Why pain is radiating left arm in angina pectoris and give pathophysiology othis physiology
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
I now have everything needed for a thorough, well-illustrated answer. Here is the complete explanation:
Angina Pectoris: Why Pain Radiates to the Left Arm + Full Pathophysiology
1. What is Angina Pectoris?
Angina pectoris is a paroxysmal, recurrent substernal chest discomfort caused by transient myocardial ischemia (lasting 15 seconds to 15 minutes) that is insufficient to cause myocyte necrosis (i.e., no infarction yet). The classic description is a crushing, squeezing, or pressure-like sensation beneath the sternum that radiates to the left arm, left jaw, shoulder, neck, and teeth.
Robbins Pathologic Basis of Disease, p. 1152-1154
2. Why Does Pain Radiate to the Left Arm? (Referred Pain Mechanism)
This is a classic example of visceral referred pain, explained by two complementary theories:
A. Embryological / Dermatomal Convergence Theory (Guyton & Hall)
"The reason for this distribution of pain is that during embryonic life, the heart originates in the neck, as do the arms. Therefore, both the heart and these surface areas of the body receive pain nerve fibers from the same spinal cord segments (C8-T5)."
- Guyton and Hall Textbook of Medical Physiology, p. 274
The heart and the medial arm/shoulder share the same spinal nerve segments (C8 to T5, particularly T1-T4). Pain signals from the ischemic heart travel along cardiac sympathetic and vagal afferents into the same dorsal horn neurons that also receive sensory input from the left arm and shoulder.
B. Convergence-Projection Theory (Ganong / Harrison's)
This is the neurophysiological explanation:
"The basis for referred pain may be convergence of somatic and visceral pain fibers on the same second-order neurons in the dorsal horn that project to the thalamus and then to the somatosensory cortex. When the visceral stimulus is prolonged, facilitation of activity from the somatic fiber endings occurs... the brain cannot determine whether the stimulus came from the viscera or from the area of referral."
