Teel me about menstual cycle
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive, authoritative content from the textbooks and the menstrual cycle diagram. Let me compile the full answer.
The Menstrual Cycle
The menstrual cycle is a precisely coordinated series of hormonal and structural events that prepares the female reproductive tract for potential pregnancy each month. It involves the hypothalamus, pituitary gland, ovaries, and uterus working in sequence.
Overview
A "typical" cycle is 28 days long, though 21-35 days is considered normal. Day 1 is counted from the first day of menstrual bleeding. The cycle has two main phases divided by ovulation on approximately day 14:
- Follicular phase (days 1-14) - also called the proliferative phase
- Luteal phase (days 14-28) - also called the secretory phase
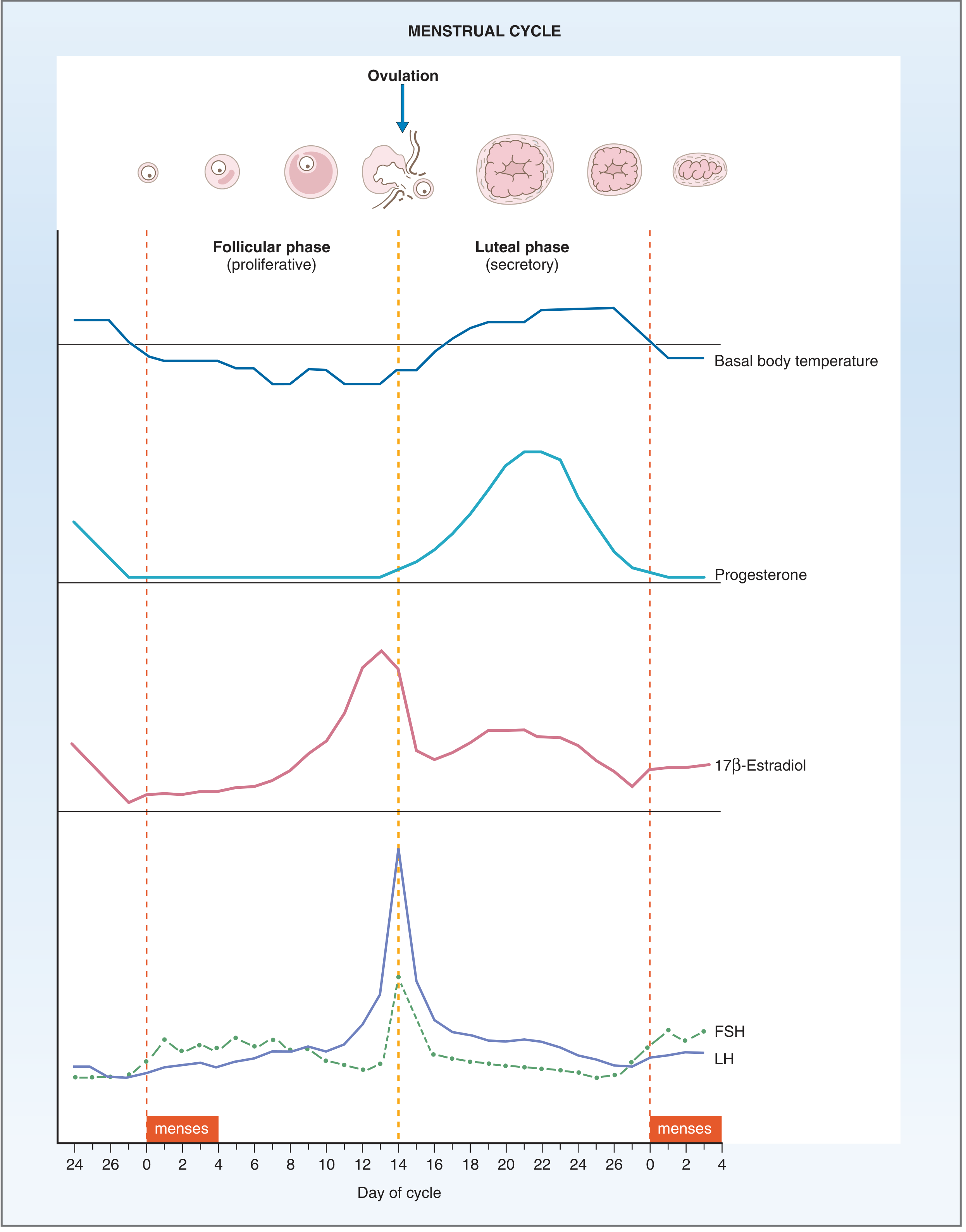
Fig. 10.10 - Events of the menstrual cycle showing FSH, LH, 17β-Estradiol, progesterone, and basal body temperature changes. Ovulation occurs at day 14. - Costanzo Physiology 7th Edition
The Hormonal Control System
The cycle is regulated through a 3-tier axis:
1. Hypothalamus secretes GnRH (gonadotropin-releasing hormone) in pulses. The pulse frequency determines how much FSH vs. LH is released from the pituitary. The hypothalamus is influenced by feedback from ovarian hormones via long, short, and ultrashort feedback loops.
