structure of hip join for biomechanics
hip joint structure anatomy biomechanics ball socket acetabulum femoral head
https://www.ncbi.nlm.nih.gov/books/NBK526019
hip joint biomechanics forces moments muscles loading gait
https://eprints.whiterose.ac.uk/id/eprint/103350/3/David%20L…
structure of hip join for biomechanics according to cynthis norkins
Cynthia Norkin Joint Structure Function hip joint biomechanics structure acetabulum femoral head
https://www.minams.edu.pk/cPanel/ebooks/miscellaneous/Joint%…
Levangie Norkin "hip complex" "structure of hip joint" acetabulum femoral neck angle anteversion trabecular
https://www.minams.edu.pk/cPanel/ebooks/miscellaneous/Joint%…
Structure of the Hip Joint for Biomechanics
Per Levangie & Norkin - Joint Structure and Function: A Comprehensive Analysis (4th/5th ed.), Chapter 10: The Hip Complex
Overview
1. Proximal Articular Surface - The Acetabulum
Formation
Articular Surface
- The lunate surface (horseshoe-shaped) is the true articular area, lined with hyaline cartilage
- The acetabular fossa is the non-articular central depression, filled with the fat pad and housing the ligamentum teres attachment
- The acetabulum is deficient inferiorly at the acetabular notch, bridged by the transverse acetabular ligament
Center Edge (CE) Angle of Wiberg
- Normal adults: ~38° in men, ~35° in women (range 22°-42°)
- A decreased CE angle = shallow acetabulum = less coverage = greater instability risk and predisposition to hip dysplasia
Acetabular Anteversion
Acetabular Labrum
- A fibrocartilaginous rim attached to the bony acetabular margin
- Deepens the acetabulum and increases the surface area contacting the femoral head
- Acts as a gasket/seal, creating negative intra-articular pressure that contributes significantly to hip stability (Norkin notes that atmospheric pressure in hip flexion plays a stronger stabilizing role than capsuloligamentous structures)
- Enhances joint lubrication when properly fitted to the femoral head
- The transverse acetabular ligament is considered part of the labrum (inferiorly), though it contains no cartilage cells; it protects blood vessels traversing the acetabular notch
2. Distal Articular Surface - The Femoral Head and Neck
Femoral Head
- Represents approximately two-thirds of a sphere
- Covered with hyaline cartilage except at the fovea capitis (small pit for ligamentum teres attachment)
- Faces superiorly, medially, and anteriorly
Angle of Inclination (Neck-Shaft Angle)
- Normal adult: ~125° (range 115°-140°)
- At birth: ~150° - decreases with weight-bearing during childhood
- Coxa valga: angle >125° - brings weight-bearing line closer to the femoral shaft, reduces bending stress on neck, but decreases abductor muscle moment arm, requiring greater abductor force for pelvic stabilization; also reduces acetabular coverage, predisposing to dislocation
- Coxa vara: angle <115° - increases bending stress on the femoral neck (greater shear force), but increases abductor moment arm (mechanically more efficient abductors)
Angle of Anteversion (Femoral Torsion)
- Normal adult: ~15°-20° anterior (anteversion)
- Newborn: ~31°; decreases ~1.5°/year until ~age 15
- Increased anteversion (>20°): femoral head faces more anteriorly than the acetabulum - joint incongruence; leads to toe-in gait, risk of anterior impingement and OA
- Retroversion (<15° or posterior): head faces posteriorly, risk of posterior instability
