10 changes of ecg
Reading File
Finding Sources
Finding Sources
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Searching Images
ECG changes myocardial infarction STEMI T wave Q wave evolution
Now I have comprehensive material. Let me compile the full answer.
10 ECG Changes in Myocardial Infarction / Ischemia
ECG findings in ischemia and infarction span from the earliest minutes of coronary occlusion through the chronic healed phase. Here are the key 10 changes:
1. Hyperacute T Waves (earliest change — minutes)
Tall, broad, peaked T waves appear in the leads overlying the ischemic territory. This is often the very first ECG sign of STEMI, preceding ST elevation. The T wave is abnormally large and "tent-like."
"Note the broad, tall T waves in leads V3 and V4... These are the hyperacute T waves of early ST segment elevation myocardial infarction." — Rosen's Emergency Medicine
2. ST-Segment Elevation (minutes to hours — transmural ischemia)
ST elevation ≥1 mm in ≥2 contiguous leads defines STEMI. The morphology is typically flat, horizontal, or convex (tombstone-like) — distinct from the concave elevation of pericarditis or benign early repolarization.
- Transmural ischemia from epicardial coronary occlusion (thrombosis or vasospasm)
- Indicates the "culprit" territory (anterior, inferior, lateral, posterior)
3. Reciprocal ST Depression (simultaneous with ST elevation)
ST depression in leads on the opposite side of the infarcting territory. Examples:
- Inferior STEMI (II, III, aVF elevation) → reciprocal ST depression in aVL
- Anterior STEMI (V1–V4 elevation) → reciprocal depression in inferior leads (II, III, aVF)
- Posterior MI → ST depression in V1–V3 (representing posterior ST elevation "mirrored")
Reciprocal changes increase specificity, and correlate with larger infarct size and worse outcomes. — Rosen's Emergency Medicine
4. ST-Segment Depression (subendocardial ischemia / NSTEMI)
Horizontal or downsloping ST depression indicates subendocardial ischemia. Seen in:
- Unstable angina and NSTEMI
- Demand ischemia (exercise, tachycardia)
- As a reciprocal change in STEMI
Upsloping depression is less specific for ischemia. — Miller's Anesthesia
5. T-Wave Inversion (hours after onset → subacute phase)
Symmetrical, narrow T-wave inversions in the ischemic leads. The Wellens syndrome is a critical subtype:
- Type I: Deep symmetrical T-wave inversions in anterior precordial leads (V2–V3)
- Type II: Biphasic T waves in anterior leads
- Both indicate critical LAD stenosis with high risk of progressing to anterior STEMI
"The T wave inversions of ACS are classically narrow and symmetrical." — Rosen's Emergency Medicine
6. Q-Wave Formation (hours to days — transmural necrosis)
Pathological Q waves (≥40 ms wide, ≥25% depth of R wave) reflect loss of viable myocardium and depolarisation away from that territory. Development depends on:
- Volume of infarcted tissue (more so than transmurality)
- Reperfusion status — Q waves may be transient if perfusion is restored early
"Most patients initially presenting with ST-segment elevation ultimately evolve Q waves on the ECG." — Harrison's Principles of Internal Medicine
7. Loss of R-Wave Progression / Poor R-Wave Progression
Progressive decrease or absence of R waves across precordial leads V1–V4 in anterior MI. A QS complex (entirely negative deflection, no R wave) indicates full-thickness necrosis.
8. Biphasic T Waves
An intermediate finding between upright T waves and full inversion. Classically seen in Wellens Type II (anterior leads) — a warning sign of impending anterior STEMI due to LAD lesion.
9. PR-Segment Changes (less common in MI; important to distinguish from pericarditis)
In acute pericarditis (a mimic of MI): diffuse PR depression with PR elevation in aVR. In contrast, MI ECG does not show PR changes — this distinction helps differentiate the two.
