Explain epistaxis
Reading File
Finding Sources
Searching PubMed
epistaxis management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive explanation. Here is the full answer:
Epistaxis (Nosebleed)
Epistaxis — bleeding from the nasal cavity — is one of the most common otolaryngologic presentations. While distressing, it is rarely life-threatening.
Anatomy & Vascular Supply
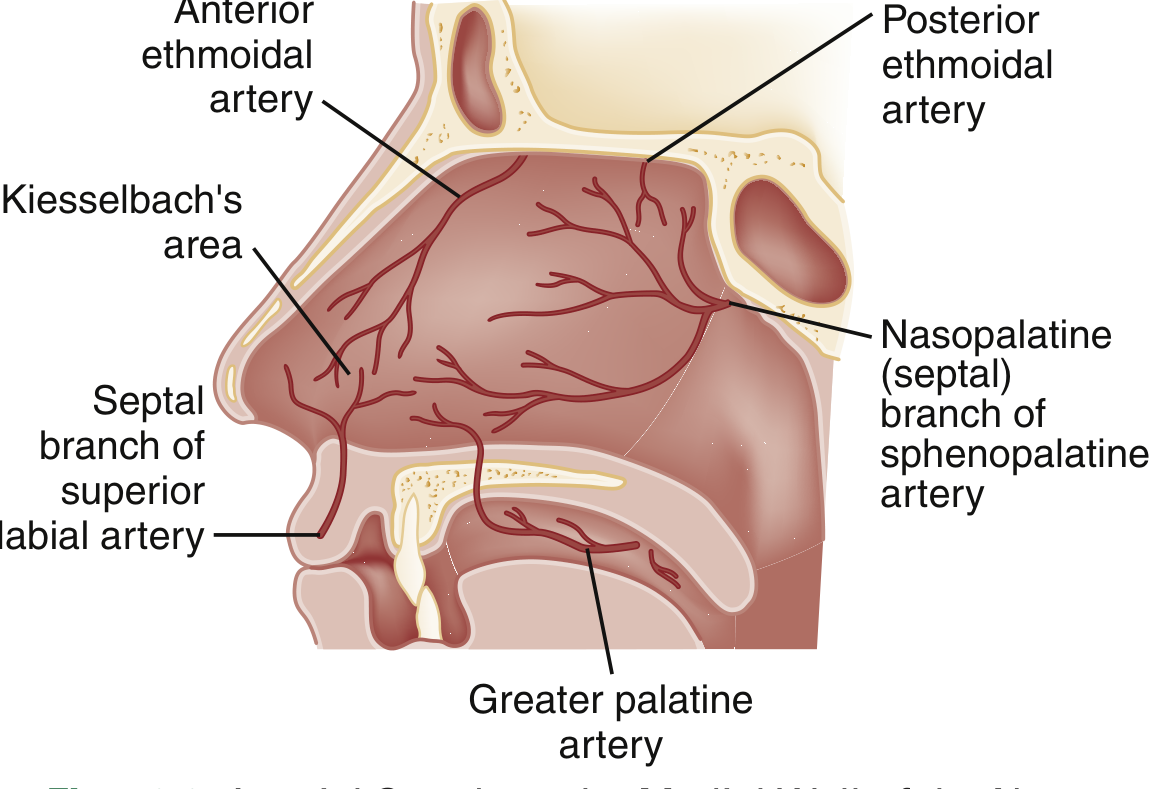
Three arterial systems supply the nasal mucosa:
| Artery | Origin | Area Supplied |
|---|---|---|
| Sphenopalatine artery | External carotid → maxillary | Turbinates, posterior/inferior septum |
| Anterior & posterior ethmoidal arteries | Internal carotid → ophthalmic | Superior mucosa, medially and laterally |
| Superior labial artery | External carotid → facial | Anterior mucosal septum |
Kiesselbach's plexus (also called Little's area) is the anastomotic confluence of all three systems on the anteroinferior nasal septum — the origin of ~90% of all nosebleeds.
Classification
| Type | Frequency | Source | Features |
|---|---|---|---|
| Anterior | ~90% | Kiesselbach's plexus | Unilateral, self-limited, visible |
| Posterior | ~10% | Sphenopalatine artery | Bilateral, profuse, older adults, harder to manage |
Posterior bleeding originates deep in the nasal cavity, is more severe, tends to occur in older patients with multiple comorbidities, and carries risk of airway compromise and aspiration.