- The neck-shaft angle offsets the femoral shaft laterally from the pelvis, giving the hip abductor muscles their working moment arm
3. Articular Congruence
- Maximum congruence: occurs with combined flexion, abduction, and lateral rotation - this matches the fetal/infant position and is the position of maximum joint surface contact
- Close-packed position: hip extension with slight abduction and medial rotation - ligaments wind tightly around femoral head/neck, drawing the head into the acetabulum, giving maximum capsuloligamentous stability
- When the hip is neither maximally congruent nor close-packed (e.g., flexion + adduction), it is most vulnerable to traumatic dislocation
4. Hip Joint Capsule and Ligaments
Capsule
- Attaches proximally to the entire acetabular periphery (beyond the labrum)
- Thickened anterosuperiorly where predominant weight-bearing stresses occur
- Thin and loosely attached posteroinferiorly
- Contains longitudinal and oblique fibers; circumferential fibers near the proximal attachment form the zona orbicularis - a locking ring around the femoral neck that resists distraction forces
Three Extracapsular Ligaments
| Ligament | Origin | Insertion | Motion Limited |
|---|---|---|---|
| Iliofemoral (Y-ligament of Bigelow) | Anterior inferior iliac spine (AIIS) + acetabular rim | Intertrochanteric line (two bands) | Extension, lateral rotation, abduction; strongest ligament in the body |
| Pubofemoral | Superior pubic ramus | Anterior intertrochanteric fossa (blends with iliofemoral) | Abduction, extension |
| Ischiofemoral | Ischial portion of acetabular rim | Posterior femoral neck / greater trochanter | Internal rotation in extension; limits extension |
- Each hip motion is checked by at least one portion of one ligament
- All ligaments and the capsule tighten maximally with full hip extension
- Anterior ligaments (especially iliofemoral) are stronger/stiffer than posterior
Intracapsular Ligament
- Ligamentum teres (ligament of the femoral head): runs from the acetabular fossa/transverse ligament to the fovea capitis; encloses the artery to the femoral head (branch of obturator artery); plays a minor mechanical role in adults but provides a proprioceptive function and is a minor stabilizer in extreme positions
5. Structural Adaptations to Weight-Bearing
Trabecular Architecture of the Proximal Femur
- Principal compressive group: runs from the medial femoral cortex superiorly to the femoral head - resists compressive loads
- Principal tensile group: runs from the lateral cortex, arching superiorly to the femoral head - resists tensile/bending loads
- Ward's triangle: a relatively weak area between the two principal groups; site of susceptibility to femoral neck fractures
- The greater trochanteric group reinforces the region of abductor force transmission
Acetabular Weight-Bearing
- The superior dome of the acetabulum bears the predominant compressive load in standing
- In bilateral stance: joint reaction force ≈ 1/3 body weight per hip
- In unilateral stance (single-leg stance during gait): abductor muscles must contract vigorously to prevent contralateral pelvic drop (Trendelenburg), generating a total joint reaction force of approximately 3× body weight (and up to 6× BW during running)
- Norkin calculates that ~2/3 of the total hip abductor force (~917 N) acts vertically downward on the pelvis; ~1/3 (~454 N) pulls the pelvis laterally into the femoral head, producing a net compressive force of ~1605 N through the primary weight-bearing area