2. Anterior Pituitary produces:
- FSH (follicle-stimulating hormone) - drives follicle development
- LH (luteinizing hormone) - triggers ovulation and corpus luteum formation
FSH and LH are glycoproteins with identical alpha subunits but different beta subunits that confer receptor specificity.
3. Ovaries respond to FSH and LH to produce estrogen and progesterone, which in turn feed back on the hypothalamus and pituitary.
-
- Berek & Novak's Gynecology, p. 265-275
Phase 1: Follicular (Proliferative) Phase - Days 1 to 14
Ovarian Events
At the start of each cycle, rising FSH recruits a cohort of primordial follicles. One dominant follicle is selected, grows, and begins secreting increasing amounts of estradiol (17β-estradiol). The granulosa cells of the follicle aromatize androgens (produced by theca cells under LH stimulation) into estradiol - this is the "two-cell, two-gonadotropin" model.
Endometrial Events
Rising estradiol causes:
- Growth and proliferation of the endometrial lining
- Growth of uterine glands and stroma
- Elongation of spiral arteries
- Cervical mucus becomes copious, watery, and elastic - producing a "ferning" pattern on a glass slide. This creates channels through which sperm can travel.
The LH Surge
As estradiol rises to a critical threshold late in the follicular phase, it switches from negative feedback to positive feedback on the pituitary, triggering a massive surge in LH (and smaller FSH surge). This LH surge is the signal for ovulation.
-
- Costanzo Physiology 7th Edition, p. 478
Ovulation - Day 14
The LH surge triggers the dominant follicle to rupture and release its oocyte into the fallopian tube. The oocyte (which was arrested in meiosis I) resumes meiosis upon the LH surge. The empty follicle then transforms into the corpus luteum.
Phase 2: Luteal (Secretory) Phase - Days 14 to 28
Ovarian Events
The corpus luteum forms from the ruptured follicle and begins secreting large amounts of progesterone as well as some estradiol. These high levels suppress FSH and LH via negative feedback, preventing new follicle recruitment.
Endometrial Events
Under progesterone's influence:
- Endometrial proliferation slows
- Uterine glands become tortuous and glycogen-filled, increasing secretions
- Stroma becomes edematous
- Spiral arteries elongate and become coiled
- Cervical mucus becomes thick, scant, and non-elastic - no longer penetrable by sperm
The endometrium is now in its optimal state for embryo implantation.
Basal body temperature rises by ~0.5°C in the luteal phase, because progesterone raises the hypothalamic temperature set point. This temperature shift can be used to detect ovulation.
