Give a notes including diagram, flowchart for malabsorption syndrome
Reading File
Finding Sources
Searching the Web
malabsorption syndrome pathophysiology classification clinical features diagnosis treatment
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Searching Images
malabsorption syndrome pathophysiology diagram
Finding Sources
Finding Sources
Searching Images
small intestine malabsorption villi absorption diagram celiac disease
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Now I have everything needed to write comprehensive notes. Let me compile them.
Malabsorption Syndrome — Comprehensive Notes
1. Definition
Malabsorption syndrome refers to impaired absorption of nutrients (macronutrients, micronutrients, vitamins, minerals) through the intestinal mucosa into the bloodstream or lymphatics. It encompasses both:
- Maldigestion — defective hydrolysis of large molecular nutrients
- Malabsorption — impaired transport of nutrients across the intestinal wall
Ganong's Review of Medical Physiology — "Various disease processes can impair absorption without a loss of intestinal length. The pattern of deficiencies that results is sometimes called the malabsorption syndrome."
2. Normal Absorption — Three-Phase Model
Understanding malabsorption requires knowing normal physiology:
┌─────────────────────────────────────────────────────────────┐
│ NORMAL DIGESTION & ABSORPTION │
│ │
│ LUMINAL PHASE MUCOSAL PHASE POST-MUCOSAL │
│ (Intraluminal) (Enterocyte) PHASE │
│ │
│ • Gastric acid • Brush border • Lymphatics │
│ secretion enzymes • Portal vein │
│ • Pancreatic • Active/passive • Chylomicron │
│ enzymes transport formation │
│ • Bile salts • Enterocyte • Systemic │
│ • Emulsification uptake circulation │
└─────────────────────────────────────────────────────────────┘
3. Classification / Causes
Diagram: Classification by Phase
┌────────────────────────────────────────────────────────────────────────┐
│ CAUSES OF MALABSORPTION SYNDROME │
├────────────────┬───────────────────────────┬───────────────────────────┤
│ LUMINAL PHASE │ MUCOSAL PHASE │ POST-MUCOSAL PHASE │
│ (Pre-mucosal) │ (Enterocyte) │ (Transport) │
├────────────────┼───────────────────────────┼───────────────────────────┤
│ Pancreatic │ Celiac disease │ Intestinal lymphangiectasia│
│ insufficiency │ (villous atrophy) │ │
│ │ │ Lymphoma │
│ Chronic │ Tropical sprue │ │
│ pancreatitis │ │ Whipple's disease │
│ │ Crohn's disease │ │
│ Cystic fibrosis│ │ Abetalipoproteinemia │
│ │ Infectious enteritis │ (chylomicron defect) │
│ Zollinger- │ (Giardia, TB, │ │
│ Ellison syn. │ Cryptosporidium) │ Right heart failure │
│ (acid inact. │ │ (raised venous pressure) │
│ pancr. enzyme) │ Short bowel syndrome │ │
│ │ │ │
│ Bile salt │ Radiation enteritis │ │
│ deficiency │ │ │
│ (cholestasis, │ Autoimmune enteropathy │ │
│ ileal resec.) │ │ │
│ │ SIBO (mucosal damage + │ │
│ SIBO (bile │ bile salt deconjugation) │ │
│ salt deconj.) │ │ │
│ │ Eosinophilic │ │
│ Post-gastrect. │ gastroenteritis │ │
│ (rapid transit)│ │ │
│ │ HIV enteropathy │ │
│ Drugs │ │ │
│ (cholestyramine│ Microvillus inclusion │ │
│ neomycin) │ disease (neonatal) │ │
