Hydronephrosis
Reading File
Finding Sources
Searching PubMed
hydronephrosis
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the information needed for a comprehensive answer.
Hydronephrosis
Definition
Hydronephrosis is dilation of the renal pelvis and calyces, with accompanying atrophy of the renal parenchyma, caused by obstruction to the outflow of urine. The obstruction may be sudden or insidious, and may occur at any level of the urinary tract - from the urethra to the renal pelvis.
- Robbins & Kumar Basic Pathology, p. 529
Etiology
Causes at Each Level
Congenital
- Atresia of the urethra
- Valve formations in the ureter or urethra
- Aberrant renal artery compressing the ureter
- Abnormal kidney position with torsion or kinking of ureter
- Pelviureteric junction (PUJ) obstruction - most common cause of unilateral hydronephrosis (incidence 1 in 500 live births); caused by an aperistaltic segment at the PUJ due to muscular hypoplasia, high ureteric insertion, or crossing aberrant vessels
Acquired - Obstructive
| Category | Examples |
|---|---|
| Foreign bodies | Calculi (most common), sloughed necrotic papillae |
| Neoplastic | Benign prostatic hyperplasia, carcinoma of prostate, bladder tumors, retroperitoneal lymphoma, carcinoma of cervix/uterus |
| Inflammatory | Prostatitis, ureteritis, urethritis, retroperitoneal fibrosis |
| Neurogenic | Paralysis of bladder from spinal cord damage |
| Physiological | Pregnancy (mild hydronephrosis) |
| Infection | Schistosomiasis |
Unilateral vs. Bilateral: Bilateral hydronephrosis occurs only when obstruction is below the level of the ureters (e.g., bladder outlet, urethra). Obstruction at or above the ureter level produces unilateral disease.
- Robbins & Kumar, p. 530; S Das Manual on Clinical Surgery, p. 582
Pathogenesis
Even with complete obstruction, glomerular filtration persists for some time - the filtrate diffuses back into the renal interstitium and perirenal spaces, ultimately returning to lymphatic and venous systems. Continued filtration progressively dilates the calyces and pelvis.
The high intrapelvic pressure is transmitted back through the collecting ducts, compressing renal vasculature and producing:
-
Arterial insufficiency and venous stasis
-
The papillae suffer the greatest pressure increase
-
Initial functional disturbances are tubular (impaired concentrating ability)
-
Glomerular filtration diminishes only later
-
Obstruction also triggers an interstitial inflammatory reaction, eventually leading to interstitial fibrosis
-
Robbins & Kumar, p. 530
Morphology (Gross & Microscopic)
Gross Pathology:

- Subtotal/intermittent obstruction: kidney massively enlarged (up to 20 cm), consisting almost entirely of the greatly distended pelvicalyceal system
- Renal parenchyma compressed and atrophied, with obliteration of papillae and flattening of pyramids
- Sudden complete obstruction: glomerular filtration compromised early, renal function may cease while dilation is still mild
- Depending on level of obstruction, ureters may also be dilated (hydroureter)
Microscopic Pathology:
-
Early: tubular dilation and atrophy
-
Later: loss of glomeruli, replacement of parenchyma by fibrous tissue
-
Inflammatory reaction minimal in uncomplicated cases
-
Superimposed pyelonephritis is common
-
Robbins & Kumar, p. 530
Clinical Features
Symptoms:
- Dull ache or sense of weight in the loin; may be mild enough to be mistaken for backache
- Rapid development can produce severe colicky pain
- Pain may be referred to the epigastrium (mimicking duodenal ulcer)
- Pain exacerbated by excessive fluid intake, alcohol, or diuretics
- Dietl's crisis: after a few hours of pain, passage of a large volume of urine with visible reduction in swelling
Signs:
- Cystic, large renal swelling - ballottable, bimanually palpable
Unilateral hydronephrosis: may remain silent for long periods unless the contralateral kidney is also dysfunctional.