- Ganong's Review of Medical Physiology, p. 1199
Diagram - Convergence-Projection Theory of Referred Pain:
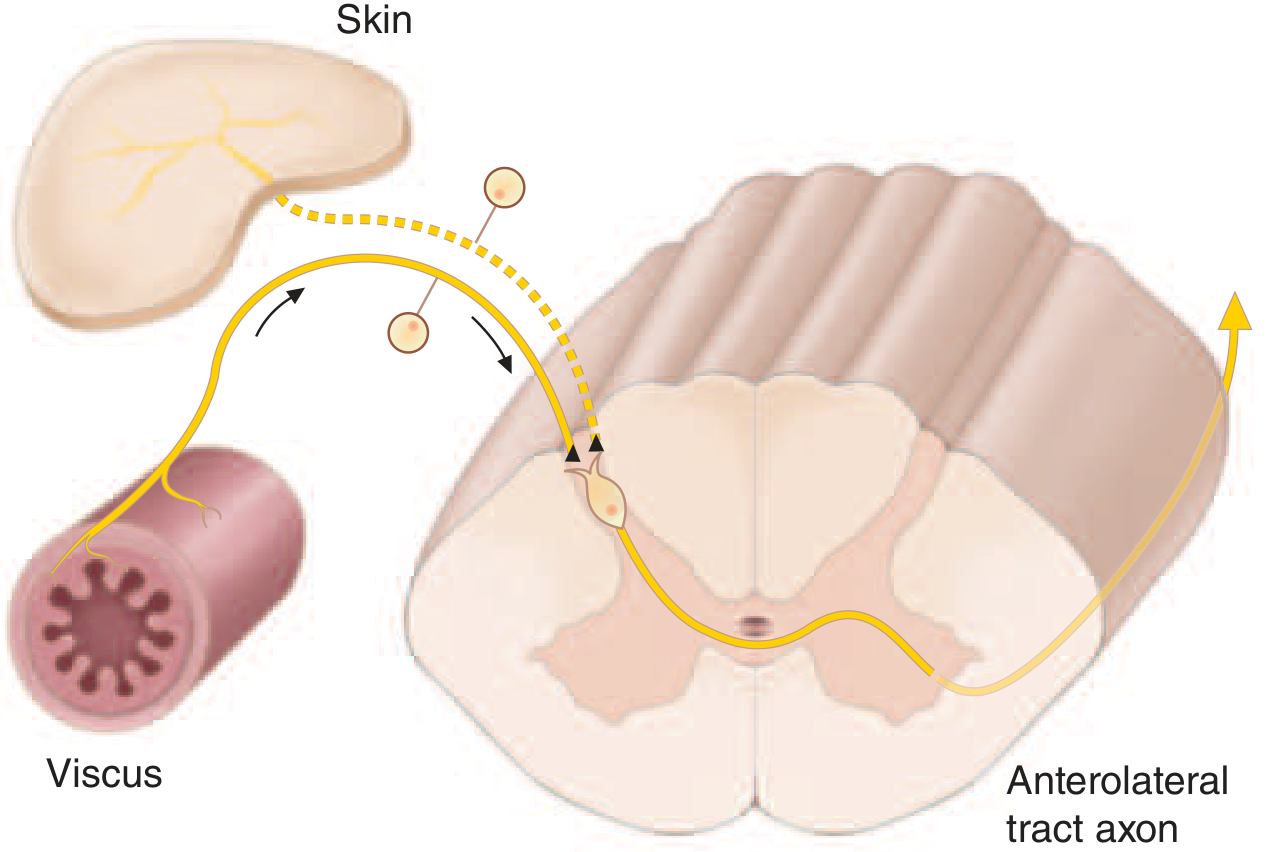
The visceral pain fiber from the ischemic heart and the somatic fiber from the left arm skin both synapse on the same dorsal horn neuron. The brain "projects" the sensation to the arm because it has far more experience receiving signals from the arm than from the heart. (Harrison's Principles of Internal Medicine, 22nd Ed.)
Diagram - Pain modulation pathways (Ganong's):
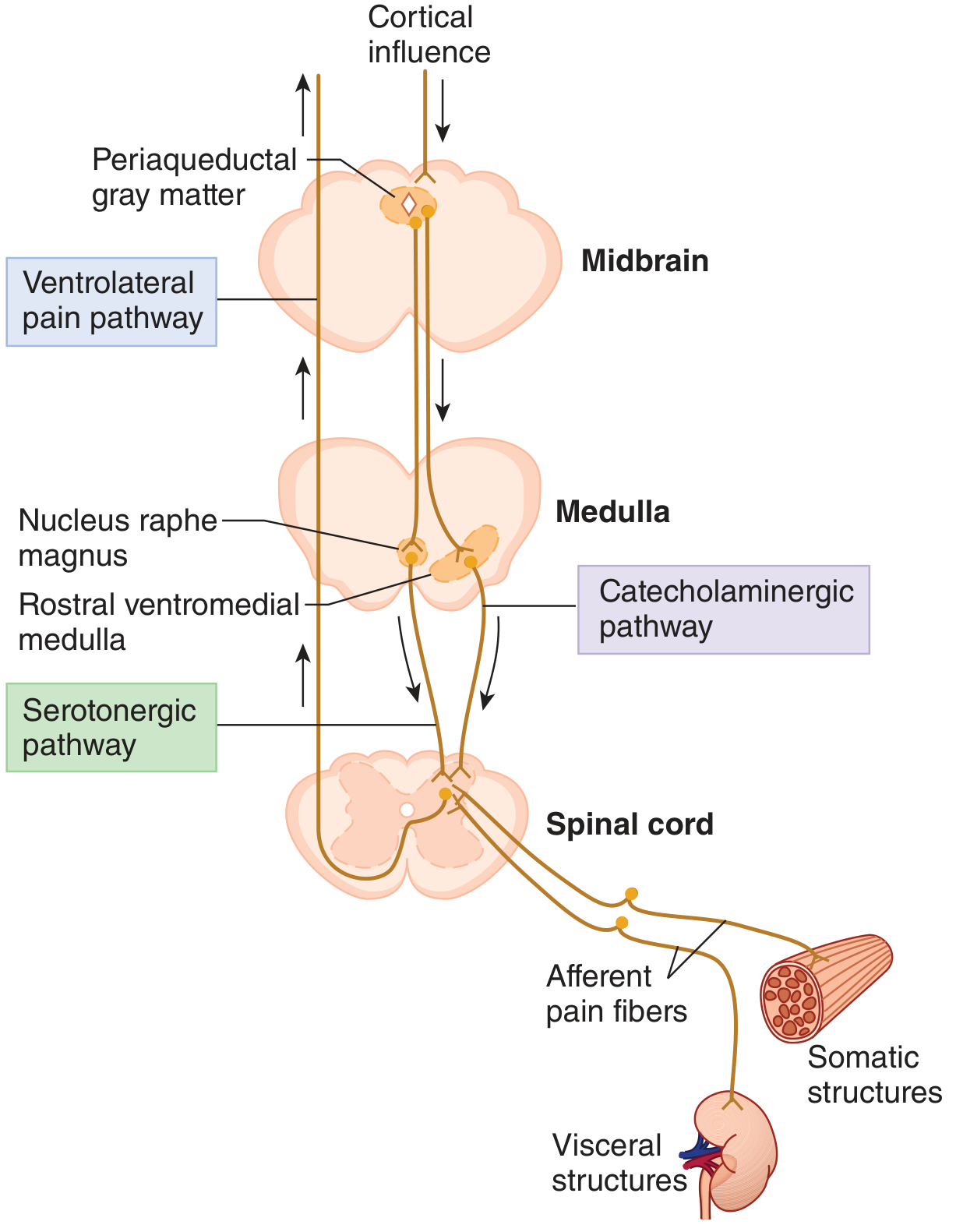
Pain from both visceral (cardiac) and somatic (arm) afferents travels via the ventrolateral spinothalamic tract, with modulation from serotonergic and catecholaminergic descending pathways. (Ganong's Review of Medical Physiology, 26th Ed.)
Step-by-Step Pathway of Referred Pain in Angina:
| Step | What Happens |
|---|---|
| 1. Myocardial ischemia | Reduced coronary blood flow causes ATP depletion and anaerobic metabolism |
| 2. Release of pain mediators | Adenosine, bradykinin, lactic acid, histamine, kinins, proteolytic enzymes accumulate |
| 3. Activation of cardiac afferents | These chemicals stimulate nociceptors in cardiac muscle; pain travels via cardiac sympathetic fibers (C8-T5) to the dorsal horn |
| 4. Convergence in dorsal horn | Cardiac visceral afferents synapse on the same second-order neurons as somatic fibers from left arm and shoulder (T1-T4 dermatomes) |
| 5. Signal ascends via spinothalamic tract | Ascends contralaterally through the anterolateral tract to the thalamus (VPL nucleus) |
| 6. Cortical misinterpretation | The somatosensory cortex, which has far more representation for the arm than the heart, "projects" the pain to the left arm - the brain cannot distinguish the true source |
3. Full Pathophysiology of Angina Pectoris
Underlying Cause: Supply-Demand Mismatch
The fundamental mechanism is an imbalance between myocardial oxygen supply and demand:
Decreased Supply:
