functional Differences
| Feature | Primary Motor Cortex (M1) | Primary Somatosensory Cortex (S1) |
|---|---|---|
| Location | Precentral gyrus | Postcentral gyrus |
| Brodmann areas | 4 | 3, 1, 2 |
| Layer IV | Thin (sparse granular layer) | Thick (prominent granular layer) |
| Output | Commands voluntary movement via corticospinal tract | Processes touch, pressure, pain, temperature, proprioception from contralateral body |
| Key cell type | Giant Betz cells (layer V) projecting to spinal motor neurons | Stellate cells receiving thalamic (VPL nucleus) relay |
| Damage result | Contralateral weakness/paralysis | Contralateral loss of discriminative touch, proprioception, two-point discrimination |
Other Motor Areas (Frontal Lobe)
- Premotor cortex (area 6 lateral) - planning and sequencing movements
- Supplementary motor area (area 6 medial) - internally generated movements, bimanual coordination
- Broca's area (areas 44, 45) - language production (dominant hemisphere)
Part 2: Upper Motor Neuron (UMN) vs Lower Motor Neuron (LMN)
The Concept
The motor system operates as a two-neuron chain:
-
Upper motor neuron (UMN): Cell bodies in the motor cortex (and brainstem); axons travel in the corticospinal tract (pyramidal tract) down to the anterior horn of the spinal cord. For cranial nerve muscles, the analogous pathway is the corticobulbar tract projecting to cranial nerve motor nuclei.
-
Lower motor neuron (LMN): Cell bodies in the anterior horn of the spinal cord (or cranial nerve motor nuclei); axons travel via peripheral nerves directly to skeletal muscle. These are the "final common pathway."
Signs Compared
| Sign | UMN Lesion | LMN Lesion |
|---|---|---|
| Weakness | Yes | Yes |
| Muscle atrophy | No (mild disuse atrophy possible) | Yes (denervation atrophy) |
| Fasciculations | No | Yes (spontaneous anterior horn firing) |
| Tone | Increased (spasticity)* | Decreased (flaccidity) |
| Reflexes (DTRs) | Increased (hyperreflexia)* | Decreased/absent (hyporeflexia) |
| Babinski sign | Present (extensor plantar response) | Absent |
| Clonus | May be present | Absent |
*Note: With acute UMN lesions (e.g., acute stroke, spinal cord injury - "spinal shock"), tone and reflexes are initially decreased and only become increased over hours to months as spasticity develops.
Why Spasticity in UMN Lesions?
The corticospinal tract travels alongside descending inhibitory pathways to anterior horn interneurons. Damage to these inhibitory pathways (rather than the corticospinal tract alone) is what causes the disinhibited hyperreflexia and spasticity seen in UMN lesions.
Clinical Examples
| Condition | Type | Explanation |
|---|---|---|
| Stroke (motor cortex/internal capsule) | UMN | Affects corticospinal tract above anterior horn |
| Multiple sclerosis | UMN | Demyelination of white matter tracts |
| Amyotrophic lateral sclerosis (ALS) | Both UMN + LMN | Degenerates both motor neuron populations simultaneously |
| Polio | LMN | Virus destroys anterior horn cells |
| Peripheral nerve injury (e.g., radial nerve palsy) | LMN | Damages nerve distal to anterior horn |
| Guillain-Barre syndrome | LMN | Demyelination of peripheral nerves |
| Bell's palsy | LMN (CN VII) | Entire face involved ipsilaterally (including forehead) |
| Stroke affecting CN VII | UMN (CN VII) | Forehead spared (bilateral cortical representation) |
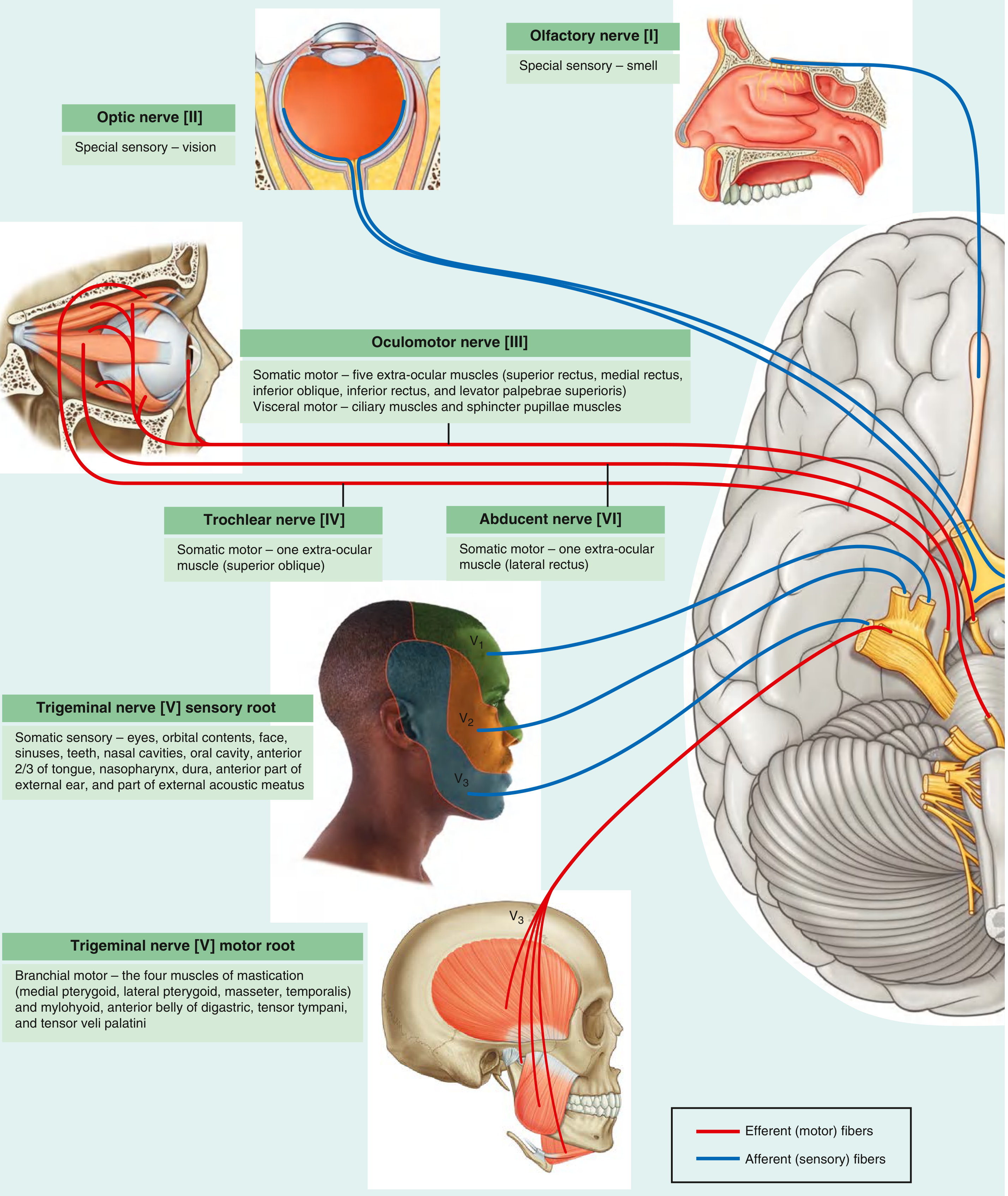
Part 3: Cranial Nerves - Overview
There are 12 pairs of cranial nerves, all emerging from the brainstem (except CN I from olfactory epithelium and CN II from retina). Each has a specific foraminal exit from the skull.
