Give a complete treatment of Spinal Tb of 5 year old boy weight 20
Reading File
Finding Sources
Finding Sources
Searching PubMed
"spinal tuberculosis" AND children AND treatment
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Searching the Web
spinal tuberculosis Pott disease child treatment WHO guidelines 2023 2024 drug doses
Reading Web Page
https://globaltb.njms.rutgers.edu/educationalmaterials/Produ…
Loading Image
Loading Image
I now have comprehensive information to provide a complete treatment guide. Let me compile the answer.
Spinal Tuberculosis (Pott Disease) — Complete Treatment Guide
Patient: 5-year-old boy, weight 20 kg
1. Overview & Pathogenesis
Spinal TB (Pott disease) is the most common extrapulmonary site of tuberculosis and the most common granulomatous spinal infection. Infection originates in the metaphysis of the vertebral body and spreads beneath the anterior longitudinal ligament, causing:
- Destruction of contiguous vertebral levels (or skip lesions in ~15%)
- Cold abscess formation (~50%)
- Relative preservation of the intervertebral disc (unlike pyogenic infection)
- Progressive kyphosis / gibbus deformity
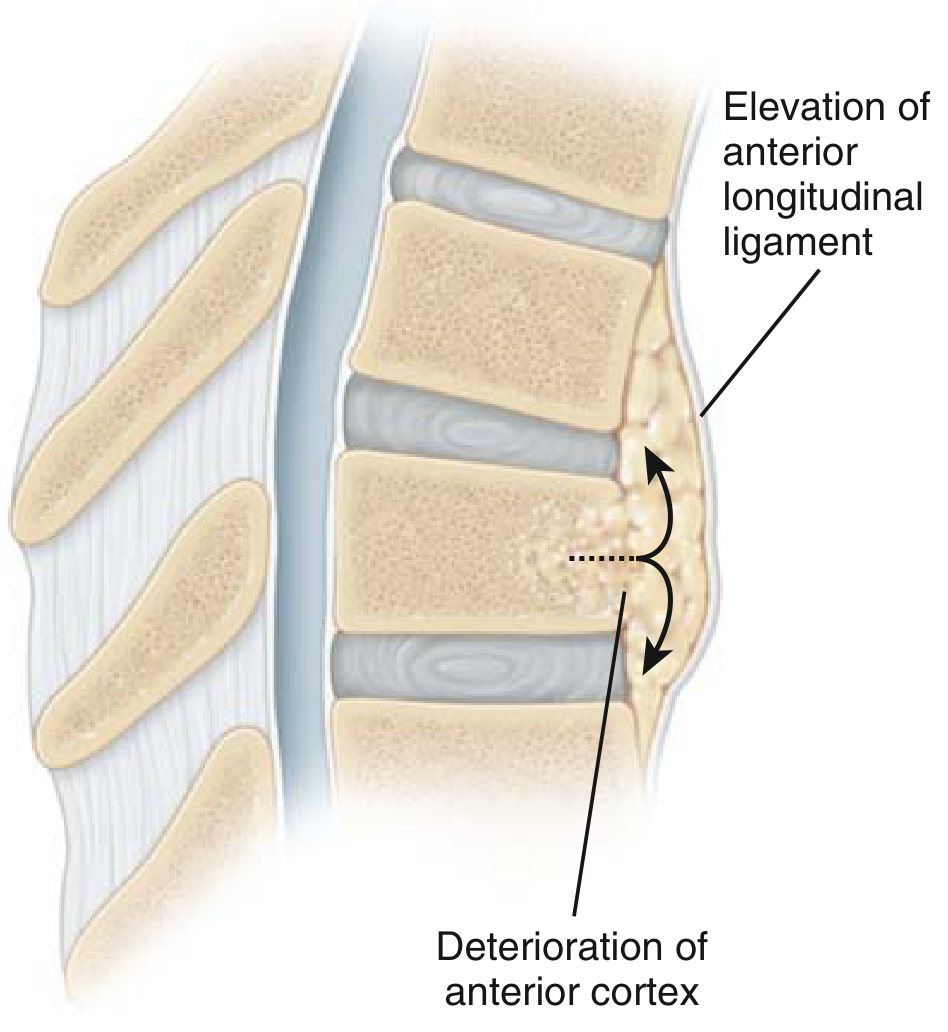
Pathogenesis: infection in the vertebral metaphysis spreads under the anterior longitudinal ligament — Miller's Review of Orthopaedics 9th Ed.