- Atherosclerotic coronary artery stenosis (most common) - fixed narrowing reduces baseline perfusion reserve
- Coronary vasospasm (Prinzmetal/variant angina)
- Thrombosis (unstable angina)
- Anaemia or hypoxia reducing oxygen-carrying capacity
Increased Demand:
- Physical exertion (increases heart rate, stroke volume, contractility)
- Emotional stress - sympathetic activation
- Cold exposure - peripheral vasoconstriction raises afterload
- Full stomach - vagal stimulation + increased cardiac work
- Tachycardia of any cause - reduces diastolic perfusion time
Sequence of Events (Ischemic Cascade):
Coronary stenosis / spasm
↓
Reduced subendocardial blood flow (subendocardium most vulnerable - highest wall tension)
↓
O2 supply < O2 demand
↓
Anaerobic glycolysis → lactic acid accumulation → intracellular acidosis
↓
ATP depletion → failure of Na+/K+ ATPase → cellular K+ loss
↓
Diastolic dysfunction (impaired relaxation) FIRST, then systolic dysfunction
↓
ECG changes: ST depression (subendocardial ischemia) or ST elevation (transmural)
↓
Release of adenosine, bradykinin, histamine, kinins → stimulate cardiac nociceptors
↓
Pain: substernal + referred to left arm/jaw/neck
↓
If ischemia resolves (rest / nitroglycerin) → NO necrosis (angina)
If ischemia persists (>20-40 min) → myocyte death → MI
Chemical Mediators of Anginal Pain:
| Mediator | Role |
|---|---|
| Adenosine | Primary pain-producing substance; activates A1 receptors on cardiac afferents |
| Bradykinin | Potent sensitizer of cardiac C-fibers |
| Lactic acid | Acidosis activates acid-sensing ion channels (ASICs) on nociceptors |
| Histamine | Released from mast cells during ischemia; sensitizes nociceptors |
| Kinins & proteolytic enzymes | Released from damaged/ischemic cells; not cleared rapidly due to slow coronary flow |
Robbins Pathologic Basis of Disease: "Anginal pain is a consequence of ischemia-induced release of adenosine, bradykinin, and other molecules that stimulate sympathetic and vagal afferent nerves."
4. Three Patterns of Angina Pectoris
| Type | Mechanism | Features |
|---|---|---|