Bilateral hydronephrosis:
-
Leads to anuria and renal failure
-
Incomplete bilateral obstruction paradoxically causes polyuria (due to tubular concentrating defects) - this can obscure the diagnosis
-
S Das Manual on Clinical Surgery, p. 582; Robbins & Kumar, p. 530
Grading (Ultrasound)
The severity of hydronephrosis on ultrasound is graded qualitatively:
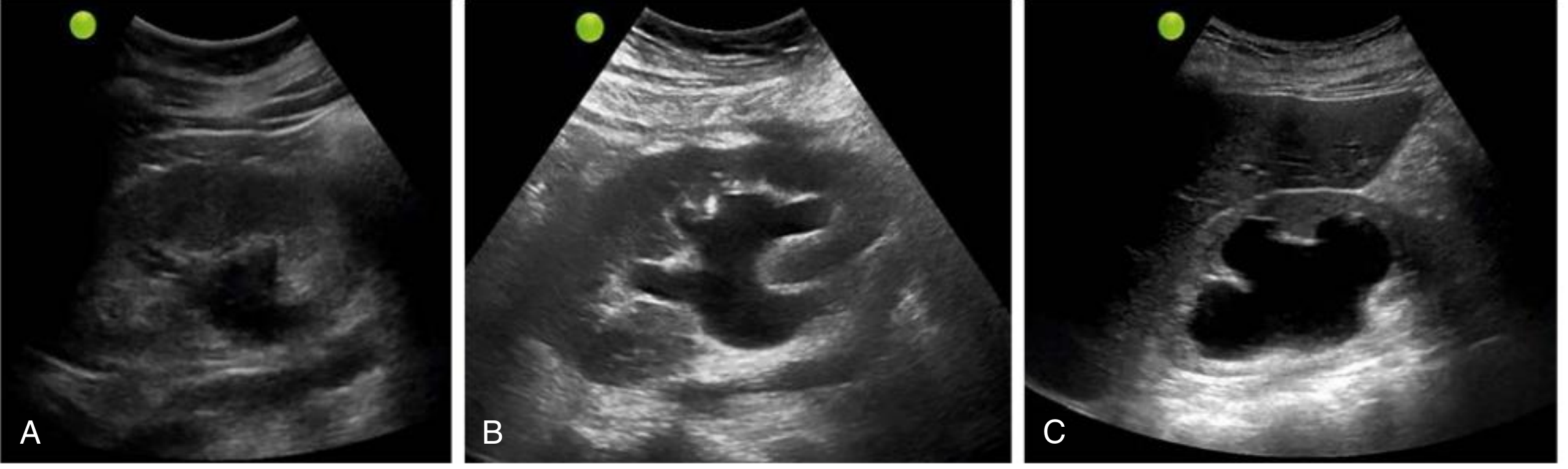
| Grade | US Appearance |
|---|---|
| Mild | Dilation of renal pelvis and calyces; overall parenchymal architecture retained |
| Moderate | Medullary pyramids start to flatten due to back pressure; increasing pelvicalyceal dilation |
| Severe | Renal pelvis and calyces appear ballooned (occupying most of kidney); corticomedullary differentiation lost; parenchyma thin |
If the hydronephrotic area demonstrates internal echoes, consider pyonephrosis (pus in the collecting system) - especially with fever and flank pain.
Pitfalls on ultrasound:
-
False negatives in acute/partial obstruction, volume depletion, retroperitoneal fibrosis
-
Renal vasculature and cysts (especially parapelvic cysts) can mimic hydronephrosis - use color Doppler to confirm flow in vessels; cysts are round and circumscribed vs. the irregular branching pattern of hydronephrosis
-
Comprehensive Clinical Nephrology, 7th ed., p. 81
Investigations
| Test | Purpose |
|---|---|
| Ultrasound (POCUS/US) | First-line; grades severity, identifies cause |
| IVU / Excretory urography | Confirmatory; early films may not show pelvis/calyces - delayed films (6 hrs) improve visualization; retrograde urography if needed |
| CT urogram | Better anatomic detail, identifies stones and tumors |
| MAG3 diuretic renography | Differential renal function, drainage assessment |
| MR urography (MRU) | Alternative to diuretic renogram; superior anatomic resolution, no radiation; gadolinium-based; useful for surgical planning |
| Retrograde pyelography | When other modalities inconclusive |
| VCUG | When vesicoureteric reflux suspected (especially in children) |
- Campbell-Walsh-Wein Urology, p. 537; S Das, p. 582
Management
Principles:
- Treat the underlying cause
- Relieve obstruction promptly to preserve renal function - removal of obstruction usually permits full return of function within a few weeks
- Longstanding obstruction produces irreversible changes
Specific approaches:
- PUJ obstruction: pyeloplasty (Anderson-Hynes dismembered pyeloplasty is the gold standard)
- Ureteric calculi: medical expulsion therapy, ureteroscopy, ESWL, or PCNL depending on size/location
- BPH/bladder outlet obstruction: alpha blockers, 5-alpha reductase inhibitors, TURP
- Malignant obstruction: ureteric stenting or percutaneous nephrostomy as temporizing measures; treat underlying malignancy
- Infected/pyonephrotic kidney: urgent nephrostomy drainage + antibiotics before definitive surgery
- Retroperitoneal fibrosis: corticosteroids, ureteric stenting, ureterolysis
Antenatal Hydronephrosis (ANH)
-
Prevalence 0.6-5.4%; majority are transient and resolve after birth