-
- Costanzo Physiology 7th Edition, p. 479-480
Phase 3: Menses - Days 1 to 4-5
If fertilization does not occur, the corpus luteum regresses (luteolysis) around day 26-28. Progesterone and estradiol levels drop abruptly. Without hormonal support:
-
The spiral arteries constrict and then dilate, causing ischemia and necrosis of the endometrium
-
The endometrial lining and blood are shed as menstrual flow
-
Menses typically lasts 4-5 days
-
During menses, FSH begins to rise again as the next cycle's follicles are recruited
-
- Berek & Novak's Gynecology, p. 264
What Happens if Pregnancy Occurs?
If fertilization occurs, the developing embryo (blastocyst) secretes hCG (human chorionic gonadotropin), which acts like LH to rescue the corpus luteum. The corpus luteum then continues producing progesterone to maintain the endometrium until the placenta takes over (around week 10-12).
Summary Table
| Feature | Follicular Phase (Days 1-14) | Luteal Phase (Days 14-28) |
|---|---|---|
| Dominant hormone | Estrogen | Progesterone |
| Endometrium | Proliferating, thickening | Secretory, glands tortuous |
| Cervical mucus | Watery, elastic, "ferning" | Thick, scant, no ferning |
| Basal body temp | Lower | Higher (+0.5°C) |
| Ovarian structure | Growing follicle | Corpus luteum |
| FSH/LH | Gradually rising | Low (suppressed) |
Clinical Notes
- Amenorrhea (absent periods): can result from hyperprolactinemia, hypothalamic dysfunction, thyroid disease, or ovarian failure
- Cycle length variation is mainly due to differences in the follicular phase - the luteal phase is consistently about 14 days
- Progesterone measurement on day 21 is used clinically to confirm ovulation (levels >3 ng/mL suggest ovulation has occurred)
- Elevated prolactin inhibits GnRH pulsatility and can disrupt the entire cycle, causing amenorrhea and galactorrhea
Sources: Berek & Novak's Gynecology | Costanzo Physiology 7th Edition | The Developing Human: Clinically Oriented Embryology
What are common menstrual cycle disorders (PCOS, endometriosis, irregular periods)?
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"polycystic ovary syndrome"[MeSH Terms] AND management
Finding Sources
Finding Sources
Searching PubMed
"endometriosis"[MeSH Terms] AND diagnosis AND treatment
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive guide to the most common menstrual cycle disorders:
Common Menstrual Cycle Disorders
1. Polycystic Ovary Syndrome (PCOS)
What it is
PCOS is the most common endocrine abnormality in women of reproductive age, affecting 6-12% of this population. It is a heterogeneous disorder with considerable clinical and biochemical variability. - Goldman-Cecil Medicine, p. 2560
Diagnosis - Rotterdam Criteria (2003)
Two out of three of the following are required (after excluding other causes):
| Criterion | Details |
|---|---|
| 1. Oligo-ovulation or anovulation | Irregular or absent periods |
| 2. Hyperandrogenism | Clinical (hirsutism, acne, male-pattern hair loss) or biochemical (elevated testosterone) |
| 3. Polycystic ovaries on ultrasound | ≥12 follicles per ovary, each 2-9 mm in diameter |
This gives rise to four phenotypes, ranging from full triad to isolated features. - Berek & Novak's Gynecology, p. 1920
Pathophysiology
The core defect involves:
- Insulin resistance and compensatory hyperinsulinemia - present across all racial/ethnic groups
- Insulin amplifies LH-driven androgen production by ovarian theca cells
- Elevated androgens disrupt normal follicular development, causing anovulation
- The hypothalamic-pituitary unit is structurally intact but functionally deranged - often showing an elevated LH:FSH ratio
- Genetic factors: alterations in CYP17 (androgen synthesis) and CYP19 (aromatase) genes have been implicated
Clinical Features
- Menstrual irregularity: ranging from oligomenorrhea to complete amenorrhea - the most common presenting complaint
- Hirsutism: occurs in ~70% of US patients with PCOS
- Acne and male-pattern alopecia
- Obesity: worsens insulin resistance and hyperandrogenism in a vicious cycle
- Acanthosis nigricans: a skin sign of insulin resistance (velvety dark patches at skin folds)
- PCOS typically begins at puberty and may worsen with weight gain
Long-Term Risks
- >50% of affected women develop type 2 diabetes by age 40
- Cardiovascular disease risk
- Endometrial hyperplasia/cancer (from chronic anovulation with unopposed estrogen)
- Infertility - Goldman-Cecil Medicine, p. 2560
Treatment
- Lifestyle modification - weight loss of even 5-10% restores ovulation in many women. A 2025 systematic review (PMID 39861440) confirms lifestyle interventions as first-line.