└────────────────┴───────────────────────────┴───────────────────────────┘
Causes in the Tropics (Sleisenger & Fordtran)
| Category | Examples |
|---|---|
| Infections (Bacteria) | M. avium intracellulare, M. tuberculosis |
| Protozoa | Giardia lamblia, Cryptosporidium, Cyclospora, Cystoisospora |
| Helminths | Strongyloides, Capillaria philippinensis |
| Mucosal diseases | Celiac disease, Tropical sprue, HIV enteropathy |
| Pancreatic insufficiency | Tropical pancreatitis, alcoholic pancreatitis |
| Lymphatic obstruction | Intestinal lymphangiectasia |
| Specific transport defects | Abetalipoproteinemia, glucose-galactose malabsorption |
4. Pathophysiology
Flowchart: General Mechanism
┌─────────────────────────────────────────────────────────────────┐
│ MALABSORPTION PATHOPHYSIOLOGY │
└─────────────────────────────────────────────────────────────────┘
│
┌───────────────────┼──────────────────┐
▼ ▼ ▼
LUMINAL DEFECT MUCOSAL DEFECT LYMPHATIC/
VASCULAR DEFECT
│ │ │
↓ Digestion ↓ Absorption ↓ Transport
│ │ │
└───────────────────┴──────────────────┘
│
▼
┌───────────────────────────────┐
│ IMPAIRED NUTRIENT UPTAKE │
└───────────────────────────────┘
│
┌───────────────────┴──────────────────┐
▼ ▼
FAT MALABSORPTION CARBOHYDRATE &
• Steatorrhea PROTEIN MALABS.
• Fatty acid → colon • Osmotic diarrhea
• ↓ Fat-soluble vitamins • Fermentation → gas
(A, D, E, K) • Muscle wasting
• Oxalate kidney stones • Hypoproteinemia
• Bile acid loss → diarrhea • Edema
│ │
└───────────────────┬──────────────────┘
▼
┌──────────────────────────────────────┐
│ MICRONUTRIENT / VITAMIN DEFICIENCIES│
│ Iron → anemia │
│ B12/Folate → megaloblastic anemia │
│ Vitamin D/Ca²⁺ → osteomalacia │
│ Vitamin K → bleeding tendency │
│ Zinc → dermatitis │
└──────────────────────────────────────┘
Key Mechanism: Celiac Disease (Autoimmune Mucosal Injury)
GLUTEN ingestion
│
▼
Gluten peptides cross mucosa (increased permeability)
│
▼
Tissue transglutaminase (tTG) modifies gliadin peptides
│
▼
HLA-DQ2 / HLA-DQ8 antigen presentation to CD4+ T cells
│
▼
T cell-mediated immune response → cytokine release
│
▼
Intraepithelial lymphocytosis → Crypt hyperplasia → Villous atrophy
│
▼
↓ Absorptive surface area → MALABSORPTION
5. Histological Spectrum (Marsh Classification)
Villous changes in celiac disease / malabsorption:

| Marsh Stage | Histology |
|---|---|
| 0 | Normal villi, no lymphocytes |
| I | ↑ Intraepithelial lymphocytes (>25/100 enterocytes) |
| II | + Crypt hyperplasia |
| IIIa | Partial villous atrophy |
| IIIb | Subtotal villous atrophy |
| IIIc | Total villous atrophy (flat mucosa) |
6. Clinical Features
Diagram: Clinical Manifestations
MALABSORPTION SYNDROME
│
┌──────────────────┼──────────────────┐
▼ ▼ ▼
GI SYMPTOMS NUTRITIONAL SYSTEMIC
DEFICIENCIES
• Diarrhea • Weight loss • Fatigue/weakness
• Steatorrhea • Muscle wasting • Growth failure
(pale, bulky, • Edema (children)
oily, floating, (hypoalbuminemia) • Peripheral edema
offensive) • Anemia • Tetany
• Abdominal (Fe, B12, folate) (↓ Ca²⁺, Mg²⁺)
bloating/pain • Bone pain / • Peripheral
• Flatulence fractures neuropathy
• Nausea (Vit D/Ca²⁺) (B12 deficiency)