The 12 Cranial Nerves
| # | Name | Type | Key Function | Exit Foramen |
|---|---|---|---|---|
| I | Olfactory | Sensory | Smell | Cribriform plate |
| II | Optic | Sensory | Vision | Optic canal |
| III | Oculomotor | Motor | Eye movement (SR, MR, IR, IO, levator palpebrae); pupil constriction & accommodation (parasympathetics) | Superior orbital fissure |
| IV | Trochlear | Motor | Eye movement (superior oblique - intorts/depresses) | Superior orbital fissure |
| V | Trigeminal | Mixed | Face/scalp sensation (V1-V3); muscles of mastication (V3 only) | V1: SOF; V2: foramen rotundum; V3: foramen ovale |
| VI | Abducens | Motor | Eye movement (lateral rectus - abducts) | Superior orbital fissure |
| VII | Facial | Mixed | Muscles of facial expression; taste (anterior 2/3 tongue); lacrimation, salivation (submandibular/sublingual glands) | Internal acoustic meatus → stylomastoid foramen |
| VIII | Vestibulocochlear | Sensory | Hearing (cochlear); balance (vestibular) | Internal acoustic meatus |
| IX | Glossopharyngeal | Mixed | Taste/sensation (posterior 1/3 tongue, oropharynx); stylopharyngeus muscle; parotid secretion; carotid body/sinus | Jugular foramen |
| X | Vagus | Mixed | Pharynx/larynx sensation and muscle; parasympathetics to thorax/abdomen (heart, lungs, GI to splenic flexure); taste (epiglottis) | Jugular foramen |
| XI | Accessory | Motor | Sternocleidomastoid; upper trapezius | Jugular foramen |
| XII | Hypoglossal | Motor | All intrinsic and most extrinsic tongue muscles | Hypoglossal canal |
Mnemonic: Type (S=Sensory, M=Motor, B=Both)
"Some Say Marry Money But My Brother Says Big Brains Matter More"
S, S, M, M, B, M, B, S, B, B, M, M
Key Cranial Nerve Reflexes
| Reflex | Afferent (sensory) | Efferent (motor) |
|---|---|---|
| Corneal (blink) | CN V (ophthalmic V1) | CN VII (facial) |
| Pupillary light | CN II (optic) | CN III (oculomotor - parasympathetics) |
| Gag | CN IX (glossopharyngeal) | CN X (vagus) |
| Jaw-jerk | CN V (mandibular V3) | CN V (mandibular V3) |
Grouping by Brainstem Level
- Midbrain: CN III (oculomotor), CN IV (trochlear - only CN to exit dorsally)
- Pons: CN V (trigeminal), CN VI (abducens), CN VII (facial), CN VIII (vestibulocochlear)
- Medulla: CN IX, X, XI, XII
- Not from brainstem: CN I (olfactory epithelium → olfactory bulb), CN II (retina → optic chiasm)
Clinically Important Patterns
- Ptosis + dilated pupil + "down and out" eye - CN III palsy (posterior communicating artery aneurysm vs. diabetic microvascular ischemia - the latter is pupil-sparing)
- Horizontal diplopia - CN VI palsy (very sensitive to raised ICP due to its long intracranial course)
- Vertical diplopia, head tilt - CN IV palsy (most common cause: trauma)
- Complete ipsilateral facial weakness (including forehead) - LMN CN VII lesion (Bell's palsy, Lyme disease)
- Contralateral lower face weakness, forehead spared - UMN CN VII lesion (stroke) - forehead is spared because it has bilateral cortical representation
- Tongue deviates toward lesion on protrusion - CN XII palsy (genioglossus on intact side pushes tongue toward the damaged side)
Sources: Neuroanatomy through Clinical Cases, 3rd Ed.; Neuroscience: Exploring the Brain, 5th Ed.; Gray's Anatomy for Students; Rosen's Emergency Medicine, 9th Ed.
