differential diagnosis for grennish color urine
Reading File
Searching the Web
green urine differential diagnosis causes
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive information from the medical library and web sources. Here is the full differential diagnosis:
Differential Diagnosis: Greenish Urine
Green or blue-green urine is most commonly benign (drug or dietary related), but can occasionally signal infection or metabolic disease. Here is the full breakdown organized by category:
1. Medications (Most Common Cause)
| Drug | Class | Mechanism |
|---|---|---|
| Propofol | IV anesthetic | Hepatic metabolism produces phenolic quinol conjugates excreted in urine; more likely with respiratory alkalosis |
| Amitriptyline | Tricyclic antidepressant | Direct dye-like effect of the drug/metabolites |
| Indomethacin | NSAID | From liver metabolism |
| Promethazine / Phenergan | Antihistamine/antiemetic | Phenothiazine ring discoloration |
| Metoclopramide | Antiemetic | Same phenothiazine class |
| Mitoxantrone | Chemotherapy (antineoplastic) | Blue-green dye properties; also turns skin/sclera blue |
| Methocarbamol | Muscle relaxant | Produces green-brown color |
| Cimetidine | H2 blocker | Blue-green discoloration |
| Triamterene | Potassium-sparing diuretic | Pale blue with blue fluorescence in acid urine |
| Flutamide | Anti-androgen | Green pigment |
| Sildenafil | PDE5 inhibitor | Rare, reported cases |
| Phenylbutazone | NSAID | Rare |
| Doxorubicin | Chemotherapy | Blue-green |
| Methylene blue | Diagnostic dye / antidote | Blue or blue-green; found in Urised, Prosed DS, Trac Tabs |
| Phenol poisoning | Toxicological | Phenol oxidized to quinones in urine, turns green |
2. Infections
- Pseudomonas aeruginosa UTI or bacteremia - the classic infectious cause. The bacterium produces pyocyanin (a blue-green pigment) and pyoverdin, giving urine a distinct green color. Often accompanied by cloudy urine and UTI symptoms.
3. Bile Pigments / Hepatobiliary Disease
- Obstructive jaundice (cholestasis) - bilirubin and especially biliverdin (oxidized bilirubin) accumulates and is excreted in urine. In severe chronic obstruction, urine can turn dark green. Shaking the specimen produces a characteristic yellow foam.
- Severe hepatocellular disease
4. Dietary / Dyes
- Food dyes (especially blue and green artificial dyes in drinks, candies, sweets)
- Asparagus - can add a greenish tinge
- Chlorophyll supplements or products (e.g., Clorets gum with actizol)
- Traditional Chinese medicine (some preparations, e.g., Wilisan pills, contain methylene blue)
5. Rare Inherited / Metabolic Conditions
| Condition | Mechanism |
|---|---|
| Hartnup disease | Tryptophan malabsorption; indole derivatives in urine |
| Indicanemia / Indicanuria | Excess indican from tryptophan metabolism in intestinal bacterial overgrowth |
| Familial benign hypercalcemia (Blue Diaper Syndrome) | Children; defective intestinal absorption of tryptophan |
| Porphyrias (rare presentations) | Variable urine discoloration |
6. Structural / Anatomical
- Vesicoenteric fistula - bowel contents (including bile) mix with urine, producing green discoloration
Clinical Approach
| Feature | Suggests |
|---|---|
| Receiving propofol infusion | Propofol-induced (benign, resolves with discontinuation) |
| Yellow foam on shaking urine | Bile pigments (obstructive jaundice) |
| Dysuria + cloudy green urine + febrile | Pseudomonas UTI |
| Recent medication change | Drug-induced (review drug list first) |
| ICU patient on methylene blue | Methylene blue |
| Skin/sclera also blue-green | Mitoxantrone |
| Children + hypercalcemia history | Blue Diaper Syndrome |
In the vast majority of cases, green urine is drug-induced and benign, resolving spontaneously once the offending agent is stopped. Infection and biliary causes require prompt evaluation.
Sources: Henry's Clinical Diagnosis and Management by Laboratory Methods; Roberts and Hedges' Clinical Procedures in Emergency Medicine; Barash's Clinical Anesthesia, 9e; LITFL Green Urine Reference; Mayo Clinic - Urine Color
What is done to rule out hepatobiliary disease or pseudomonas UTI
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
I now have everything needed for a thorough, textbook-backed answer.