2. Diagnosis
Clinical Features
| Feature | Detail |
|---|---|
| Local | Back pain, gibbus deformity, spinal tenderness |
| Systemic | Fever, night sweats, anorexia, weight loss |
| Neurological | Weakness/paralysis of lower limbs (Pott paraplegia) — compressive myelopathy |
| Abscess | Cold paravertebral, psoas, or retropharyngeal abscess |
Investigations
| Investigation | Finding |
|---|---|
| X-ray spine | Anterior vertebral body destruction, disc space narrowing, gibbus |
| MRI spine (preferred) | Subligamentous spread, epidural or paraspinous abscess, cord compression; discordant disc signal distinguishes TB from pyogenic |
| CT-guided biopsy | AFB stain, culture, GeneXpert MTB/RIF (molecular confirmation) |
| Chest X-ray | Abnormal in ~2/3 of cases |
| Mantoux / TST | May be negative in 20% (anergy) |
| IGRA (Quantiferon) | More specific in BCG-vaccinated children |
| CBC, ESR, CRP | Raised inflammatory markers |
| Sputum AFB/culture | If pulmonary co-involvement |
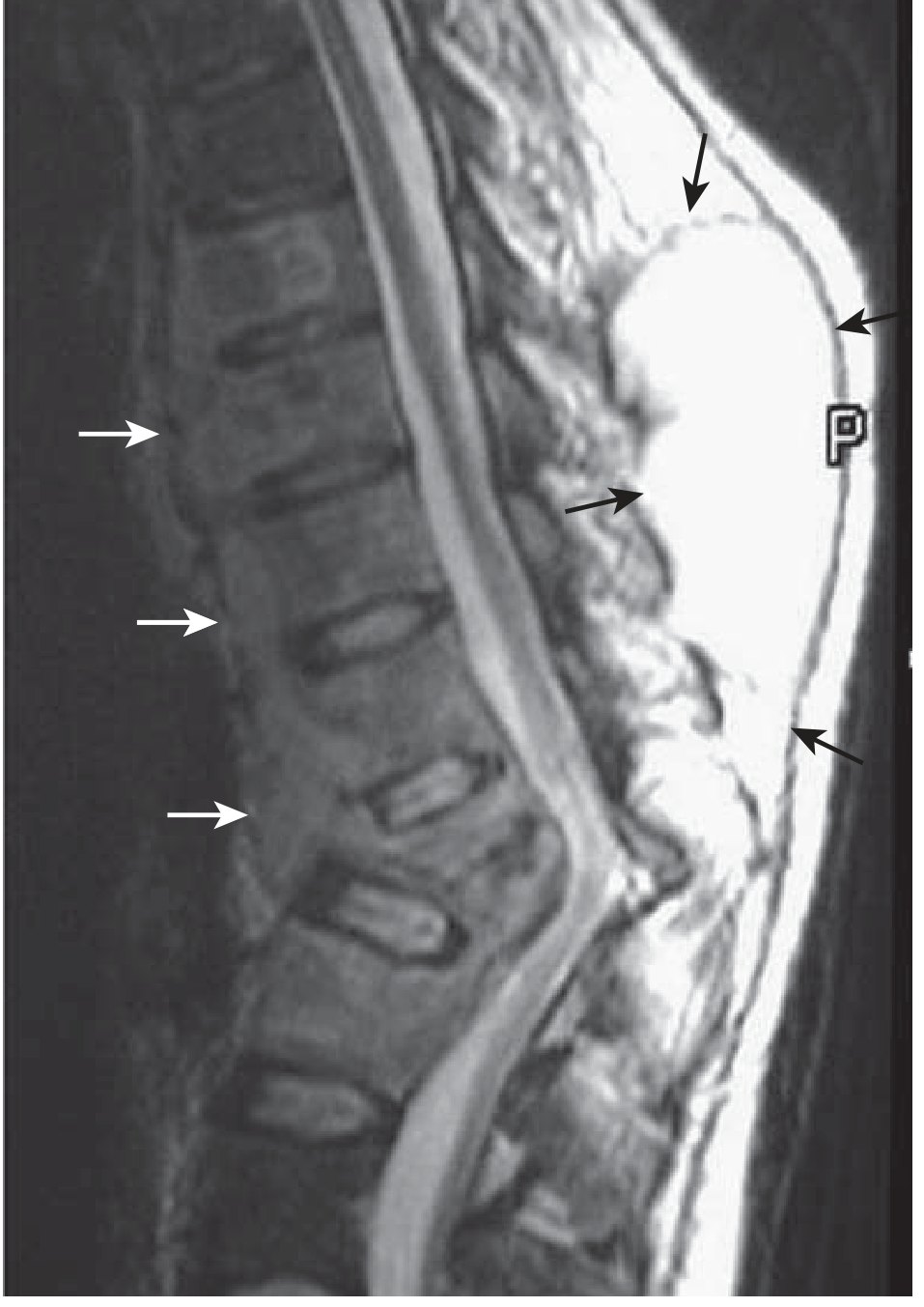
Sagittal T1-MRI: relative disc sparing, subligamentous spread (white arrows), vertebral destruction with gibbus, cold paraspinous abscesses (black arrows) — Miller's Review of Orthopaedics 9th Ed.