Create a clinical decision tool for UMN vs LMN diagnosis
Circle of willis
Finding Sources
Running Command
mkdir -p /tmp/workspace/clinical-tools && echo "done"
Finding Sources
Writing File
~/clinical-tools/umn-lmn-tool.html
<!DOCTYPE html>
<html lang="en">
<head>
<meta charset="UTF-8">
<meta name="viewport" content="width=device-width, initial-scale=1.0">
<title>UMN vs LMN Clinical Decision Tool</title>
<style>
:root {
--umn: #2563eb;
--lmn: #dc2626;
--both: #7c3aed;
--neutral: #374151;
--bg: #f8fafc;
--card: #ffffff;
--border: #e2e8f0;
--shadow: 0 2px 8px rgba(0,0,0,0.08);
}
* { box-sizing: border-box; margin: 0; padding: 0; }
body { font-family: 'Segoe UI', system-ui, sans-serif; background: var(--bg); color: var(--neutral); }
header {
background: linear-gradient(135deg, #1e3a5f 0%, #2563eb 100%);
color: white; padding: 24px 32px;
display: flex; align-items: center; gap: 16px;
}
header h1 { font-size: 1.6rem; font-weight: 700; }
header p { font-size: 0.9rem; opacity: 0.85; margin-top: 4px; }
.badge { background: rgba(255,255,255,0.2); border-radius: 20px; padding: 4px 12px; font-size: 0.75rem; font-weight: 600; }
.container { max-width: 1100px; margin: 0 auto; padding: 24px 16px; }
/* ---- CHECKER ---- */
.checker-card {
background: var(--card); border-radius: 16px; box-shadow: var(--shadow);
padding: 28px; margin-bottom: 28px; border: 1px solid var(--border);
}
.checker-card h2 { font-size: 1.15rem; font-weight: 700; margin-bottom: 6px; color: #1e3a5f; }
.checker-card p.subtitle { font-size: 0.85rem; color: #64748b; margin-bottom: 20px; }
.signs-grid {
display: grid; grid-template-columns: repeat(auto-fill, minmax(200px, 1fr));
gap: 12px; margin-bottom: 20px;
}
.sign-item {
background: #f1f5f9; border-radius: 10px; padding: 12px 14px;
display: flex; align-items: flex-start; gap: 10px; cursor: pointer;
border: 2px solid transparent; transition: all 0.18s;
}
.sign-item:hover { background: #e0e7ff; }
.sign-item.selected-umn { border-color: var(--umn); background: #eff6ff; }
.sign-item.selected-lmn { border-color: var(--lmn); background: #fff1f2; }
.sign-item label { font-size: 0.88rem; font-weight: 500; cursor: pointer; line-height: 1.4; }
.sign-item input[type="checkbox"] { margin-top: 2px; width: 16px; height: 16px; flex-shrink: 0; accent-color: var(--umn); }
.sign-tag { font-size: 0.7rem; font-weight: 700; padding: 1px 6px; border-radius: 10px; margin-left: auto; white-space: nowrap; }
.tag-umn { background: #dbeafe; color: var(--umn); }
.tag-lmn { background: #fee2e2; color: var(--lmn); }
.tag-both { background: #ede9fe; color: var(--both); }
.btn-row { display: flex; gap: 10px; flex-wrap: wrap; }
.btn { padding: 10px 22px; border-radius: 8px; border: none; cursor: pointer; font-size: 0.9rem; font-weight: 600; transition: 0.15s; }
.btn-primary { background: #1e3a5f; color: white; }
.btn-primary:hover { background: #2563eb; }
.btn-reset { background: #f1f5f9; color: #374151; border: 1px solid #e2e8f0; }
.btn-reset:hover { background: #e2e8f0; }
/* ---- RESULT ---- */
#result { margin-top: 20px; display: none; }
.result-box {
border-radius: 14px; padding: 22px 24px; border: 2px solid;
animation: fadeIn 0.3s ease;
}
@keyframes fadeIn { from { opacity:0; transform:translateY(6px); } to { opacity:1; transform:translateY(0); } }
.result-box.umn { border-color: var(--umn); background: #eff6ff; }
.result-box.lmn { border-color: var(--lmn); background: #fff1f2; }
.result-box.mixed { border-color: var(--both); background: #faf5ff; }
.result-box.unclear { border-color: #94a3b8; background: #f8fafc; }
.result-title { font-size: 1.3rem; font-weight: 800; display: flex; align-items: center; gap: 10px; }
.result-score { font-size: 0.88rem; color: #64748b; margin-top: 6px; margin-bottom: 14px; }
.result-hints { display: grid; grid-template-columns: 1fr 1fr; gap: 10px; margin-top: 12px; }
.hint { background: rgba(255,255,255,0.7); border-radius: 8px; padding: 10px 14px; font-size: 0.85rem; }
.hint strong { display: block; font-size: 0.78rem; text-transform: uppercase; letter-spacing: 0.05em; color: #64748b; margin-bottom: 3px; }
/* ---- COMPARISON TABLE ---- */
.section-title { font-size: 1.1rem; font-weight: 700; color: #1e3a5f; margin-bottom: 14px; display: flex; align-items: center; gap: 8px; }
table.comp { width: 100%; border-collapse: collapse; font-size: 0.9rem; }
table.comp th { padding: 10px 14px; text-align: left; font-size: 0.8rem; text-transform: uppercase; letter-spacing: 0.06em; background: #1e3a5f; color: white; }
table.comp th:first-child { border-radius: 8px 0 0 0; }
table.comp th:last-child { border-radius: 0 8px 0 0; }
table.comp td { padding: 10px 14px; border-bottom: 1px solid var(--border); vertical-align: top; }
table.comp tr:last-child td { border-bottom: none; }
table.comp tr:nth-child(even) td { background: #f8fafc; }
.umn-cell { color: var(--umn); font-weight: 600; }
.lmn-cell { color: var(--lmn); font-weight: 600; }
/* ---- TWO COLS ---- */
.two-cols { display: grid; grid-template-columns: 1fr 1fr; gap: 20px; margin-bottom: 28px; }
@media (max-width: 680px) { .two-cols { grid-template-columns: 1fr; } .result-hints { grid-template-columns: 1fr; } }
.info-card {
background: var(--card); border-radius: 14px; box-shadow: var(--shadow);