6. Summary: Form Follows Function
"The mature shape of the head of the femur and the acetabulum is determined by the functional interaction between these two structures."
- Normal loading during infancy and childhood is required for the acetabulum to develop its correct depth and the femoral head its spherical shape
- Disruption (e.g., developmental dysplasia of the hip) causes a shallow acetabulum, reduced CE angle, poor coverage, and biomechanically inefficient abductor moment arms
- Every structural angle (CE angle, neck-shaft angle, anteversion) has direct biomechanical consequences for force distribution, muscle efficiency, and stability
Create a visual summary diagram of hip angles and ligaments
Medical education diagram showing hip joint angles and ligaments, clean anatomical illustration style on white background. Two main sections side by side: LEFT SECTION - "Hip Joint Angles": 1. Neck-Shaft Angle (frontal plane view of proximal femur): Show femoral head, neck, and shaft with angle arc labeled "Normal: 125°", with smaller insets showing Coxa Valga (>125°) and Coxa Vara (<115°) 2. Angle of Anteversion (transverse/top-down view of femur): Show femoral neck twisted forward relative to knee condyle axis, labeled "Normal: 15-20° anterior", with arrow indicating anterior direction 3. Center Edge (CE) Angle of Wiberg (frontal view of acetabulum + femoral head): Show vertical line through femoral head center and line to lateral acetabular rim forming the CE angle arc, labeled "Normal: 35-38°" RIGHT SECTION - "Hip Joint Ligaments" (anterior view of hip joint): Draw hip joint with pelvis and proximal femur, showing three colored ligament bands: - ILIOFEMORAL LIGAMENT (Y-ligament of Bigelow) in blue: inverted Y-shape on anterior hip, labeled "Limits: extension, lateral rotation, abduction - Strongest ligament in body" - PUBOFEMORAL LIGAMENT in green: inferior-medial band, labeled "Limits: abduction, extension" - ISCHIOFEMORAL LIGAMENT in orange: shown on posterior view inset, labeled "Limits: internal rotation in extension" - ZONA ORBICULARIS shown as circular band around femoral neck, labeled "Resists distraction" Include anatomical labels: Greater trochanter, Lesser trochanter, Femoral head, Acetabulum, Intertrochanteric line, AIIS Title at top: "Hip Joint Structure - Key Angles & Ligaments (Levangie & Norkin)" Color-coded legend, clear annotation lines, professional medical textbook style
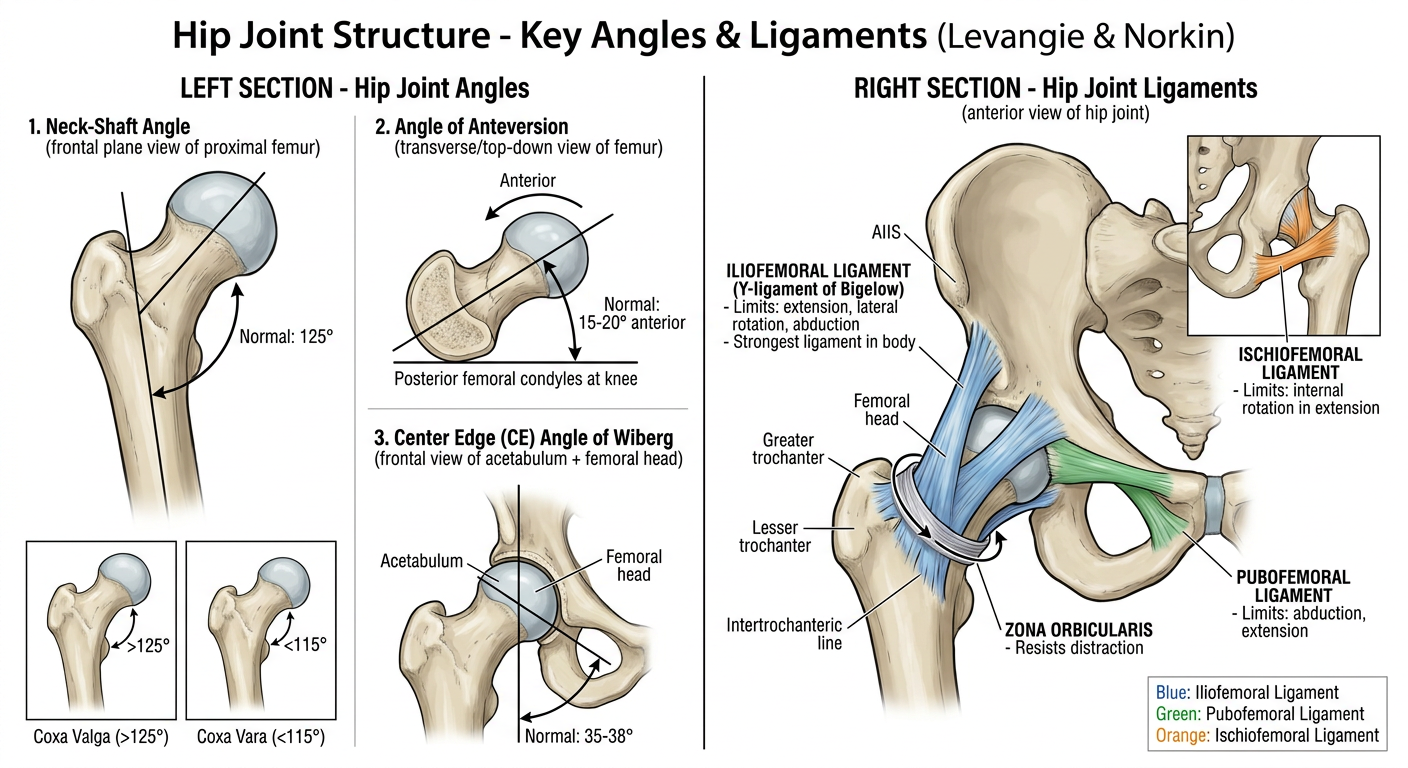
- Neck-Shaft Angle (frontal plane): Normal 125°, with coxa valga (>125°) and coxa vara (<115°) variants
- Angle of Anteversion (transverse plane): Normal 15-20° anterior twist of femoral neck relative to knee condyle axis
- Center Edge (CE) Angle of Wiberg: Normal 35-38°, measuring acetabular coverage/roof over the femoral head
- Iliofemoral (Y-ligament of Bigelow) - blue: the strongest ligament in the body; limits extension, lateral rotation, abduction
- Pubofemoral - green: limits abduction and extension
- Ischiofemoral - orange (posterior): limits internal rotation in extension
- Zona orbicularis: circular fibers around femoral neck resisting distraction
can the above answer be in pointers way...the understand better
🦴 Structure of the Hip Joint for Biomechanics
(Levangie & Norkin - Joint Structure and Function)
1. OVERVIEW