- Combined oral contraceptive pill (OCP) - suppresses androgen production and regulates cycles
- Metformin - improves insulin sensitivity, can restore ovulation
- Inositol - a 2024 meta-analysis (PMID 38163998) for the updated PCOS guidelines found inositol supplementation improves metabolic and hormonal parameters
- Clomiphene or letrozole - for ovulation induction when fertility is desired
- Anti-androgens (spironolactone) for hirsutism
2. Endometriosis
What it is
Endometriosis is defined by the presence of endometrial glands and stroma outside the uterus. It occurs in up to 10% of women of reproductive age and in nearly half of women with infertility. - Robbins & Kumar Basic Pathology, p. 689
Three Types
- Superficial peritoneal endometriosis - implants on the pelvic peritoneum
- Ovarian endometriosis - "chocolate cysts" (endometriomas)
- Deep infiltrating endometriosis - penetrates >5 mm below the peritoneal surface; highest risk of malignant transformation
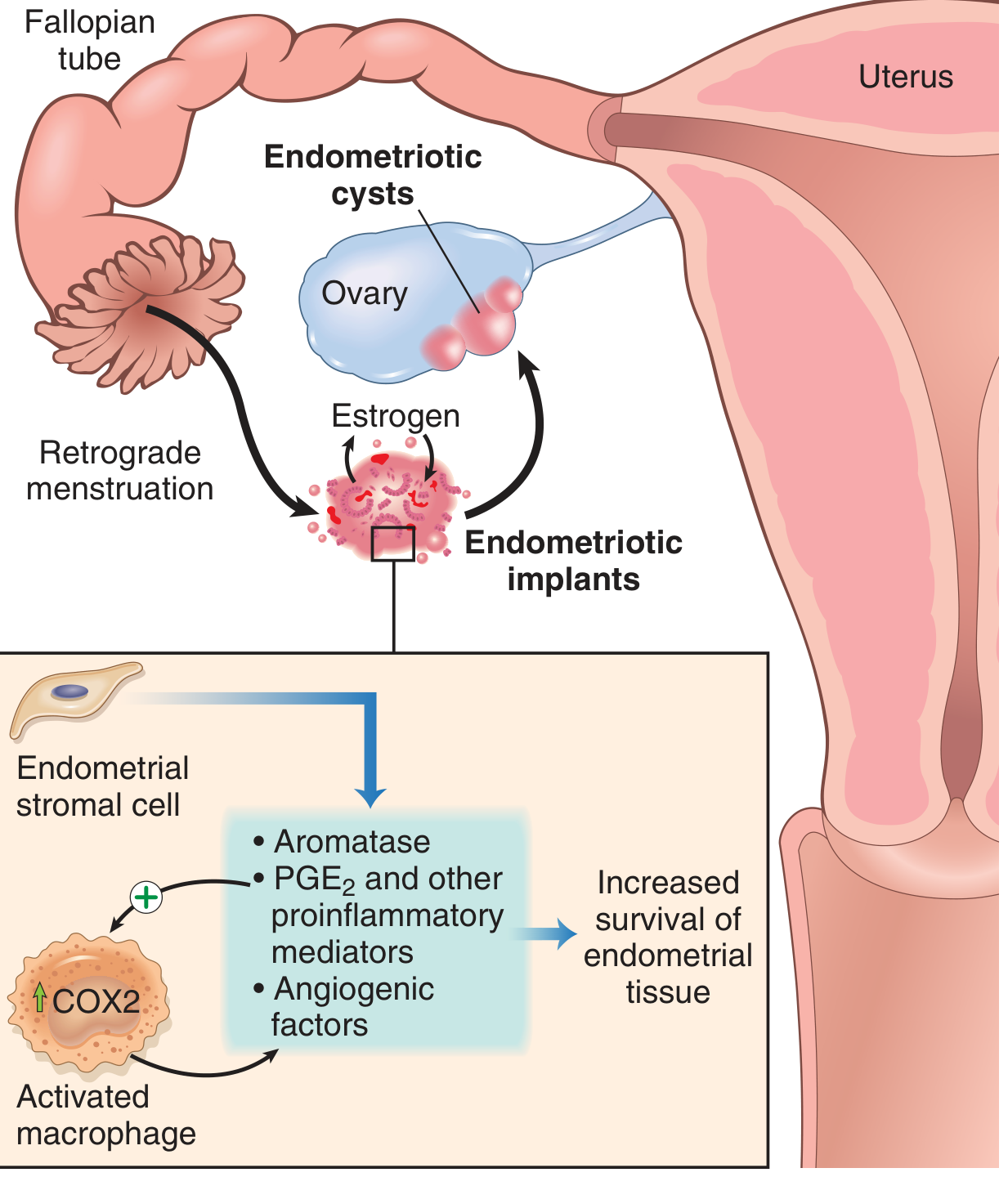
Fig. 17.9 - Pathogenesis of endometriosis. Retrograde menstruation seeds implants which produce aromatase, PGE2, and angiogenic factors, creating a self-sustaining inflammatory cycle. - Robbins & Kumar Basic Pathology
Pathogenesis - Leading Theories
- Retrograde menstruation theory (Sampson's theory): Most widely accepted. Endometrial tissue flows backwards through the fallopian tubes during menstruation and implants on pelvic structures
- Benign metastasis theory: Spread via blood/lymphatics to distant sites (lung, brain, bone)
- Coelomic metaplasia theory: Peritoneal cells undergo metaplastic transformation into endometrial-type tissue
- Stem/progenitor cell theory: Bone marrow-derived cells differentiate into ectopic endometrium
The implants are not just misplaced tissue - they express increased aromatase (making local estrogen), elevated COX-2, PGE2, VEGF, and matrix metalloproteinases. This creates an estrogen-driven, proinflammatory, self-sustaining environment. - Robbins & Kumar, p. 689