Workup to Rule Out Hepatobiliary Disease vs. Pseudomonas UTI
Part 1 - Ruling Out Hepatobiliary Disease
The key principle: green urine from hepatobiliary causes is due to conjugated (direct) hyperbilirubinemia - specifically biliverdin (oxidized bilirubin) appearing in urine. The workup proceeds in layers:
Step 1 - Urine Dipstick
- Urine bilirubin - detects conjugated (direct) bilirubin only. Unconjugated bilirubin is albumin-bound and does not pass into urine. A positive urine bilirubin immediately points to hepatobiliary pathology (cholestasis, hepatocellular disease, or biliary obstruction).
- A simple bedside clue: shaking the urine specimen produces yellow foam (vs. white foam in concentrated normal urine).
Step 2 - Serum Liver Function Tests
| Test | What it Tells You |
|---|---|
| Total + Direct bilirubin | Is it conjugated (hepatic/obstructive) or unconjugated (hemolytic/pre-hepatic)? |
| ALP (Alkaline Phosphatase) | Elevated in cholestasis and biliary obstruction |
| GGT (Gamma-GT) | Confirms ALP elevation is of hepatic origin (vs. bone, placenta) |
| ALT / AST | Elevated in hepatocellular damage (hepatitis pattern) |
| PT / INR | Assesses synthetic function; prolonged = significant liver dysfunction |
| Albumin | Chronic liver disease marker |
The R-value (ALT/ULN ÷ ALP/ULN) distinguishes hepatocellular (R >5) from cholestatic (R <2) injury pattern. - Yamada's Textbook of Gastroenterology, 7e
Step 3 - Fractionated Bilirubin Interpretation
The diagnostic approach to elevated bilirubin is shown below:
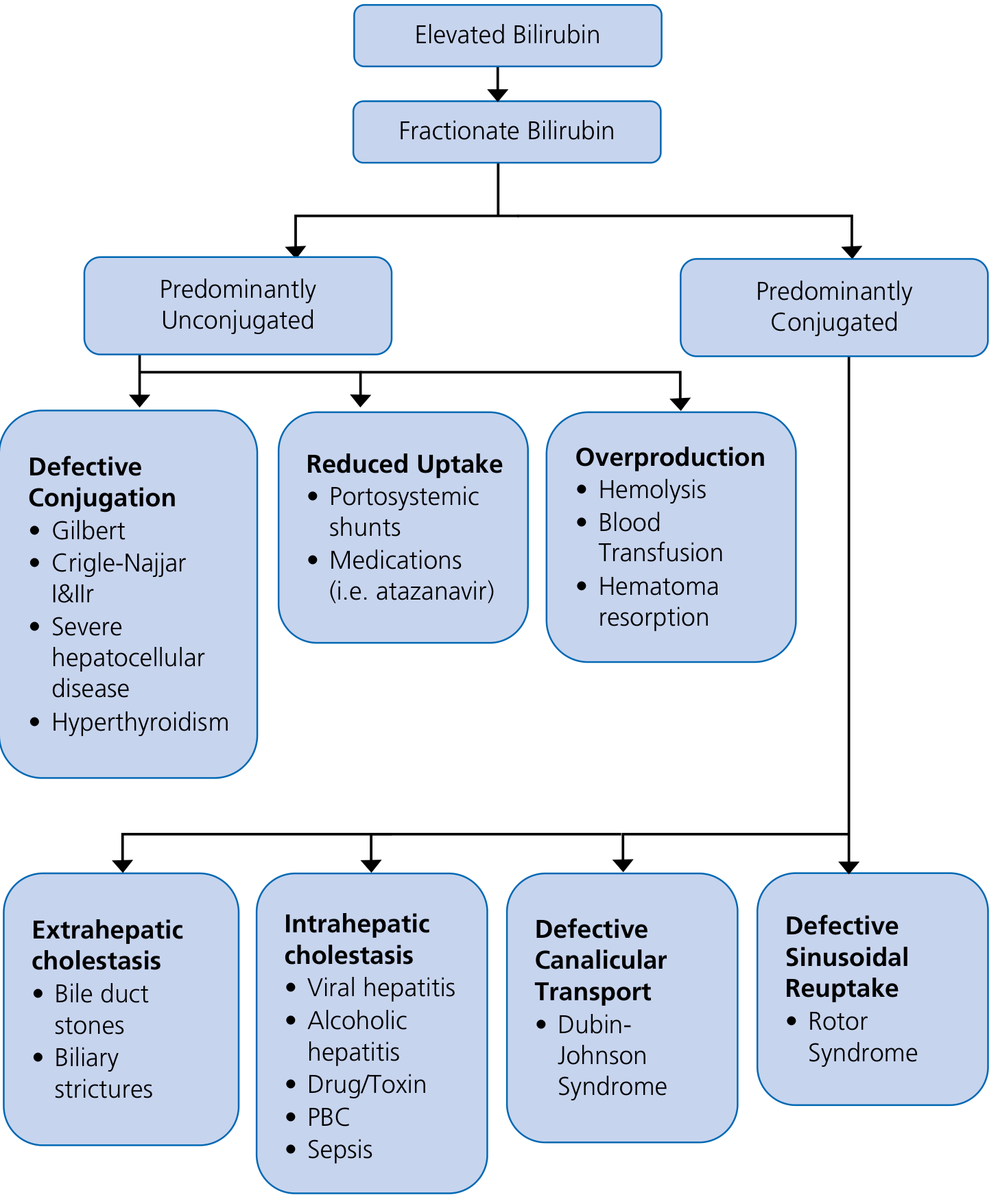
- Predominantly conjugated hyperbilirubinemia narrows to: extrahepatic cholestasis (bile duct stones, strictures), intrahepatic cholestasis (viral hepatitis, alcoholic hepatitis, PBC, drugs/toxins, sepsis), or defective canalicular transport.