- Ball-and-socket (spheroidal) synovial joint
- Formed by: femoral head (ball) + acetabulum (socket)
- Must balance two demands: stability (weight-bearing) + mobility (locomotion)
- Connects axial skeleton to lower extremity
2. PROXIMAL ARTICULAR SURFACE - The Acetabulum
- Formed by 3 bones meeting at the triradiate cartilage:
- Ilium (superior)
- Ischium (posteroinferior)
- Pubis (anteroinferior)
- Triradiate cartilage fuses by age 20-25 years
- Lunate surface = horseshoe-shaped, lined with hyaline cartilage = true articular area
- Acetabular fossa = central non-articular depression; contains fat pad + ligamentum teres attachment
- Acetabular notch = inferior gap; bridged by transverse acetabular ligament
- Acetabulum faces laterally + inferiorly + anteriorly
3. CENTER EDGE (CE) ANGLE OF WIBERG
- Formed between:
- A vertical line through the center of the femoral head
- A line from the center of femoral head to the lateral rim of the acetabulum
- Measures the amount of acetabular coverage / "roof" over the femoral head
- Normal values:
- Men: ~38°
- Women: ~35°
- Range both sexes: 22°-42°
- Decreased CE angle = shallow acetabulum = less coverage = instability + dysplasia risk
4. ACETABULAR ANTEVERSION
- Acetabulum faces slightly anteriorly (anteversion)
- Normal: ~17°
- Works in combination with femoral anteversion to determine joint congruence
- Mismatch between femoral and acetabular anteversion → incongruence → OA risk
5. ACETABULAR LABRUM
- Fibrocartilaginous rim attached to bony acetabular margin
- Functions:
- Deepens the acetabulum → increases surface contact area
- Creates a gasket/seal → generates negative intra-articular pressure
- Negative pressure contributes MORE to stability than capsuloligamentous structures (especially in hip flexion)
- Enhances joint lubrication
- Transverse acetabular ligament = inferior portion of labrum (no cartilage cells); protects blood vessels at acetabular notch
6. DISTAL ARTICULAR SURFACE - Femoral Head & Neck
- Represents approximately 2/3 of a sphere
- Covered with hyaline cartilage except at the fovea capitis (attachment of ligamentum teres)
- Faces superiorly + medially + anteriorly
7. ANGLE OF INCLINATION (Neck-Shaft Angle)
- Angle between femoral neck axis and femoral shaft in the frontal plane
- Normal adult: ~125° (range 115°-140°)
- At birth: ~150° → decreases as child starts weight-bearing
| Deviation | Angle | Biomechanical Effect |
|---|---|---|
| Coxa Valga | >125° | ↓ bending stress on neck; ↓ abductor moment arm → needs more abductor force; ↓ acetabular coverage → dislocation risk |
| Coxa Vara | <115° | ↑ bending/shear stress on neck; ↑ abductor moment arm → more efficient abductors |
8. ANGLE OF ANTEVERSION (Femoral Torsion)
- Angle of femoral neck relative to femoral shaft in the transverse plane
- Measured between: line through knee condyles vs. line through femoral head/neck
- Normal adult: ~15°-20° anterior
- Developmental change:
- Newborn: ~31°
- Decreases ~1.5°/year until age 15
- Deviations:
| Deviation | Effect |
|---|---|
| Increased anteversion (>20°) | Head faces more anteriorly than acetabulum; toe-in gait; anterior impingement risk; OA |
| Retroversion (<15°) | Head faces posteriorly; posterior instability risk |
9. ARTICULAR CONGRUENCE
- Maximum congruence (maximum surface contact):
- Position = Flexion + Abduction + Lateral rotation
- Matches fetal/infant position
- Close-packed position (maximum ligamentous stability):