Epidemiology
- Bimodal age distribution: peaks in children and the elderly
- Higher incidence in winter months and cold/dry climates — dry heated air desiccates nasal mucosa and cold affects coagulation
- In children, most common between ages 2–10
Causes
Local (nasal/facial):
- Nose picking (most common in children)
- Upper respiratory tract infections / rhinitis
- Low humidity / desiccation (rhinitis sicca)
- Allergic rhinitis
- Nasal foreign bodies
- Nasal polyps, septal deviation
- Environmental irritants (cocaine, chronic nasal vasoconstrictors)
- Barotrauma
- Trauma / surgery
- Neoplasms (e.g., juvenile nasopharyngeal angiofibroma in adolescent males — suspect when there is profuse unilateral bleeding with nasal obstruction)
Systemic:
- Anticoagulant or antiplatelet therapy
- Coagulopathies (von Willebrand disease type 1 is the most commonly identified — found in ~⅓ of children with recurrent epistaxis)
- Thrombocytopenia (leukemia, aplastic anemia, chemotherapy)
- Hepatic disease / vitamin K deficiency
- Hereditary hemorrhagic telangiectasia (Osler-Weber-Rendu disease) — a congenital vascular malformation causing recurrent, multifocal bleeding
- Hypertension: no proven causal relationship, but elevated BP at presentation is associated with persistent bleeding
Clinical Evaluation
Initial priorities
- Airway — assess patency, especially in posterior bleeds
- Hemodynamics — tissue perfusion, signs of significant blood loss
- History — timing, frequency, severity; trauma; medications; family history of bleeding disorders
Physical examination
- Instruct patient to blow the nose to clear clots
- Apply bilateral pressure on the cartilaginous part of the nose for 10–15 minutes (a nose clip is superior to manual pressure alone)
- Administer 0.05% oxymetazoline (2 sprays) before applying pressure to optimize hemostasis and aid examination
- Tilt head slightly forward (not back) to avoid swallowing blood
- Examine with nasal speculum opened vertically, floor of nose parallel to the room floor
Diagnostics
Not routinely required. Reserve labs for:
- Patients on anticoagulants (INR, PT, aPTT, platelets)
- Severe or prolonged bleeding (CBC)
- Underlying liver disease or hematologic malignancy
Management (Stepwise)
Step 1 — Direct pressure + vasoconstriction
- Pinch the cartilaginous nose for 10–15 min
- Topical oxymetazoline or phenylephrine
- Topical anesthetic (2% lidocaine) to facilitate examination
Step 2 — Identify the bleeding site + cautery
- Silver nitrate chemical cautery — most effective when the site is identified
- Apply from periphery → center, superior → inferior (to avoid blood)
- Contact ≤15 seconds; never cauterize both sides of the septum simultaneously (risk of necrosis)
Step 3 — Topical hemostatics
If cautery fails:
- Absorbable gelatin sponge (Gelfoam)
- Oxidized cellulose (Surgicel)
- Topical tranexamic acid (500 mg IV solution on pledget or atomized): moderate-quality evidence supports reduced bleeding at 10 min and re-bleeding at 7–10 days; superior to anterior nasal packing in antiplatelet users
Step 4 — Anterior nasal packing
For persistent anterior epistaxis:
- Merocel (polyvinyl acetal nasal tampon) or Rapid Rhino (procoagulant-coated inflatable balloon) inserted along the floor of the nose
- If uncontrolled despite an adequately placed anterior pack → insert a second pack in the opposite naris
- Routine prophylactic antibiotics are not recommended
Step 5 — Posterior packing
When bleeding persists despite anterior packing, suspect posterior source:
- Double balloon catheter (e.g., Epistat): posterior balloon inflated first, device seated by pulling anteriorly, then anterior balloon inflated
- Foley catheter (if commercial device unavailable): 5–7 mL water in balloon, seated in nasopharynx; caution for pressure necrosis
- Requires inpatient monitoring (risk of airway compromise, hypoxia, cardiac events — especially in elderly)
Step 6 — Refractory / definitive
- Endovascular embolization — >80–91% success rate; preferred in coagulopathic patients and those on anticoagulants; requires bilateral selective internal + external carotid angiography; targets sphenopalatine, facial, and ascending pharyngeal arteries
- Surgical ligation — historically the gold standard for intractable bleeds
Special Situations
| Scenario | Consideration |
|---|---|
| Anticoagulated patient | Anticoagulant reversal rarely needed unless markedly supratherapeutic or life-threatening; topical thrombin/cellulose/gelatin compounds work even in fully anticoagulated patients |
| Child < 2 years | Consider non-accidental trauma and bleeding disorders |
| Recurrent childhood epistaxis | Refer to hematology — ~⅓ have a coagulopathy (most often vWD type 1) |
| Adolescent male, unilateral profuse bleeding | Suspect juvenile nasopharyngeal angiofibroma; CT scan warranted |
| HHT / Osler-Weber-Rendu | Requires specialized multidisciplinary approach; embolization often needed |
Disposition
- Anterior epistaxis controlled in ED → discharge with instructions: avoid nose-picking, apply topical antibiotic ointment nightly to lubricate mucosa
- Anterior pack placed → ENT follow-up in 2–3 days for pack removal; no routine antibiotics
- Posterior pack placed → hospital admission for monitoring
- Refractory → urgent ENT consultation for embolization or surgical planning
Sources: Rosen's Emergency Medicine, 9e • Tintinalli's Emergency Medicine, 9e • Cummings Otolaryngology, 7e • Roberts & Hedges' Clinical Procedures in Emergency Medicine, 7e
This is a shared conversation. Sign in to Orris to start your own chat.