- Predominantly unconjugated points away from cholestasis toward hemolysis or conjugation defects. - Yamada's Textbook of Gastroenterology, 7e
Step 4 - Abdominal Imaging
- Abdominal ultrasound is the first-line imaging test - it identifies bile duct dilation (>7 mm = abnormal), gallstones, biliary strictures, and liver parenchymal changes. Note: the bile duct may NOT be dilated early in acute obstruction. - Harrison's Principles of Internal Medicine, 22e
- If ultrasound is inconclusive: MRCP (best non-invasive biliary imaging) or CT abdomen for suspected malignancy/mass.
- ERCP is reserved for cases where therapeutic intervention (stone removal, stenting) is anticipated.
Part 2 - Ruling Out Pseudomonas UTI
Pseudomonas aeruginosa does NOT reduce nitrate to nitrite (it is a gram-negative non-fermenter), so the nitrite dipstick is often negative despite active infection - making culture essential.
Step 1 - Urinalysis with Microscopy
| Finding | Significance |
|---|---|
| Leukocyte esterase positive | Indirect marker of pyuria (WBCs in urine) |
| Nitrite | Usually negative for Pseudomonas (non-fermenter, doesn't reduce nitrate) |
| WBCs on microscopy (>5 WBC/hpf) | Pyuria - supports infection |
| Bacteria on Gram stain | Gram-negative rods = supports Pseudomonas or Enterobacterales |
| Cloudy appearance | Suggests significant bacteriuria/pyuria |
A positive nitrite test makes UTI very likely (specificity 98%), but nitrite testing has insufficient sensitivity alone (53%) and is typically negative in Pseudomonas. - Tintinalli's Emergency Medicine
Step 2 - Urine Culture and Sensitivity (Gold Standard)
This is the definitive test for UTI.
| Collection Method | Positive Threshold |
|---|---|
| Clean catch midstream | ≥ 50,000 cfu/mL |
| Catheter specimen | ≥ 50,000 cfu/mL |
| Suprapubic aspiration | Any single-species growth |
- Culture results must always be interpreted in the context of pyuria - a positive culture without pyuria may represent colonization rather than true infection.
- Sensitivity testing from the culture will also guide antibiotic choice, important because Pseudomonas has intrinsic resistance to many antibiotics. - Tintinalli's Emergency Medicine
Step 3 - Blood Cultures (if systemically unwell)
- If the patient has fever, rigors, hypotension, or other signs of sepsis, add blood cultures to rule out Pseudomonas bacteremia - this is a clinical emergency.
Summary: Quick Differentiation at the Bedside
| Test | Hepatobiliary Disease | Pseudomonas UTI |
|---|---|---|
| Urine dipstick bilirubin | Positive | Negative |
| Urine foam test | Yellow foam | Normal white foam |
| Leukocyte esterase | Negative | Positive |
| Urine nitrite | Negative | Usually Negative (Pseudomonas) |
| Urine microscopy | Normal or bile casts | WBCs + gram-neg rods |
| ALP / GGT | Elevated | Normal |
| Direct bilirubin | Elevated | Normal |
| Urine culture | Sterile | >50,000 cfu/mL Pseudomonas |
Sources: Yamada's Textbook of Gastroenterology, 7e; Tintinalli's Emergency Medicine; Harrison's Principles of Internal Medicine, 22e; Henry's Clinical Diagnosis and Management by Laboratory Methods
This is a shared conversation. Sign in to Orris to start your own chat.