- Position = Extension + slight Abduction + Medial rotation
- Ligaments wind tightly around femoral neck, drawing head into acetabulum
- Most vulnerable position (neither congruent nor close-packed):
- Flexion + Adduction → highest dislocation risk
10. HIP JOINT CAPSULE
- Far more substantial and stronger than the shoulder capsule
- Structure: dense irregular fibrous tissue with longitudinal + oblique fibers
- Proximal attachment: entire acetabular periphery, beyond the labrum
- Thickened anterosuperiorly → where predominant weight-bearing stresses occur
- Thin posteroinferiorly → relatively weak area
- Zona orbicularis: circular deep fibers encircling femoral neck like a ring → resists distraction forces
11. HIP JOINT LIGAMENTS
a) Iliofemoral Ligament (Y-Ligament of Bigelow)
- Origin: Anterior inferior iliac spine (AIIS) + acetabular rim
- Insertion: Intertrochanteric line (two bands = inverted Y-shape)
- Strongest ligament in the human body
- Limits: Extension, lateral rotation, abduction
b) Pubofemoral Ligament
- Origin: Superior pubic ramus
- Insertion: Anterior intertrochanteric fossa (blends with iliofemoral)
- Limits: Abduction + extension
c) Ischiofemoral Ligament
- Origin: Ischial portion of acetabular rim (posterior)
- Insertion: Posterior femoral neck / greater trochanter
- Limits: Internal rotation in extension
Key points about all ligaments:
- Every hip motion is checked by at least one ligament
- All ligaments tighten maximally with full hip extension
- Anterior ligaments (especially iliofemoral) are stronger/stiffer than posterior
d) Ligamentum Teres (Intracapsular)
- Runs from acetabular fossa to fovea capitis of femoral head
- Encloses: artery to femoral head (branch of obturator artery)
- Minor mechanical role in adults
- Provides proprioceptive function + minor stabilizer in extreme positions
12. STRUCTURAL ADAPTATIONS TO WEIGHT-BEARING
Trabecular Architecture (Wolff's Law)
- Cancellous bone organizes along lines of stress:
- Principal compressive group: medial cortex → femoral head (resists compression)
- Principal tensile group: lateral cortex → arches to femoral head (resists bending)
- Ward's triangle: weak area between groups → common fracture site
- Greater trochanteric group: reinforces abductor force transmission zone
Joint Reaction Forces
| Activity | Joint Reaction Force |
|---|---|
| Bilateral stance (each hip) | ~1/3 body weight |
| Single-leg stance / gait | ~3× body weight |
| Running | Up to 6× body weight |
Abductor Muscle Role in Unilateral Stance
- Abductors (gluteus medius + minimus) must contract to prevent contralateral pelvic drop (Trendelenburg)
- ~2/3 of abductor force (~917 N) acts vertically downward on pelvis
- ~1/3 of abductor force (~454 N) pulls pelvis laterally into femoral head
- Net compressive force through weight-bearing area: ~1605 N (>360 lb)
13. KEY NORKIN PRINCIPLE - Form Follows Function
"The mature shape of the femoral head and acetabulum is determined by the functional interaction between these two structures."
- Normal mechanical loading during infancy/childhood → correct acetabular depth + spherical femoral head
- Disrupted loading (e.g., developmental dysplasia) → shallow acetabulum, reduced CE angle, poor coverage, inefficient abductor moment arms
- Every structural angle (CE, neck-shaft, anteversion) has direct biomechanical consequences for force distribution, muscle efficiency, and joint stability