• Borborygmi • Bleeding • Night blindness
(Vit K ↓) (Vit A ↓)
• Dermatitis • Glossitis
(Zinc, Vit A) • Angular stomatitis
• Amenorrhoea • Koilonychia
• Infertility • Cheilosis
7. Investigations
Flowchart: Diagnostic Approach
SUSPECTED MALABSORPTION
(Chronic diarrhea + weight loss + nutritional deficiencies)
│
▼
┌─────────────────────────────────────────┐
│ STEP 1: CONFIRM MALABSORPTION │
│ • Stool fat test (72-hr fecal fat) │
│ Gold standard: >7 g/day on 100 g │
│ fat/day diet │
│ • Sudan stain (qualitative fat) │
│ • Serum albumin, prealbumin │
│ • CBC (anemia pattern) │
└─────────────────────────────────────────┘
│
▼ Fecal fat POSITIVE
┌─────────────────────────────────────────┐
│ STEP 2: LOCALIZE THE DEFECT │
│ │
│ Pancreatic? Mucosal? │
│ • CT/MRCP • Duodenal biopsy │
│ • Fecal elastase • tTG IgA + IgA │
│ • Secretin test (celiac) │
│ • Small bowel MRI/ │
│ SIBO? enterography │
│ • H₂ breath test │
│ (glucose/lactulose) │
│ • Jejunal aspirate │
│ culture (>10⁵/mL) │
│ │
│ Bile acid deficiency? │
│ • SeHCAT test │
│ • Serum C4, FGF19 │
└─────────────────────────────────────────┘
│
▼
┌─────────────────────────────────────────┐
│ STEP 3: SPECIFIC NUTRIENT LEVELS │
│ • Serum B12, folate, iron │
│ • Serum Ca²⁺, Vit D, Vit A, Vit K │
│ • Serum zinc, magnesium │
│ • PT/INR (Vit K) │
└─────────────────────────────────────────┘
│
▼
┌─────────────────────────────────────────┐
│ STEP 4: SPECIFIC TESTS │
│ • Stool O&P, PCR (Giardia) │
│ • Hydrogen breath test (lactose, │
│ fructose malabsorption) │
│ • Schilling test (B12 absorption) │
│ • VCE / balloon enteroscopy │
│ (if diagnosis elusive) │
└─────────────────────────────────────────┘
Key Investigations Summary Table
| Test | What it Detects | Normal Value |
|---|---|---|
| 72-hr fecal fat | Overall fat malabsorption | <7 g/day |
| Fecal elastase | Pancreatic exocrine insufficiency | >200 μg/g |
| H₂ breath test | SIBO, lactose/fructose malabsorption | <20 ppm rise |
| tTG IgA + total IgA | Celiac disease | Negative |
| D-xylose test | Mucosal absorptive capacity | >20 mg/dL at 1 hr |
| Duodenal biopsy | Villous atrophy (celiac, Whipple's) | Normal villi |
| Jejunal aspirate culture | SIBO | <10⁵ organisms/mL |
| Serum B12 / folate | Vitamin deficiency | B12 >200 pg/mL |
| SeHCAT | Bile acid malabsorption | Retention >15% |
8. Endoscopic Finding: Celiac Disease (Malabsorption)
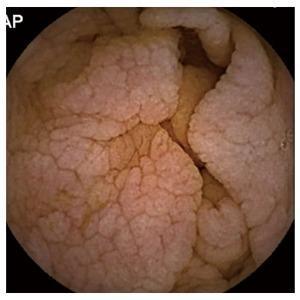
Capsule endoscopy showing villous atrophy with mosaic pattern, absent villi and scalloped folds — hallmark of celiac disease causing malabsorption
9. Treatment
Flowchart: Management
MALABSORPTION — TREATMENT
│
├──────────────────────────────────────────────┐
▼ ▼
TREAT UNDERLYING CAUSE NUTRITIONAL SUPPORT
│
┌────┴─────────────────────────────────────────┐
│ │
▼ ▼
MUCOSAL DISEASE PANCREATIC INSUFFICIENCY
• Celiac disease: • Pancreatic enzyme
Gluten-free diet replacement therapy
(wheat, rye, (PERT) with meals
barley excluded) • PPI if acid inactivating
• Crohn's disease: enzymes
Steroids, biologics • Fat-soluble vitamin
• Tropical sprue: supplementation
Tetracycline +
folic acid BILE ACID DEFICIENCY