-
Postnatal ultrasound at least 48 hours after birth
-
Diuretic renography after 4-6 weeks of life
-
ANH classified into low, intermediate, and high risk
-
High-risk: VCUG + antibiotic prophylaxis + functional scan + monthly follow-up
-
Low-risk: 1-3 monthly US follow-up may suffice
-
Bailey and Love's Short Practice of Surgery, 28th ed., p. 3451
Complications
- Chronic renal failure (bilateral obstruction)
- Recurrent UTI / pyelonephritis
- Pyonephrosis
- Hypertension (from renal ischemia)
- Renal calculi (stasis promotes stone formation)
- Rupture of the collecting system (rare)
Sources: Robbins & Kumar Basic Pathology, p. 529-530 | Comprehensive Clinical Nephrology 7th ed., p. 81 | S Das Manual on Clinical Surgery, p. 582 | Bailey and Love's Surgery 28th ed., p. 3451 | Campbell-Walsh-Wein Urology, p. 537
Cause specific treatment
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Excellent - I have rich content from multiple authoritative sources. Here is the comprehensive cause-specific treatment guide:
Hydronephrosis: Cause-Specific Treatment
General Principles Before Specific Therapy
Treatment is dictated by three factors: location of obstruction, underlying cause, and degree of renal impairment.
- Complete bilateral obstruction (or obstruction of a solitary kidney) presenting as AKI is a medical emergency - rapid intervention is required to salvage function
- Short-term obstruction (<1-2 weeks): usually adequate functional return after relief
- Chronic obstruction (>12 weeks): often irreversible and severe kidney damage; recovery may be limited even after relief
- Dialysis is rarely required except to make the patient fit for intervention (e.g., life-threatening hyperkalemia, severe fluid overload)
Key principle: Nephrostomy can be used to gauge potential for functional recovery in chronic obstruction - failure of kidney recovery after several weeks of drainage strongly suggests irreversible structural damage, making definitive surgery unlikely to benefit.
- Comprehensive Clinical Nephrology, 7th ed., p. 861-863
Emergency / Temporizing Measures (Any Cause)
Before definitive treatment, urgent decompression may be needed when:
- Obstruction with infection (pyonephrosis/urosepsis)
- AKI or azotemia from obstruction of solitary or bilateral kidneys
- Severe unrelenting pain
| Approach | When to Use |
|---|---|
| Percutaneous nephrostomy (PCN) | First-line emergency for upper urinary tract obstruction; achievable under local anesthetic; avoids general anesthesia; decompresses >70% without dialysis |
| Retrograde ureteral stent | Upper tract obstruction; requires cystoscopy (usually GA); preferred over PCN in grade 1-2 ureteral injuries |
| Urethral catheter | Obstruction distal to the bladder (BPH, urethral stricture) |
| Suprapubic cystostomy | When urethral catheter cannot be passed |
In bilateral obstruction: place nephrostomy in the kidney with more preserved parenchyma first; bilateral nephrostomies may be required to maximize functional recovery.