padding: 22px; border: 1px solid var(--border);
}
.info-card h3 { font-size: 0.95rem; font-weight: 700; margin-bottom: 12px; display: flex; align-items: center; gap: 6px; }
.info-card ul { list-style: none; padding: 0; }
.info-card li { padding: 6px 0; font-size: 0.86rem; border-bottom: 1px solid #f1f5f9; display: flex; gap: 8px; align-items: flex-start; }
.info-card li:last-child { border-bottom: none; }
.dot { width: 8px; height: 8px; border-radius: 50%; flex-shrink: 0; margin-top: 5px; }
.dot-umn { background: var(--umn); }
.dot-lmn { background: var(--lmn); }
.dot-both { background: var(--both); }
/* ---- PATHWAY DIAGRAM ---- */
.pathway { background: var(--card); border-radius: 14px; box-shadow: var(--shadow); padding: 24px; margin-bottom: 28px; border: 1px solid var(--border); }
.pathway-flow { display: flex; align-items: center; gap: 0; flex-wrap: wrap; justify-content: center; margin-top: 16px; }
.p-node {
background: #f1f5f9; border-radius: 10px; padding: 12px 16px; text-align: center;
font-size: 0.82rem; font-weight: 600; border: 2px solid var(--border); min-width: 110px;
}
.p-node.umn-node { background: #dbeafe; border-color: var(--umn); color: var(--umn); }
.p-node.lmn-node { background: #fee2e2; border-color: var(--lmn); color: var(--lmn); }
.p-node.muscle-node { background: #dcfce7; border-color: #16a34a; color: #15803d; }
.p-arrow { font-size: 1.4rem; color: #94a3b8; padding: 0 6px; }
.p-label { font-size: 0.72rem; color: #64748b; display: block; margin-top: 3px; font-weight: 400; }
/* ---- FOOTER ---- */
footer { text-align: center; padding: 20px; font-size: 0.8rem; color: #94a3b8; border-top: 1px solid var(--border); margin-top: 8px; }
.warning { background: #fffbeb; border: 1px solid #fcd34d; border-radius: 8px; padding: 10px 14px; font-size: 0.82rem; color: #92400e; margin-top: 16px; }
</style>
</head>
<body>
<header>
<div>
<h1>🧠 UMN vs LMN Clinical Decision Tool</h1>
<p>Upper Motor Neuron & Lower Motor Neuron lesion differentiation — based on clinical signs</p>
</div>
<span class="badge">Neurology</span>
</header>
<div class="container">
<!-- CHECKER -->
<div class="checker-card">
<h2>Clinical Sign Checker</h2>
<p class="subtitle">Select all signs present in your patient. The tool will suggest the most likely lesion type.</p>
<div class="signs-grid" id="signsGrid">
<!-- filled by JS -->
</div>
<div class="btn-row">
<button class="btn btn-primary" onclick="assess()">Assess Findings</button>
<button class="btn btn-reset" onclick="resetAll()">Reset</button>
</div>
<div id="result">
<div class="result-box" id="resultBox">
<div class="result-title" id="resultTitle"></div>
<div class="result-score" id="resultScore"></div>
<div class="result-hints" id="resultHints"></div>
</div>
<div class="warning">⚠️ This tool is an educational aid only. Clinical judgment, history, and investigations are required for diagnosis.</div>
</div>
</div>
<!-- MOTOR PATHWAY -->
<div class="pathway">
<div class="section-title">⬇️ The Two-Neuron Motor Pathway</div>
<div class="pathway-flow">
<div class="p-node">Motor Cortex<br><span class="p-label">(Precentral gyrus)</span></div>
<span class="p-arrow">→</span>
<div class="p-node umn-node">UMN Axon<br><span class="p-label">Corticospinal / corticobulbar tract</span></div>
<span class="p-arrow">→</span>
<div class="p-node">Anterior Horn<br><span class="p-label">Spinal cord (or CN nucleus)</span></div>
<span class="p-arrow">→</span>
<div class="p-node lmn-node">LMN Axon<br><span class="p-label">Peripheral nerve</span></div>
<span class="p-arrow">→</span>
<div class="p-node muscle-node">Skeletal Muscle<br><span class="p-label">Neuromuscular junction</span></div>
</div>
<p style="text-align:center; font-size:0.8rem; color:#64748b; margin-top:14px;">
Lesion <strong>above</strong> the anterior horn → <span style="color:var(--umn); font-weight:700;">UMN signs</span> |
Lesion <strong>at or below</strong> the anterior horn → <span style="color:var(--lmn); font-weight:700;">LMN signs</span>
</p>
</div>
<!-- COMPARISON TABLE -->
<div class="checker-card" style="margin-bottom:28px;">
<div class="section-title">📋 Full Comparison Table</div>
<table class="comp">
<thead>
<tr>
<th>Sign / Feature</th>
<th>UMN Lesion</th>
<th>LMN Lesion</th>
<th>Notes</th>
</tr>
</thead>
<tbody>
<tr><td><strong>Weakness</strong></td><td class="umn-cell">Yes</td><td class="lmn-cell">Yes</td><td>Both cause weakness — not discriminating alone</td></tr>
<tr><td><strong>Muscle tone</strong></td><td class="umn-cell">↑ Spasticity</td><td class="lmn-cell">↓ Flaccidity</td><td>Acutely, UMN may show flaccid paralysis ("spinal shock")</td></tr>
<tr><td><strong>Deep tendon reflexes</strong></td><td class="umn-cell">↑ Hyperreflexia</td><td class="lmn-cell">↓ Hyporeflexia / absent</td><td>Acutely, UMN reflexes may be reduced</td></tr>
<tr><td><strong>Babinski sign</strong></td><td class="umn-cell">Present (extensor plantar)</td><td class="lmn-cell">Absent</td><td>Most specific UMN sign</td></tr>
<tr><td><strong>Clonus</strong></td><td class="umn-cell">May be present</td><td class="lmn-cell">Absent</td><td>Sustained clonus strongly suggests UMN</td></tr>