• Whipple's disease: • Ursodeoxycholic acid
Ceftriaxone → • Fat-soluble vitamins
TMP-SMX (long term)
SIBO
• Giardiasis: • Antibiotics
Metronidazole (rifaximin, metronidazole,
tetracycline)
• Treat predisposing
structural cause
▼
NUTRITIONAL SUPPORT
• Oral supplementation:
- Fat-soluble vitamins (A, D, E, K) as water-soluble derivatives
- Iron, B12 (parenteral if ileal disease), folate
- Calcium, magnesium, zinc
• Medium-chain triglycerides (MCT) if lymphatic obstruction
(bypasses lymphatics — directly to portal vein)
• Enteral nutrition if severe
• Parenteral nutrition (TPN) in short bowel syndrome
• Small bowel transplantation (for refractory short gut)
BILE ACID DIARRHEA:
• Cholestyramine (binds bile acids → prevents secretory
action on colonocytes)
10. Specific Conditions Summary
| Condition | Key Feature | Specific Test | Treatment |
|---|---|---|---|
| Celiac disease | Villous atrophy, HLA-DQ2/DQ8 | tTG IgA, duodenal biopsy | Gluten-free diet |
| Tropical sprue | Common in tropics, responds to Abx | Jejunal biopsy, folate levels | Tetracycline + folate |
| Whipple's disease | T. whipplei, PAS+ macrophages | Small bowel biopsy | Ceftriaxone → TMP-SMX |
| Pancreatic insufficiency | Steatorrhea, no villous atrophy | Fecal elastase, CT pancreas | PERT |
| SIBO | H₂ breath test, structural abnormality | Breath test / aspirate | Rifaximin |
| Short bowel syndrome | Post-resection (>50% removed) | Clinical | TPN, transplant |
| Abetalipoproteinemia | ↓ Chylomicrons, acanthocytes | Blood smear, serum lipids | Fat-soluble vitamins |
| Lymphangiectasia | Protein-losing enteropathy | Biopsy, albumin | MCT diet, octreotide |
11. Complications
Malabsorption Syndrome
│
├── Megaloblastic anemia (B12/folate)
├── Iron deficiency anemia
├── Osteomalacia / osteoporosis (Vit D/Ca²⁺)
├── Bleeding diathesis (Vit K)
├── Peripheral neuropathy (B12)
├── Night blindness (Vit A)
├── Growth retardation (children)
├── Infertility / amenorrhoea
├── Hypoalbuminaemia → edema
├── Oxalate nephrolithiasis (fat malabs. → ↑ oxalate absorption)
├── Secondary immunodeficiency
└── Enteropathy-associated T-cell lymphoma (EATL)
(refractory celiac disease)
Key Points to Remember
- Three phases: Luminal → Mucosal → Post-mucosal. Identify which is defective.
- Steatorrhea is the cardinal sign — pale, bulky, floating, offensive stools.
- 72-hr fecal fat on 100 g fat/day is the gold standard screening test.
- tTG IgA is the first-line serological test for celiac disease; always check total IgA (IgA deficiency gives false negative).
- Fat-soluble vitamins A, D, E, K are always affected in fat malabsorption.
- MCT (medium-chain triglycerides) bypass lymphatics — useful in lymphangiectasia.
- Short bowel syndrome occurs when >50% of small intestine is resected.
- Bile acid loss after ileal resection causes both fat malabsorption and secretory diarrhea in the colon.
Sources: Ganong's Review of Medical Physiology 26th ed. | Sleisenger & Fordtran's Gastrointestinal & Liver Disease | Goldman-Cecil Medicine | Harrison's Principles of Internal Medicine 22E
This is a shared conversation. Sign in to Orris to start your own chat.