3. Medical Treatment (Mainstay)
Regimen — Extrapulmonary / Spinal TB (Severe Form)
For spinal TB, the standard recommended duration is 9–12 months (longer than pulmonary TB because it is a serious extrapulmonary form with poor tissue penetration):
| Phase | Duration | Drugs |
|---|---|---|
| Intensive phase | 2 months | HRZE (Isoniazid + Rifampicin + Pyrazinamide + Ethambutol) |
| Continuation phase | 7–10 months | HR (Isoniazid + Rifampicin) |
Total duration: 9–12 months (most authorities recommend 12 months for spinal TB in children, especially with cord involvement or abscess)
Drug Doses for This Child (20 kg, 5 years)
| Drug | Abbreviation | Dose | For 20 kg child | Max | Route |
|---|---|---|---|---|---|
| Isoniazid | H (INH) | 10 mg/kg/day | 200 mg/day | 300 mg | PO OD |
| Rifampicin | R (RIF) | 15 mg/kg/day | 300 mg/day | 600 mg | PO OD (empty stomach) |
| Pyrazinamide | Z (PZA) | 35 mg/kg/day | 700 mg/day | 2 g | PO OD |
| Ethambutol | E (EMB) | 20 mg/kg/day | 400 mg/day | 1 g | PO OD |
| Pyridoxine (B6) | — | 1–2 mg/kg/day | 25 mg/day | — | PO OD (with INH, to prevent neuropathy) |
Note: For serious forms of TB (including spinal/CNS), many experts use Rifampicin 20–30 mg/kg/day → for this child: up to 400–600 mg/day. Discuss with TB specialist.
Administration tip: Crush tablets, mix with a few drops of warm water, add to soft food. Liquid preparations with sorbitol cause diarrhea and are generally avoided.
Key Drug Monitoring
| Drug | Adverse Effect | Monitoring |
|---|---|---|
| INH | Hepatitis, peripheral neuropathy | LFTs monthly; give pyridoxine |
| Rifampicin | Hepatitis, orange discoloration of secretions | LFTs; warn parents |
| Pyrazinamide | Hepatotoxicity, hyperuricemia, arthralgia | LFTs; uric acid if symptomatic |
| Ethambutol | Optic neuropathy (dose >20 mg/kg) | Visual acuity, red-green color vision monthly — challenging in young children; use with caution; some guidelines omit in children <5 years unable to report visual changes |
Ethambutol caution: In children <5 years who cannot reliably report visual changes, ethambutol monitoring is difficult. Some guidelines substitute Streptomycin (15 mg/kg/day IM for 2 months) during the intensive phase, or accept the risk and monitor carefully.
DOT (Directly Observed Therapy)
All anti-TB drugs should be administered under DOT — a health worker or trained family member observes each dose ingestion. This is mandatory to prevent drug resistance.
4. Adjunctive Medical Treatment
| Agent | Indication | Dose |
|---|---|---|
| Corticosteroids (Prednisolone) | Significant cord compression / neurological deficit / severe systemic toxicity | 1–2 mg/kg/day for 4–6 weeks, then taper |
| Pyridoxine (B6) | Prevent INH neuropathy | 25 mg/day |
| Nutritional support | Malnutrition is common; improves immunity and drug tolerance | High-protein, high-calorie diet |
| Calcium & Vitamin D | Bone healing | Supplement if deficient |
5. Orthotic/Immobilization Management
| Measure | Detail |
|---|---|
| Spinal brace / TLSO | Thoracolumbosacral orthosis for thoracic/lumbar lesions; cervical collar for cervical TB. Provides pain relief, reduces kyphosis progression |
| Bed rest | Only during acute phase; prolonged bed rest is not recommended (ambulatory chemotherapy is the standard) |
| Ambulation | Early mobilization with brace once pain is controlled |
The Medical Research Council (MRC) trials demonstrated that ambulatory chemotherapy with or without bracing gives equivalent outcomes to bed rest with or without surgery in uncomplicated cases.