Clinical Features
- Severe dysmenorrhea (cyclical pelvic pain around menses)
- Dyspareunia (pain with intercourse)
- Chronic pelvic pain
- Infertility - the presenting issue in 30-40% of patients
- Menstrual irregularities - heavy or irregular bleeding
- Widespread disease causes adhesions that can distort pelvic anatomy, kink the fallopian tubes, and obliterate the pouch of Douglas
Diagnosis
Definitive diagnosis requires laparoscopy with histological confirmation. A 2025 systematic review (PMID 39373298) highlighted that diagnostic delay remains a significant problem globally, averaging 4-10 years in many regions.
Treatment
- NSAIDs and COX-2 inhibitors - first-line for pain
- Combined OCP or continuous progestin (oral, implant, or levonorgestrel IUD) - suppresses cyclical stimulation
- GnRH agonists with add-back therapy - for refractory cases
- Aromatase inhibitors - block local estrogen production in implants
- Laparoscopic surgical excision - for endometriomas or anatomical distortion
- Harrison's Principles of Internal Medicine 22e, p. [endometriosis section]
3. Irregular Periods and Related Disorders
Terminology
| Term | Definition |
|---|---|
| Amenorrhea | Absence of periods (primary: never started by age 15; secondary: stopped for ≥3 months) |
| Oligomenorrhea | Infrequent periods (cycle >35 days) |
| Menorrhagia | Heavy menstrual bleeding (>80 mL/cycle or lasting >7 days) |
| Metrorrhagia | Irregular, inter-menstrual bleeding |
| Dysmenorrhea | Painful periods |
| Polymenorrhea | Too-frequent periods (cycle <21 days) |
Dysmenorrhea
Primary dysmenorrhea has no structural cause - it results from elevated prostaglandins (PGE2, PGF2α) causing uterine contractions and ischemia. It typically starts within 1-2 years of menarche and often improves with age or after childbirth.