<tr><td><strong>Muscle atrophy</strong></td><td class="umn-cell">Absent (mild disuse atrophy possible)</td><td class="lmn-cell">Present (denervation)</td><td>LMN atrophy is more rapid and prominent</td></tr>
<tr><td><strong>Fasciculations</strong></td><td class="umn-cell">Absent</td><td class="lmn-cell">Present</td><td>Spontaneous anterior horn cell firing</td></tr>
<tr><td><strong>Distribution</strong></td><td class="umn-cell">Pyramidal pattern: arm flexors > extensors; leg extensors > flexors</td><td class="lmn-cell">Follows myotome or peripheral nerve territory</td><td>Key for localization</td></tr>
<tr><td><strong>Pattern (face CN VII)</strong></td><td class="umn-cell">Lower face only (forehead spared — bilateral UMN supply)</td><td class="lmn-cell">Entire face (including forehead)</td><td>Important stroke vs Bell's palsy distinction</td></tr>
<tr><td><strong>Hoffmann's sign</strong></td><td class="umn-cell">Present</td><td class="lmn-cell">Absent</td><td>Upper limb equivalent of Babinski</td></tr>
<tr><td><strong>Coordination</strong></td><td class="umn-cell">Impaired (if cerebellar tracts also affected)</td><td class="lmn-cell">Impaired by weakness, not cerebellar</td><td></td></tr>
<tr><td><strong>Location of lesion</strong></td><td class="umn-cell">Brain, brainstem, or spinal cord (above anterior horn)</td><td class="lmn-cell">Anterior horn, nerve root, peripheral nerve, NMJ</td><td></td></tr>
</tbody>
</table>
</div>
<!-- EXAMPLES -->
<div class="two-cols">
<div class="info-card">
<h3 style="color:var(--umn);">🔵 UMN Conditions</h3>
<ul>
<li><span class="dot dot-umn"></span><div><strong>Stroke</strong> — MCA territory most common; contralateral hemiplegia</div></li>
<li><span class="dot dot-umn"></span><div><strong>Multiple Sclerosis</strong> — white matter demyelination; relapsing-remitting</div></li>
<li><span class="dot dot-umn"></span><div><strong>Spinal cord compression</strong> — bilateral UMN below lesion level</div></li>
<li><span class="dot dot-umn"></span><div><strong>Cerebral palsy</strong> — perinatal corticospinal tract injury</div></li>
<li><span class="dot dot-umn"></span><div><strong>Primary lateral sclerosis</strong> — pure UMN variant of MND</div></li>
<li><span class="dot dot-umn"></span><div><strong>Syringomyelia</strong> — UMN below syrinx level</div></li>
<li><span class="dot dot-both"></span><div><strong>ALS</strong> — both UMN + LMN signs simultaneously</div></li>
</ul>
</div>
<div class="info-card">
<h3 style="color:var(--lmn);">🔴 LMN Conditions</h3>
<ul>
<li><span class="dot dot-lmn"></span><div><strong>Bell's palsy</strong> — CN VII; complete ipsilateral facial weakness incl. forehead</div></li>
<li><span class="dot dot-lmn"></span><div><strong>Peripheral neuropathy</strong> — GBS, diabetic, toxic</div></li>
<li><span class="dot dot-lmn"></span><div><strong>Poliomyelitis</strong> — anterior horn cell destruction; no sensory loss</div></li>
<li><span class="dot dot-lmn"></span><div><strong>Radiculopathy</strong> — nerve root compression (disc herniation)</div></li>
<li><span class="dot dot-lmn"></span><div><strong>Spinal muscular atrophy (SMA)</strong> — anterior horn cell degeneration</div></li>
<li><span class="dot dot-lmn"></span><div><strong>Mononeuropathy</strong> — radial nerve palsy, carpal tunnel</div></li>
<li><span class="dot dot-lmn"></span><div><strong>Myasthenia gravis</strong> — NMJ (fatigable weakness, no atrophy/fasciculations)</div></li>
</ul>
</div>
</div>
<!-- LOCALIZATION TIP -->
<div class="checker-card">
<div class="section-title">📍 Lesion Localization Guide</div>
<table class="comp">
<thead>
<tr><th>Pattern</th><th>Likely Location</th><th>Key Features</th></tr>
</thead>
<tbody>
<tr><td>Contralateral face + arm + leg UMN</td><td>Internal capsule / corona radiata (stroke)</td><td>Contralateral hemisensory loss if posterior limb involved</td></tr>
<tr><td>Ipsilateral CN palsy + contralateral limb UMN</td><td>Brainstem (crossed syndrome)</td><td>e.g., Weber's syndrome (ipsilateral CN III + contralateral hemiplegia)</td></tr>
<tr><td>Bilateral UMN below a level</td><td>Spinal cord</td><td>Paraplegia/quadriplegia; sensory level; bladder/bowel involvement</td></tr>
<tr><td>UMN + LMN at same level</td><td>Anterior horn + corticospinal tract</td><td>Think ALS; also consider cervical myelopathy with radiculopathy</td></tr>
<tr><td>Dermatomal sensory loss + LMN in myotome</td><td>Nerve root (radiculopathy)</td><td>Disc herniation, foraminal stenosis</td></tr>
<tr><td>LMN following peripheral nerve distribution</td><td>Peripheral nerve (mononeuropathy)</td><td>Trauma, compression, entrapment</td></tr>
<tr><td>Distal > proximal LMN; stocking-glove sensory loss</td><td>Peripheral neuropathy (polyneuropathy)</td><td>Diabetes, alcohol, GBS (ascending)</td></tr>
<tr><td>Complete unilateral facial weakness (incl. forehead)</td><td>LMN CN VII (facial nerve)</td><td>Bell's palsy, Lyme disease, parotid tumor</td></tr>
<tr><td>Unilateral lower facial weakness (forehead spared)</td><td>UMN CN VII (contralateral hemisphere)</td><td>Stroke, tumor</td></tr>
</tbody>
</table>
</div>
</div>
<footer>
Clinical Decision Tool — For educational use. Based on <em>Neuroanatomy through Clinical Cases, 3rd Ed.</em> & <em>Ganong's Review of Medical Physiology</em>. Not a substitute for clinical judgment.