6. Surgical Treatment
Surgery is not routine — it is indicated in specific situations:
Surgical Indications
| Indication | Details |
|---|---|
| Neurological deficit | Motor weakness, Pott paraplegia — surgical decompression is urgent |
| Spinal instability | Vertebral collapse threatening cord |
| Progressive kyphosis | >40–50° or rapidly progressive in a growing child |
| Failure of medical management | No clinical/radiological improvement after 4–6 weeks of ATT |
| Advanced caseation/fibrosis/avascular tissue | Limits antibiotic penetration |
| Large cold abscess | Causing compressive symptoms |
Standard Surgical Procedure
Hong Kong procedure (radical anterior débridement + uninstrumented autogenous strut grafting) remains the gold standard:
- Radical anterior débridement of infected tissue
- Autogenous rib or iliac crest strut grafting to restore anterior column height
- Instrumented posterior stabilization may be added when necessary (evidence now supports this — advantages: less progressive kyphosis, earlier healing, decreased sinus formation)
Pre-operative: Start ATT ≥10 days before surgery if feasible (controversial, but recommended where possible).
Post-operative: Continue full ATT course — mandatory.
7. Management of Complications
| Complication | Management |
|---|---|
| Pott paraplegia (early, due to abscess/pus) | Surgical decompression + ATT + corticosteroids |
| Pott paraplegia (late, due to bony sequestrum/fibrosis) | Surgical debridement; prognosis more guarded |
| Cold abscess (paravertebral/psoas) | ATT alone often sufficient; CT-guided aspiration or surgical drainage if large/compressive |
| Gibbus deformity | Brace, monitor; corrective osteotomy in severe progressive cases after disease heals |
| Drug-resistant TB | Second-line drugs (bedaquiline, linezolid, clofazimine, etc.) — refer to MDR-TB specialist |
| Sinus tract | Local wound care; usually heals with ATT |
8. Follow-Up Schedule
| Time | Assessment |
|---|---|
| 2 weeks | Clinical response (pain, fever), drug tolerance, LFTs |
| Monthly | Neurological exam, LFTs, weight, compliance (DOT) |
| 3 months | X-ray spine — bone healing |
| 6 months | MRI spine if neurological involvement; assess response |
| End of treatment | X-ray/MRI, weight gain, clinical cure |
| 1 year post-treatment | Long-term kyphosis surveillance (children at risk for progressive deformity during growth) |
A 15-year prospective pediatric study (Rajasekaran et al.) showed that healed spinal TB in children can cause progressive kyphosis during growth even after chemotherapy — annual follow-up through puberty is recommended.
9. Treatment Summary Card
Patient: 5-year-old boy, 20 kg
Diagnosis: Spinal TB (Pott disease)
INTENSIVE PHASE (2 months — daily):
Isoniazid (H) 200 mg OD
Rifampicin (R) 300 mg OD (fasting)
Pyrazinamide (Z) 700 mg OD
Ethambutol (E) 400 mg OD
Pyridoxine (B6) 25 mg OD
CONTINUATION PHASE (7–10 months — daily):
Isoniazid (H) 200 mg OD
Rifampicin (R) 300 mg OD
TOTAL DURATION: 9–12 months
BRACE: TLSO for thoracolumbar lesion
DOT: Mandatory
SURGERY: If neurological deficit, instability, progressive kyphosis, or treatment failure
Sources
- Miller's Review of Orthopaedics, 9th Ed., p. 787–788
- Bradley and Daroff's Neurology in Clinical Practice — Granulomatous Vertebral Osteomyelitis
- Adams and Victor's Principles of Neurology, 12th Ed. — Treatment of CNS Tuberculous Infections
- AAP/CDC Pediatric TB Treatment Guidelines (2023 Rutgers/Globaltb update)
- WHO Consolidated Guidelines on TB, Module 4 — Drug-Susceptible TB Treatment
- Medscape: Pott Disease Treatment — ATS/CDC/IDSA 2016 guidelines endorsed 4-drug empirical regimen
This is a shared conversation. Sign in to Orris to start your own chat.