Secondary dysmenorrhea has an underlying structural cause - endometriosis, fibroids, adenomyosis, or pelvic inflammatory disease.
Treatment (from Harrison's 22e):
- NSAIDs (ibuprofen, naproxen, mefenamic acid) - provide >80% sustained response; most effective when started before the onset of menses and continued for 2-3 days
- Combined or progestin-only hormonal contraceptives
- Heat, exercise, omega-3 fatty acids, and vitamin B1 have supporting evidence
Abnormal Uterine Bleeding (AUB)
The most common cause is anovulatory dysfunctional bleeding, which can arise from:
- Hormonal imbalances - most common at menarche and perimenopause when the HPO axis is unstable
- PCOS (see above)
- Hyperprolactinemia - elevated prolactin suppresses GnRH pulsatility
- Thyroid disorders - both hyper- and hypothyroidism disrupt the cycle
- Obesity or malnutrition - alter peripheral estrogen metabolism
- Luteal phase defect - insufficient progesterone production by the corpus luteum
- Robbins & Kumar Basic Pathology, p. 689
Amenorrhea
Broadly classified as:
Primary amenorrhea (no menses by age 15 with normal secondary sexual characteristics, or by 13 without them):
- Turner syndrome (45,X) - most common cause of primary ovarian failure
- Müllerian agenesis (absent uterus)
- Androgen insensitivity syndrome
Secondary amenorrhea (cessation of periods for ≥3 months):
- Pregnancy - always exclude first
- Hypothalamic amenorrhea - due to excessive exercise, low body weight/eating disorders, or psychological stress (suppresses GnRH pulsatility)
- Hyperprolactinemia - pituitary adenoma is a common cause
- PCOS (most common cause of secondary amenorrhea in reproductive-age women)
- Premature ovarian insufficiency - loss of ovarian function before age 40
- Berek & Novak's Gynecology, Ch. 34
Premenstrual Syndrome (PMS) and PMDD
PMS involves physical and mood symptoms (bloating, breast tenderness, irritability, anxiety) in the luteal phase that resolve with menses.
PMDD (Premenstrual Dysphoric Disorder) is the severe form, characterized by disabling mood disturbance. It is driven by abnormal CNS sensitivity to normal cyclical progesterone/allopregnanolone fluctuations.
Treatment: SSRIs (most effective), combined OCP, calcium supplementation (1200 mg/day has strong evidence), and cognitive behavioral therapy.
Summary Comparison
| Disorder | Key Feature | Core Mechanism | Main Treatments |
|---|---|---|---|
| PCOS | Irregular periods + hyperandrogenism | Insulin resistance, anovulation | Lifestyle, OCP, metformin |
| Endometriosis | Cyclical pelvic pain, infertility | Ectopic endometrial implants, estrogen-driven inflammation | NSAIDs, hormonal suppression, surgery |
| Primary dysmenorrhea | Painful periods, no structural cause | Prostaglandin excess | NSAIDs, OCP |
| Anovulatory AUB | Irregular/heavy bleeding | HPO axis instability | Hormonal regulation |
| Hypothalamic amenorrhea | No periods, low BMI or stress | Suppressed GnRH pulsatility | Weight restoration, stress reduction |
| PMDD | Severe luteal phase mood symptoms | CNS sensitivity to progesterone metabolites | SSRIs, OCP, CBT |
Sources: Goldman-Cecil Medicine | Robbins & Kumar Basic Pathology | Berek & Novak's Gynecology | Harrison's Principles of Internal Medicine 22e | Costanzo Physiology 7th Edition
This is a shared conversation. Sign in to Orris to start your own chat.