</footer>
<script>
const signs = [
{ id: 'spasticity', label: 'Increased tone (spasticity)', type: 'umn' },
{ id: 'hyperreflexia', label: 'Hyperreflexia (brisk DTRs)', type: 'umn' },
{ id: 'babinski', label: 'Babinski sign present', type: 'umn' },
{ id: 'clonus', label: 'Clonus', type: 'umn' },
{ id: 'hoffmann', label: "Hoffmann's sign", type: 'umn' },
{ id: 'forehead_spare', label: 'Forehead spared (facial)', type: 'umn' },
{ id: 'pyramidal', label: 'Pyramidal weakness pattern', type: 'umn' },
{ id: 'flaccid', label: 'Decreased tone (flaccidity)', type: 'lmn' },
{ id: 'hyporeflexia', label: 'Hyporeflexia / absent reflexes', type: 'lmn' },
{ id: 'atrophy', label: 'Muscle atrophy', type: 'lmn' },
{ id: 'fasciculations', label: 'Fasciculations', type: 'lmn' },
{ id: 'forehead_all', label: 'Full face weak (incl. forehead)', type: 'lmn' },
{ id: 'nerve_dist', label: 'Nerve/dermatomal distribution', type: 'lmn' },
{ id: 'weakness', label: 'Weakness (non-specific)', type: 'both' },
];
const grid = document.getElementById('signsGrid');
signs.forEach(s => {
const div = document.createElement('div');
div.className = 'sign-item';
div.id = 'item_' + s.id;
const tagClass = s.type === 'umn' ? 'tag-umn' : s.type === 'lmn' ? 'tag-lmn' : 'tag-both';
const tagLabel = s.type === 'umn' ? 'UMN' : s.type === 'lmn' ? 'LMN' : 'Both';
div.innerHTML = `
<input type="checkbox" id="chk_${s.id}">
<label for="chk_${s.id}">${s.label}</label>
<span class="sign-tag ${tagClass}">${tagLabel}</span>`;
div.querySelector('input').addEventListener('change', function() {
div.classList.remove('selected-umn','selected-lmn');
if (this.checked) {
div.classList.add(s.type === 'lmn' ? 'selected-lmn' : 'selected-umn');
}
});
grid.appendChild(div);
});
function assess() {
let umnScore = 0, lmnScore = 0;
const umnSigns = [], lmnSigns = [];
signs.forEach(s => {
const chk = document.getElementById('chk_' + s.id);
if (chk && chk.checked) {
if (s.type === 'umn') { umnScore += 2; umnSigns.push(s.label); }
else if (s.type === 'lmn') { lmnScore += 2; lmnSigns.push(s.label); }
else { umnScore += 0.5; lmnScore += 0.5; }
}
});
const resultDiv = document.getElementById('result');
const box = document.getElementById('resultBox');
const title = document.getElementById('resultTitle');
const score = document.getElementById('resultScore');
const hints = document.getElementById('resultHints');
resultDiv.style.display = 'block';
box.className = 'result-box';
if (umnScore === 0 && lmnScore === 0) {
box.classList.add('unclear');
title.innerHTML = '⬜ No discriminating signs selected';
score.textContent = 'Select clinical signs above to see an assessment.';
hints.innerHTML = '';
return;
}
let verdict, cls, icon, nextSteps, differential;
if (umnScore > 0 && lmnScore > 0 && Math.abs(umnScore - lmnScore) <= 2) {
cls = 'mixed'; icon = '🟣';
verdict = 'Mixed UMN + LMN Pattern';
nextSteps = 'Consider ALS / MND, cervical myelopathy with radiculopathy, or a multi-level lesion.';
differential = 'ALS, cervical spondylotic myelopathy, subacute combined degeneration, syringomyelia with cord expansion.';
} else if (umnScore > lmnScore) {
cls = 'umn'; icon = '🔵';
verdict = 'Likely Upper Motor Neuron (UMN) Lesion';
nextSteps = 'Localise above the anterior horn: brain (cortex, internal capsule, brainstem) or spinal cord. MRI brain ± spine.';
differential = 'Stroke, MS, spinal cord compression, cerebral palsy, tumour, TBI.';