- Comprehensive Clinical Nephrology, 7th ed., p. 862
1. Pelviureteric Junction (PUJ) Obstruction
Most common cause of unilateral hydronephrosis (incidence 1:500 live births)
Indications for Surgery
- Functionally significant PUJ obstruction (confirmed on diuretic renography or MRU)
- Pre-operative drainage (stent or nephrostomy) only in select cases: infection, azotemia from solitary/bilateral obstruction, or severe pain
Definitive Surgery: Anderson-Hynes Dismembered Pyeloplasty
- Gold standard - success rate ~95%
- Works regardless of whether ureteral insertion is high or dependent
- Allows: reduction of redundant pelvis, excision of adynamic/dysplastic segment, preservation of crossing lower pole vessels (ureter anastomosed anterior to vessel)
- Ureter spatulated along its lateral border; anastomosis with 5-0 or 6-0 absorbable monofilament suture
- Internal ureteral stent placed routinely in adults, removed 4-6 weeks post-op
- External closed suction drain placed near (not on) suture line
Surgical Approaches (equivalent outcomes):
| Approach | Notes |
|---|---|
| Laparoscopic (transperitoneal or retroperitoneal) | Standard; largely replaced open surgery; less morbidity, comparable long-term outcomes |
| Robotic-assisted | Gaining traction in pediatric patients; reduced complications but high cost |
| Open | Reserved for complex/secondary cases with active inflammation |
Alternatives (inferior outcomes):
- Endopyelotomy or balloon dilation: higher recurrence rate - outcomes inferior to open/laparoscopic pyeloplasty
Other Techniques (historical/niche):
-
Y-V plasty (Foley) - for high ureteric insertion with small pelvis
-
Heineke-Mikulicz reconstruction
-
Davis intubated ureterotomy
-
Hellstrom vascular relocation (for crossing vessel without dismemberment)
-
Campbell-Walsh-Wein Urology, p. 2601-2605; Smith & Tanagho's General Urology, 19th ed.; Comprehensive Clinical Nephrology, 7th ed., p. 863
2. Ureteral Calculi
Most common acquired cause of ureteral obstruction
Treatment involves: relief of pain + elimination of obstruction + treatment of infection
| Stone Size / Location | Treatment |
|---|---|
| Small stones <5 mm | Medical expulsion therapy (alpha-blockers e.g., tamsulosin) - await spontaneous passage |
| 5-10 mm, uncomplicated | ESWL (extracorporeal shock wave lithotripsy) or ureteroscopy (URS) |
| >10 mm, impacted, or failed ESWL | Ureteroscopy with laser lithotripsy |
| Large staghorn / upper tract stones | Percutaneous nephrolithotomy (PCNL) |
| Obstruction + sepsis | Emergency PCN or retrograde stenting first, then interval stone removal |
Ureteral obstruction by papillary tissue, blood clots, or fungus ball is treated by procedures similar to those for calculi.
- Comprehensive Clinical Nephrology, 7th ed., p. 863
3. Benign Prostatic Hyperplasia (BPH)
Most common cause of lower urinary tract obstruction in males
Conservative (Watchful Waiting)
- Patients with minimal symptoms, no infection, and normal upper urinary tract can be observed until symptoms warrant intervention
Medical Therapy
| Drug Class | Examples | Mechanism |
|---|---|---|
| Alpha-1 blockers | Tamsulosin, alfuzosin, silodosin | Relax smooth muscle of prostate/bladder neck; rapid symptom relief |
| 5-alpha reductase inhibitors | Finasteride, dutasteride | Reduce prostate volume; prevent progression; best for large prostates |
| Combination | Alpha-blocker + 5-ARI | Superior to monotherapy for preventing progression (MTOPS/CombAT trials) |
| PDE-5 inhibitors | Tadalafil | Also improves LUTS |
Surgical Therapy
| Procedure | Indication |
|---|---|
| TURP (gold standard) | Moderate-to-large prostate; refractory to medical therapy |
| Laser enucleation (HoLEP) | Large prostates; less bleeding |
| Open prostatectomy (Millin's) | Very large prostates (>80-100 g) |
| TUNA / TUMT | Minimally invasive; less durable |
- Comprehensive Clinical Nephrology, 7th ed., p. 863; Campbell-Walsh-Wein Urology, p. BPH chapter
4. Carcinoma of Prostate / Bladder / Cervix / Uterus
Malignant ureteric obstruction - often bilateral, poor prognosis
Immediate Decompression
- PCN or retrograde ureteral stent as bridge to treatment
- Metallic stents may provide more durable decompression in malignant ureteric obstruction vs. plastic stents
- Extra-anatomic stents (tunneled percutaneously from kidney to bladder in the abdominal wall): used when conventional stents have failed or ureters are impassable due to disease
Definitive Management
- Treat the underlying malignancy (chemotherapy, radiotherapy, surgery)
- Lymphoma causing obstruction: may respond dramatically to chemotherapy alone
- Long-term stenting or nephrostomy as palliative therapy for those unfit for major surgery or incurable disease
- Ileal conduit (urinary diversion): for patients with extensive pelvic malignancy or radiation damage
A "realistic medicine" approach is important - surgical management of malignant obstruction can reduce quality of life and carries significant complication risks; patient selection is paramount.