| Stable (typical) angina | Fixed atherosclerotic stenosis + increased demand | Predictable with exertion; relieved by rest within 1-5 min or sublingual nitroglycerine |
| Prinzmetal (variant) angina | Coronary artery vasospasm | Occurs at rest, no relation to exertion; ST elevation; responds to vasodilators |
| Unstable angina | Plaque rupture + thrombus + vasospasm | Increasing frequency/severity; occurs at rest; >20 min duration; harbinger of MI |
Robbins Pathologic Basis of Disease, p. 1155-1160
5. Clinical Features Summary
- Location: Substernal / retrosternal, described as pressure, heaviness, or squeezing
- Radiation: Left arm (especially ulnar aspect of forearm and hand), left jaw, neck, back, interscapular region - NOT below umbilicus or above mandible
- Duration: Typically 2-5 minutes (stable); up to 15-20 minutes
- Levine's sign: Patient places clenched fist over sternum when describing pain
- Precipitants: Exertion, emotion, cold, heavy meal
- Relief: Rest within 1-5 min; sublingual nitroglycerin within minutes
Harrison's Principles of Internal Medicine, 22nd Ed., p. 2136
Summary - Why Left Arm?
The left arm pain in angina is referred pain occurring because:
- Embryological origin - the heart and arm develop from the same cervical segments (C8-T5), so they share the same spinal nerve supply
- Convergence-projection - cardiac visceral pain fibers and arm somatic pain fibers converge onto the same dorsal horn neurons (T1-T4); the brain, having much more experience with arm pain than heart pain, mislocates the source to the arm
This is why pain also radiates to the left jaw (same C5 contribution) and left shoulder, but not to the trapezius (which is innervated by C3-C4 - a different segment, more typical of pericarditis).
Sources: Guyton & Hall Medical Physiology, p. 274 | Robbins Pathologic Basis of Disease, p. 1152-1160 | Ganong's Review of Medical Physiology, 26th Ed., p. 1199 | Harrison's Principles of Internal Medicine, 22nd Ed., p. 2136
This is a shared conversation. Sign in to Orris to start your own chat.