} else {
cls = 'lmn'; icon = '🔴';
verdict = 'Likely Lower Motor Neuron (LMN) Lesion';
nextSteps = 'Localise at/below anterior horn: nerve root, plexus, peripheral nerve, NMJ, or muscle. EMG/NCS often indicated.';
differential = 'Radiculopathy, peripheral neuropathy, GBS, polio, MND (LMN variant), Bell\'s palsy.';
}
box.classList.add(cls);
title.innerHTML = `${icon} ${verdict}`;
score.innerHTML = `UMN signs: <strong>${umnScore > 0 ? umnSigns.length : 0}</strong> | LMN signs: <strong>${lmnScore > 0 ? lmnSigns.length : 0}</strong>`;
hints.innerHTML = `
<div class="hint"><strong>Next steps</strong>${nextSteps}</div>
<div class="hint"><strong>Differential diagnosis</strong>${differential}</div>`;
}
function resetAll() {
signs.forEach(s => {
const chk = document.getElementById('chk_' + s.id);
if (chk) chk.checked = false;
const item = document.getElementById('item_' + s.id);
if (item) item.classList.remove('selected-umn','selected-lmn');
});
document.getElementById('result').style.display = 'none';
}
</script>
</body>
</html>
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Loading Image
UMN vs LMN Clinical Decision Tool
Here is the interactive tool - open it in your browser:
umn lmn tool
HTML File · HTML
The tool includes:
- Sign checker - tick present signs, get an instant UMN / LMN / Mixed assessment with differential diagnosis
- Two-neuron motor pathway diagram
- Full comparison table (tone, reflexes, atrophy, fasciculations, Babinski, Hoffmann's, distribution pattern)
- Localization guide - maps sign patterns to lesion locations (internal capsule, brainstem, spinal cord, nerve root, peripheral nerve)
- Clinical examples for both UMN and LMN conditions
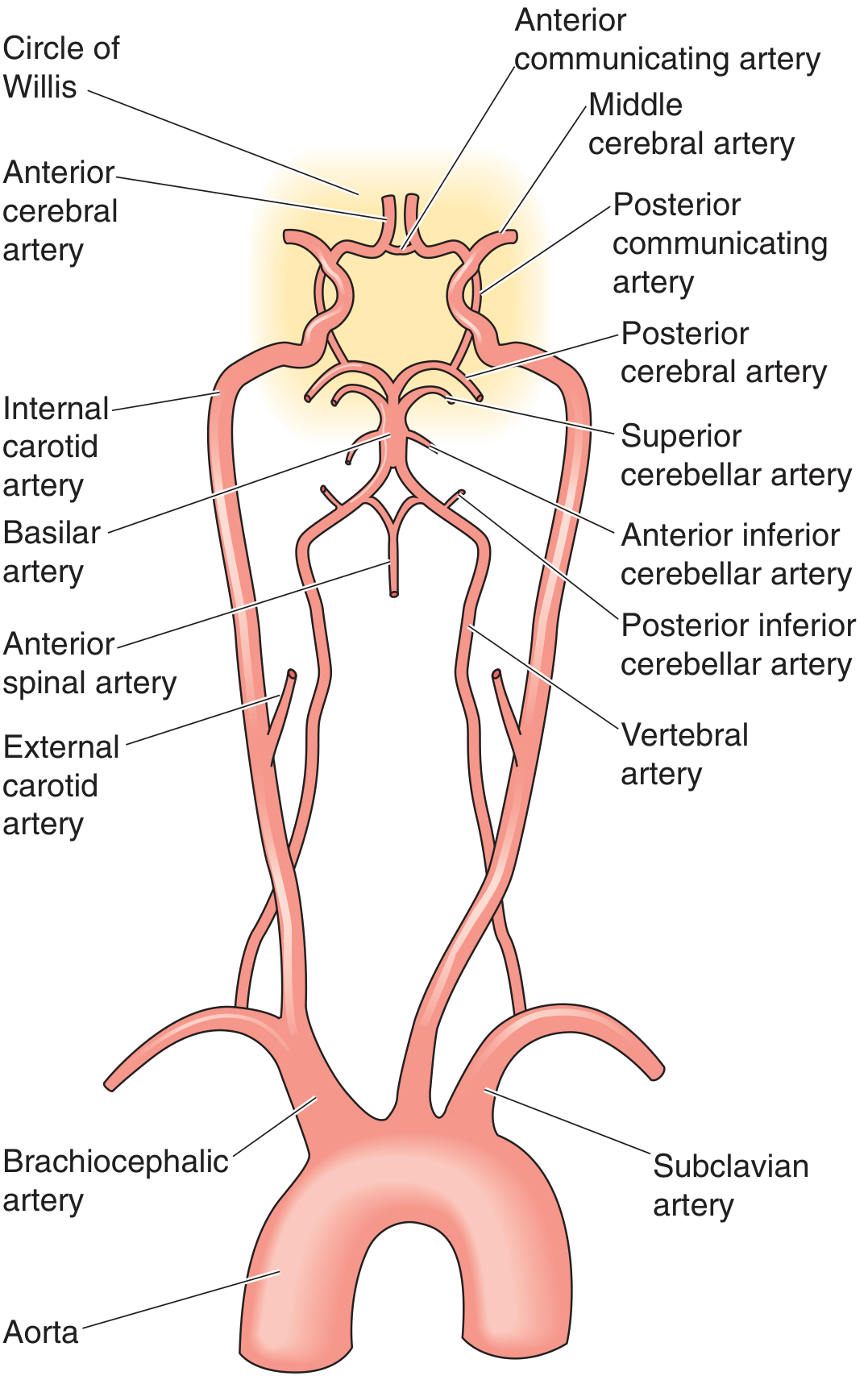
Circle of Willis
The Circle of Willis is the anastomotic ring at the base of the brain where the anterior (carotid) and posterior (vertebrobasilar) circulations meet. It provides collateral flow capacity - though a complete, full-caliber ring is present in only about 34% of individuals.
Overview: Anterior vs Posterior Circulation
| Circulation | Origin | Main vessels |
|---|---|---|
| Anterior | Internal carotid arteries (ICA) | ACA, MCA |
| Posterior | Vertebral arteries (from subclavian) → basilar artery | PCA, SCA, AICA, PICA |
The two vertebral arteries ascend through the foramina transversaria of C1-C6, enter the foramen magnum, then join at the pontomedullary junction to form the basilar artery.
The Circle of Willis - Structure
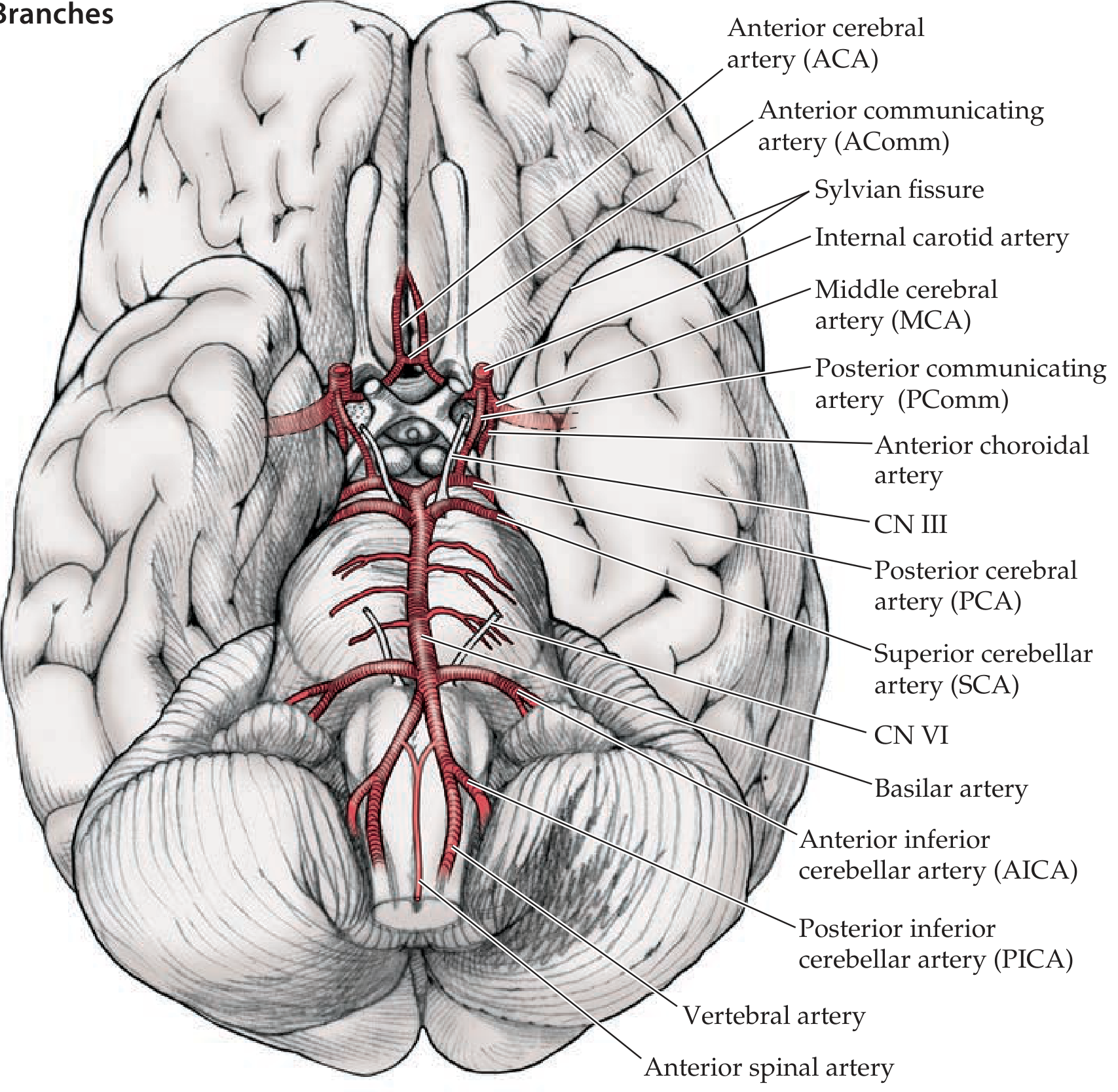
Components of the Circle
The circle is formed by 6 vessels connected by 2 communicating arteries:
| Vessel | Part of circle | Origin |
|---|---|---|
| Anterior communicating artery (AComm) | Anterior bridge | Connects the two ACAs |
| Anterior cerebral arteries x2 (ACA) | Anterior arms | Terminal branch of ICA |
| Internal carotid arteries x2 (ICA) | Lateral pillars | Carotid bifurcation |
| Posterior communicating arteries x2 (PComm) | Lateral bridges | ICA → PCA; joins anterior to posterior |
| Posterior cerebral arteries x2 (PCA) | Posterior arms | Top of basilar artery |
The Middle cerebral artery (MCA) is the other major terminal branch of the ICA but is not strictly part of the circle itself - it exits laterally into the Sylvian fissure.
The Three Main Cerebral Arteries and Their Territories
| Artery | Territory | Key structures supplied | Stroke deficit |