- Comprehensive Clinical Nephrology, 7th ed., p. 863
5. Retroperitoneal Fibrosis
Ureters encased in dense fibrous retroperitoneal tissue
| Treatment | Details |
|---|---|
| Ureteral stenting | Temporizing; long-term adverse effects with chronic stenting |
| Corticosteroids | Relief of obstruction in idiopathic RPF; also for IgG4-related RPF |
| Ureterolysis | Surgical freeing of ureters from fibrous encasement; can be combined with steroid therapy to prevent recurrence |
| Robotic ureterolysis | Available in specialist centers; may offer durable cure preferable to long-term stents + steroids |
In IgG4-related retroperitoneal fibrosis, corticosteroids alone may be sufficient and highly effective.
- Comprehensive Clinical Nephrology, 7th ed., p. 863
6. Urethral Stricture
| Step | Treatment |
|---|---|
| Acute/emergency | Urethral catheter; if impassable → suprapubic cystostomy |
| Short/mild stricture | Direct-vision internal urethrotomy (DVIU) or dilation |
| Definitive | Urethroplasty (gold standard for longer/recurrent strictures) - onlay graft or excision and primary anastomosis |
| Evolving | Urethral stenting |
Repeated DVIU or dilation has high recurrence rates and is not a definitive solution for most strictures.
- Comprehensive Clinical Nephrology, 7th ed., p. 863
7. Neurogenic Bladder (Spinal Cord Damage)
| Treatment | Details |
|---|---|
| Clean intermittent catheterization (CIC) | First-line for incomplete bladder emptying; preserves upper tracts |
| Indwelling urethral/suprapubic catheter | For those unable to perform CIC |
| Anticholinergics | Oxybutynin, tolterodine - reduce detrusor overactivity |
| Intravesical botulinum toxin | For refractory neurogenic detrusor overactivity |
| Sacral neuromodulation | Selected cases |
| Urinary diversion | Ileal conduit for severe cases refractory to all measures |
8. Pyonephrosis (Infected Hydronephrosis)
A urological emergency.
- Urgent PCN drainage (or retrograde stenting if feasible)
- IV antibiotics covering gram-negatives (e.g., piperacillin-tazobactam or cephalosporin ± aminoglycoside)
- Stabilize patient; treat sepsis
- Definitive treatment of underlying cause (stone removal, stricture repair, etc.) as interval procedure once infection controlled
9. Ureterocele
- Endoscopic incision (first-line): cystoscopic puncture/incision of the ureterocele
- May cause vesicoureteral reflux post-incision - monitor
- Open surgical reconstruction for complex or failed endoscopic cases
10. Pregnancy-Related Hydronephrosis
- Usually physiological and transient (right side > left due to uterine dextrorotation and right ovarian vein)
- Conservative management - resolves spontaneously post-delivery
- Ureteral stent or PCN only if symptomatic obstruction with infection or significant pain
11. Antenatal Hydronephrosis (ANH)
| Risk Category | Management |
|---|---|
| Low risk | Postnatal ultrasound at ≥48 hours; repeat US every 1-3 months |
| High risk | VCUG + antibiotic prophylaxis + functional scan (MAG3 diuresis renography after 4-6 weeks) + monthly follow-up |
-
Majority of ANH cases are transient and resolve spontaneously after birth
-
Persistent significant hydronephrosis with confirmed PUJ obstruction and differential function <40%: pyeloplasty
-
Bailey and Love's Surgery, 28th ed., p. 3450-3451
Summary Table
| Cause | Definitive Treatment |
|---|---|
| PUJ obstruction | Anderson-Hynes dismembered pyeloplasty (laparoscopic/robotic) |
| Ureteric calculus | ESWL / URS / PCNL (size-dependent) |
| BPH | Alpha-blocker → 5-ARI → TURP |
| Malignant obstruction | Stent/PCN + treat primary malignancy |
| Retroperitoneal fibrosis | Ureterolysis + corticosteroids |
| Urethral stricture | DVIU → urethroplasty |
| Neurogenic bladder | CIC / catheter / botox / neuromodulation |
| Pyonephrosis | Emergency PCN + IV antibiotics |
| Ureterocele | Endoscopic incision |
| Pregnancy | Watchful waiting |
| ANH | Risk-stratified surveillance / pyeloplasty if persistent |
Sources: Comprehensive Clinical Nephrology 7th ed., p. 861-863 | Campbell-Walsh-Wein Urology, p. 2601-2605 | Smith & Tanagho's General Urology, 19th ed. | Bailey and Love's Surgery 28th ed., p. 3450
This is a shared conversation. Sign in to Orris to start your own chat.