10. Normalisation / Chronic ECG Pattern (weeks to months — healed MI)
After the acute phase, the ECG may evolve to:
- Persistent Q waves (permanent marker of prior infarction)
- T-wave normalisation (may re-invert or flatten)
- ST elevation persisting >2 weeks suggests left ventricular aneurysm
- Return toward baseline in successfully reperfused patients (Q waves may disappear)
Summary Table: Temporal Sequence of ECG Changes in STEMI
| Time | ECG Finding |
|---|---|
| Minutes (earliest) | Hyperacute tall T waves |
| Minutes–hours | ST elevation (convex/flat) |
| Simultaneous | Reciprocal ST depression |
| Hours | T-wave inversion begins |
| Hours–days | Pathological Q waves |
| Hours–days | Loss of R-wave progression / QS complex |
| Days–weeks | Deep symmetrical T-wave inversions (subacute) |
| Weeks–months | T-wave normalisation |
| >2 weeks | Persistent ST elevation → LV aneurysm |
| Chronic | Fixed Q waves (permanent scar) |
ECG Territory Localisation
| Territory | Elevated Leads | Artery |
|---|---|---|
| Anterior | V1–V4 | LAD |
| Inferior | II, III, aVF | RCA or LCx |
| Lateral | I, aVL, V5–V6 | LCx |
| Posterior | ST ↓ V1–V3 (mirror) | RCA/LCx |
| RV | V4R (right-sided leads) | Proximal RCA |
Key ECG Images
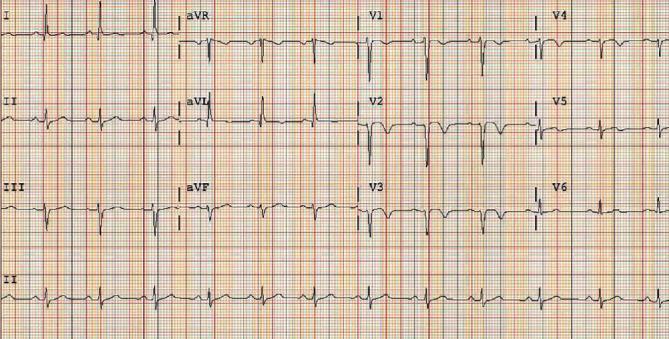
Serial ECG showing anterior STEMI evolution: QS complexes (V2–V5) with deep symmetrical T-wave inversions — classic subacute phase post-LAD occlusion
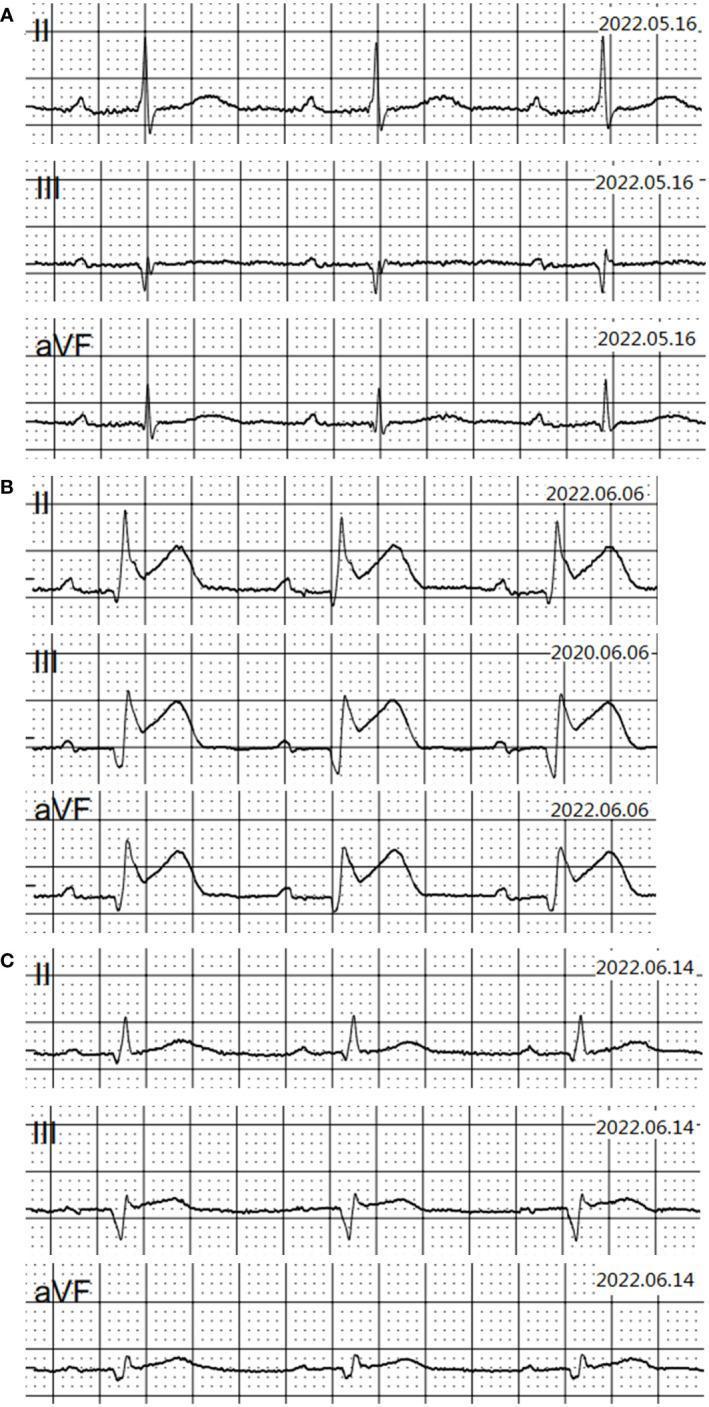
Serial inferior leads (II, III, aVF) showing baseline → acute STEMI (ST elevation + Q waves) → subacute/chronic phase (T-wave flattening)
Sources: Rosen's Emergency Medicine, 10e | Harrison's Principles of Internal Medicine, 22e | Fuster and Hurst's The Heart, 15e | Miller's Anesthesia, 10e
This is a shared conversation. Sign in to Orris to start your own chat.