|---|---|---|---|
| ACA (Anterior cerebral) | Medial surface; anterior 2/3 | Medial sensorimotor cortex (leg area), frontal lobe medial, anterior corpus callosum | Contralateral leg > arm weakness/sensory loss; incontinence; abulia |
| MCA (Middle cerebral) | Lateral convexity | Lateral sensorimotor cortex (face/arm), Broca's area (dominant), Wernicke's area (dominant), deep via lenticulostriate to internal capsule + basal ganglia | Contralateral face + arm > leg weakness; aphasia (dominant) or neglect (non-dominant) |
| PCA (Posterior cerebral) | Occipital lobe; inferior temporal; thalamus, midbrain | Visual cortex, thalamus, posterior limb of internal capsule, hippocampus | Contralateral homonymous hemianopia; thalamic pain; memory loss; alexia without agraphia |
Deep Penetrating Branches (Clinically Important)
| Branch | Origin | Supplies | Clinical significance |
|---|---|---|---|
| Lenticulostriate arteries | Proximal MCA (M1) | Putamen, caudate, internal capsule (posterior limb) | "Charcot's artery of cerebral hemorrhage" - common site of hypertensive bleed; also causes lacunar infarcts |
| Anterior choroidal artery | ICA (after PComm) | Posterior limb internal capsule, optic tract, hippocampus, choroid plexus | Occlusion: contralateral hemiplegia + hemianesthesia + hemianopia ("three H's") |
| Perforating branches of basilar | Basilar artery | Pons, midbrain | Lacunar infarcts in pons; locked-in syndrome (basilar occlusion) |
Cerebellar Arteries
Three paired cerebellar arteries arise from the posterior circulation:
| Artery | Origin | Territory | Key syndrome on occlusion |
|---|---|---|---|
| PICA (Posterior inferior cerebellar) | Vertebral artery | Lateral medulla + inferior cerebellum | Wallenberg (lateral medullary) syndrome - ipsilateral face, contralateral body pain/temp loss; dysphagia, Horner's, ataxia |
| AICA (Anterior inferior cerebellar) | Basilar artery | Lateral pons + anterior inferior cerebellum | Ipsilateral CN VII/VIII involvement + cerebellar signs |
| SCA (Superior cerebellar) | Basilar artery (just before bifurcation) | Superior cerebellum | Cerebellar ataxia; ipsilateral Horner's |
ICA Segments - Mnemonic: OPAAM
The main branches of the supraclinoid ICA (after it pierces the dura):
- O - Ophthalmic artery (retinal supply - "window to brain vasculature")
- P - Posterior communicating artery (PComm)
- A - Anterior choroidal artery
- A - Anterior cerebral artery (ACA)
- M - Middle cerebral artery (MCA)
Clinical Pearls
- PComm aneurysm compresses CN III as it runs alongside it → CN III palsy (dilated pupil, ptosis, "down and out" eye) - a neurosurgical emergency
- The AComm is the most common site for berry aneurysm rupture (subarachnoid hemorrhage)
- MCA is the most commonly occluded artery in stroke - lenticulostriate branches are "end arteries" with no collateral supply
- Collateral flow via the Circle of Willis allows ICA stenosis/occlusion to sometimes be tolerated if other vessels are patent
- Posterior circulation strokes often cause crossed deficits (ipsilateral cranial nerve + contralateral limb) and vertigo/ataxia - the vertebrobasilar territory is not just the "back of the brain"
Sources: Neuroanatomy through Clinical Cases, 3rd Ed.; Medical Physiology (Boron & Boulpaep); Neuroscience: Exploring the Brain, 5th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.